[1]
Yu EY, Ren Z, Mehrkanoon S, Stehouwer CDA, van Greevenbroek MMJ, Eussen SJPM, Zeegers MP, Wesselius A. Plasma metabolomic profiling of dietary patterns associated with glucose metabolism status: The Maastricht Study. BMC medicine. 2022 Nov 21:20(1):450. doi: 10.1186/s12916-022-02653-1. Epub 2022 Nov 21
[PubMed PMID: 36414942]
[2]
Remesar X, Alemany M. Dietary Energy Partition: The Central Role of Glucose. International journal of molecular sciences. 2020 Oct 19:21(20):. doi: 10.3390/ijms21207729. Epub 2020 Oct 19
[PubMed PMID: 33086579]
[3]
Goyal MS, Raichle ME. Glucose Requirements of the Developing Human Brain. Journal of pediatric gastroenterology and nutrition. 2018 Jun:66 Suppl 3(Suppl 3):S46-S49. doi: 10.1097/MPG.0000000000001875. Epub
[PubMed PMID: 29762377]
[4]
Hui S, Ghergurovich JM, Morscher RJ, Jang C, Teng X, Lu W, Esparza LA, Reya T, Le Zhan, Yanxiang Guo J, White E, Rabinowitz JD. Glucose feeds the TCA cycle via circulating lactate. Nature. 2017 Nov 2:551(7678):115-118. doi: 10.1038/nature24057. Epub 2017 Oct 18
[PubMed PMID: 29045397]
[5]
Liu S, Dai Z, Cooper DE, Kirsch DG, Locasale JW. Quantitative Analysis of the Physiological Contributions of Glucose to the TCA Cycle. Cell metabolism. 2020 Oct 6:32(4):619-628.e21. doi: 10.1016/j.cmet.2020.09.005. Epub 2020 Sep 21
[PubMed PMID: 32961109]
[8]
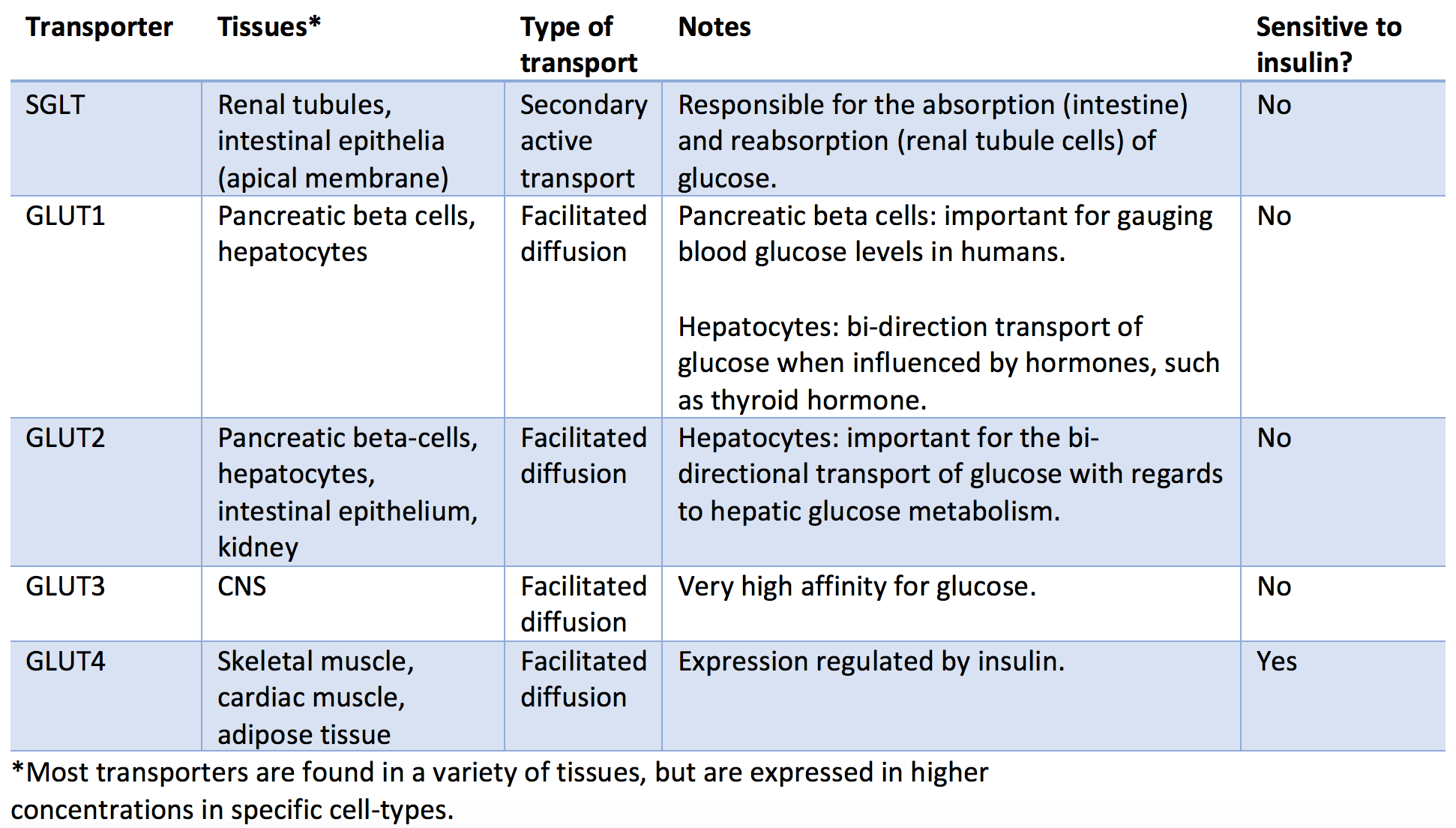
Kellett GL, Brot-Laroche E, Mace OJ, Leturque A. Sugar absorption in the intestine: the role of GLUT2. Annual review of nutrition. 2008:28():35-54. doi: 10.1146/annurev.nutr.28.061807.155518. Epub
[PubMed PMID: 18393659]
[9]
Fazakerley DJ, Koumanov F, Holman GD. GLUT4 On the move. The Biochemical journal. 2022 Feb 11:479(3):445-462. doi: 10.1042/BCJ20210073. Epub
[PubMed PMID: 35147164]
[11]
Navale AM, Paranjape AN. Glucose transporters: physiological and pathological roles. Biophysical reviews. 2016 Mar:8(1):5-9. doi: 10.1007/s12551-015-0186-2. Epub 2016 Jan 19
[PubMed PMID: 28510148]
[12]
Srichaikul K, Jenkins DJA. The Glycemic Index, Rate of Digestion of Carbohydrate Foods, and Their Potential Link with Cardiovascular Disease. The Journal of nutrition. 2022 Apr 1:152(4):920-921. doi: 10.1093/jn/nxab427. Epub
