
Introduction
Trauma to the cervical spine encompasses a broad spectrum of injuries, ranging from muscular strain, capsular or ligament sprain or tear to facet subluxations or dislocations, with or without fractures. Cervical dislocations are severe and complex injuries to the fragile vertebrae and surrounding structures of the neck. Cervical dislocations have classically been associated with traumatic spinal cord injuries. These injuries can cause spinal cord compression and significant neurological deficits. The severity of these injuries depends on various factors, including the force of the injury, the extent of damage to the stabilizing osseous and soft tissue structures of the cervical spine, patient age, syndromic issues, bone quality, and underlying comorbidities.[1]
Cervical dislocations involve the abnormal displacement or misalignment of the cervical spine, which consists of 7 vertebral bodies. The C1 (atlas) articulates with the occiput, while the C2 (axis) is considered the axial spine. Vertebrae C3 through C7 are considered the subaxial spine. In addition, the cervical spine has a resting lordotic curve from C3 to C7. These structures provide physiological motion and protect neural elements.
The spine can be divided into 3 distinct columns, each contributing to cervical stability.[2] The anterior column consists of the anterior longitudinal ligament and the anterior two-thirds of the vertebral body and disk. The middle column consists of the posterior longitudinal ligament, the posterior one-third of the vertebral body and disk, and the posterior vertebral body wall. The posterior column comprises the pedicles, lamina, spinous process, and the posterior ligamentous complex. The posterior ligamentous complex is considered a critical predictor of spinal stability and includes the ligamentum flavum, facet joint or capsule, interspinous ligament, and supraspinous ligament.[2] In the event of trauma, the stability of the cervical spine and the required treatment will depend on the extent of injury to the osseous and soft tissue structures.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Cervical dislocations exhibit a bimodal distribution, and the mechanism of injury varies by patient's age. Traumatic incidents such as high-impact collisions, falls, or sports-related accidents can commonly cause cervical dislocations, often leading to significant impairment of motor and sensory functions. Younger patients are typically associated with high-velocity injury mechanisms, such as motor vehicle collisions, whereas older patients more commonly experience low-velocity injury mechanisms, such as ground-level falls.[1][2]
Facet joint dislocations can be purely ligamentous or accompanied by a fracture, depending on the mechanism of injury. They are typically caused by a flexion-distraction event at the time of injury and are located in the subaxial spine.[3] Hyperflexion generates a distraction force that causes the posterior osseous and ligamentous structures to fail under tension, while a rotational or shear force can result in fracture or dislocation.[3]
Epidemiology
Cervical dislocations can occur in 2 locations—axial, consisting of the occipitocervical (occiput/C1) and atlantoaxial (C1/C2) articulations, and subaxial, which ranges from C2/C3 to C7/T1. Acquired instability causing dislocations can occur in the axial spine and is seen in the pediatric population. However, the majority of these dislocations are secondary to traumatic events, with about 75% occurring in the subaxial spine.[1][4] Most subaxial dislocations are associated with males.
Special consideration should be given to the pediatric population in the setting of cervical trauma due to the increased likelihood of spinal cord injury and lethality. Children aged 8 or younger are more susceptible to cervical spine injuries due to their larger head size, weaker muscles, and increased ligamentous laxity.
The key predictors indicating a cervical fracture in a polytrauma patient include the following: [5]
- Pelvic fracture
- Pelvic fracture combined with a fall and/or concurrent head injury
- Injury severity score greater than 15
- Age 40 or older
Pathophysiology
Axial cervical dislocations can result from either atraumatic or traumatic etiologies. Atraumatic or acquired occipitocervical instability is typically seen in patients with Down syndrome and is rarely symptomatic. Traumatic occipitocervical dislocation is a severe injury, often fatal, due to brainstem destruction. Atlantoaxial dislocation can occur due to degenerative conditions, such as rheumatoid arthritis or Down syndrome, or from trauma, such as odontoid fractures (C2), atlas fractures (C1), or transverse ligament injury.
In the context of trauma, cervical dislocations can result in compression and injury to the spinal cord. The primary injury to the cord occurs due to direct trauma, damaging neural tissue. However, secondary injury to the spinal cord can be equally or more critical than the initial trauma. This secondary trauma arises from injury to adjacent tissues and structures, leading to an abundant inflammatory response characterized by reduced local perfusion, cytokine release, apoptosis, lipid peroxidation, and hematoma formation.