[PubMed PMID: 35174392]
[13]
Jones JG. Hepatic glucose and lipid metabolism. Diabetologia. 2016 Jun:59(6):1098-103. doi: 10.1007/s00125-016-3940-5. Epub 2016 Apr 5
[PubMed PMID: 27048250]
[15]
Vargas E, Joy NV, Carrillo Sepulveda MA. Biochemistry, Insulin Metabolic Effects. StatPearls. 2024 Jan:():
[PubMed PMID: 30252239]
[20]
Christensen MB. Glucose-dependent insulinotropic polypeptide: effects on insulin and glucagon secretion in humans. Danish medical journal. 2016 Apr:63(4):. pii: B5230. Epub
[PubMed PMID: 27034187]
[21]
Kubihal S, Goyal A, Gupta Y, Khadgawat R. Glucose measurement in body fluids: A ready reckoner for clinicians. Diabetes & metabolic syndrome. 2021 Jan-Feb:15(1):45-53. doi: 10.1016/j.dsx.2020.11.021. Epub 2020 Dec 3
[PubMed PMID: 33310176]
[22]
Murray-Bachmann R, Leung TM, Myers AK, Murthi S, Sarbanes M, Ziskovich K, Lesser M, Poretsky L. Reliability of continuous glucose monitoring system in the inpatient setting. Journal of clinical & translational endocrinology. 2021 Sep:25():100262. doi: 10.1016/j.jcte.2021.100262. Epub 2021 Jul 7
[PubMed PMID: 34336598]
[23]
Sung JF, Taslimi MM, Faig JC. Continuous glucose monitoring in pregnancy: new frontiers in clinical applications and research. Journal of diabetes science and technology. 2012 Nov 1:6(6):1478-85
[PubMed PMID: 23294795]
[24]
Chen ME, Aguirre RS, Hannon TS. Methods for Measuring Risk for Type 2 Diabetes in Youth: the Oral Glucose Tolerance Test (OGTT). Current diabetes reports. 2018 Jun 16:18(8):51. doi: 10.1007/s11892-018-1023-3. Epub 2018 Jun 16
[PubMed PMID: 29909550]
[25]
Galant AL, Kaufman RC, Wilson JD. Glucose: Detection and analysis. Food chemistry. 2015 Dec 1:188():149-60. doi: 10.1016/j.foodchem.2015.04.071. Epub 2015 Apr 23
[PubMed PMID: 26041177]
[26]
Khan RMM, Chua ZJY, Tan JC, Yang Y, Liao Z, Zhao Y. From Pre-Diabetes to Diabetes: Diagnosis, Treatments and Translational Research. Medicina (Kaunas, Lithuania). 2019 Aug 29:55(9):. doi: 10.3390/medicina55090546. Epub 2019 Aug 29
[PubMed PMID: 31470636]
[27]
Tonelli J, Kishore P, Lee DE, Hawkins M. The regulation of glucose effectiveness: how glucose modulates its own production. Current opinion in clinical nutrition and metabolic care. 2005 Jul:8(4):450-6
[PubMed PMID: 15930973]
Level 3 (low-level) evidence
[28]
Kishimoto I. Subclinical Reactive Hypoglycemia with Low Glucose Effectiveness-Why We Cannot Stop Snacking despite Gaining Weight. Metabolites. 2023 Jun 15:13(6):. doi: 10.3390/metabo13060754. Epub 2023 Jun 15
[PubMed PMID: 37367911]
[29]
Karakas SE. Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome. Journal of clinical medicine. 2023 Nov 23:12(23):. doi: 10.3390/jcm12237252. Epub 2023 Nov 23
[PubMed PMID: 38068304]
[30]
Chao HW, Chao SW, Lin H, Ku HC, Cheng CF. Homeostasis of Glucose and Lipid in Non-Alcoholic Fatty Liver Disease. International journal of molecular sciences. 2019 Jan 13:20(2):. doi: 10.3390/ijms20020298. Epub 2019 Jan 13
[PubMed PMID: 30642126]
[31]
Harreiter J, Roden M. [Diabetes mellitus: definition, classification, diagnosis, screening and prevention (Update 2023)]. Wiener klinische Wochenschrift. 2023 Jan:135(Suppl 1):7-17. doi: 10.1007/s00508-022-02122-y. Epub 2023 Apr 20
[PubMed PMID: 37101021]
[32]
Nawale RB, Mourya VK, Bhise SB. Non-enzymatic glycation of proteins: a cause for complications in diabetes. Indian journal of biochemistry & biophysics. 2006 Dec:43(6):337-44
[PubMed PMID: 17285797]
[36]
Awosika A, Adabanya U, Millis RM, Omole AE, Moon JH. Postprandial Hypotension: An Underreported Silent Killer in the Aged. Cureus. 2023 Feb:15(2):e35411. doi: 10.7759/cureus.35411. Epub 2023 Feb 24
[PubMed PMID: 36851946]
[37]
Morgan RK, Cortes Y, Murphy L. Pathophysiology and aetiology of hypoglycaemic crises. The Journal of small animal practice. 2018 Nov:59(11):659-669. doi: 10.1111/jsap.12911. Epub 2018 Aug 13
[PubMed PMID: 30102417]
Level 3 (low-level) evidence
[40]
International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. The lancet. Diabetes & endocrinology. 2019 May:7(5):385-396. doi: 10.1016/S2213-8587(18)30315-2. Epub 2019 Mar 27
[PubMed PMID: 30926258]