Steroids are administered to mitigate this secondary injury by improving perfusion and reducing free radical formation, thereby decreasing inflammation. Clinicians should be vigilant for 2 common conditions associated with acute spinal cord injury—spinal shock and neurogenic shock. Neurogenic shock can induce bradycardia and hypotension due to reduced sympathetic outflow, exacerbating spinal cord injury by causing hypoperfusion (see Image. Cord Compression Following Cervical Spine Injury).[6]
Classification Systems
Allen and Ferguson Classification (1982): Allen and Ferguson described 6 common patterns of indirect injury to the subaxial cervical spine (phylogenies) based on radiographic images and associated traumatic forces (flexion/extension/compression/distraction):
- Flexion and compression
- Vertical compression
- Flexion and distraction (facet joint dislocation)
- Extension and compression
- Extension and distraction
- Lateral flexion
Magerl Classification (1990): This system categorizes injuries based on pathomorphological characteristics, emphasizing the involvement and extent of the anterior and posterior elements, with specific attention to soft-tissue injuries and ancillary bony lesions.
The classification includes the following 3 main types of injuries:
- Type A injuries: Primarily caused by compression
- Type B injuries: Primarily caused by tension
- Type C injuries: Primarily caused by axial torque corresponding to an increasing degree of injury instability
Subaxial Injury Classification (SLIC, 2007): This classification considers 3 critical factors, including injury morphology, disco-ligamentous complex integrity, and neurological status. A score is assigned based on the overall severity of the injury.
| Injuries | Scores |
| Morphological features | |
| No morphological abnormality | 0 |
| Compression | 1 |
| Burst | 2 |
|
Distraction |
3 |
| Rotational and/or translational | 4 |
| Disco-ligamentous complex integrity | |
| Intact | 0 |
| Indeterminate | 1 |
| Disrupted | 2 |
| Patient’s neurological status | |
| Intact | 0 |
| Nerve root injury | 1 |
| Complete | 2 |
| Incomplete | 3 |
| Persistent cord compression (in the setting of a neurological deficit) | +1 |
| Total SLIC Score | 0-10 |
Notably, the SLIC score summarizes as mentioned below.
Scores 1 to 3: Nonsurgical management
Score 4: Surgical or nonsurgical treatment
Scores 5 to 10: Surgical management
AO Spine Subaxial Cervical Spine Injury Classification System (2013): The classification system categorizes injuries based on the below-mentioned criteria.
- Morphology of the injury
- Facet injury
- Neurological status
- Any case-specific modifiers
This classification includes the following 3 main types of injuries:
- Type A injuries: Result from vertebral compression with intact tension band.
- Type B injuries: Result in the failure of the posterior or anterior tension band due to distraction forces without translation or dislocation.
- Type C injuries: Injuries displacement or translation of a vertebral body relative to another, occurring in various directions—anterior, posterior, lateral translation, or vertical distraction.
Type C injuries are classical cervical dislocations. Type B injuries with a translation component are automatically classified as type C.
Cervical spondyloptosis refers to a condition where a vertebral body is completely displaced anteriorly or posteriorly over another vertebral body (see Image. Traumatic Cervical Spondyloptosis of the C6-C7 Segments).
AO Spine Upper Cervical Spine Fracture Classification: Type C injuries in this classification encompass injuries at the occipital condyle or craniocervical junction with displacement on spinal imaging, atlantoaxial instability or translation in any plane, and injuries at the C2 or C2-C3 joint resulting in vertebral body translation in any directional plane. These injuries may also be classified as cervical dislocations.
History and Physical
The key to proper treatment of cervical spine trauma is early diagnosis and management. Unfortunately, in cases of blunt trauma, relying solely on a physical exam is unreliable for diagnosing or ruling out cervical spine injury.[7] Therefore, it is crucial to have a thorough understanding of the mechanism of injury, perform a neurological examination, and obtain appropriate imaging. When trauma to the head and neck is suspected, immobilization of the cervical spine is essential to prevent the risk of secondary injury to the spinal cord.[8] This immobilization is achieved using a rigid cervical collar, positioning the neck in a neutral alignment (see Image. Cervical Collar).
In the setting of any trauma evaluation, before proceeding with clinical and radiologic assessments, the patient must undergo a primary survey following Advanced Trauma Life Support (ATLS) protocols. The initial steps include assessing the airway and protecting the cervical spine, followed by supporting breathing, ensuring circulation, assessing neurological status, and exposing the patient to a comprehensive examination. Once the patient is stabilized, a secondary survey can be conducted. This involves obtaining a detailed history and performing a thorough physical examination to ascertain the mechanism of injury, identify any medical comorbidities that may increase the risk of spinal injury, and determine any other axial injuries of the spinal column or distracting injuries in the extremities.
Upon presentation, a thorough neurological examination is crucial to establish and document the patient's baseline. Periodic reassessments should be conducted and compared to the initial baseline to evaluate any changes, whether improvement or deterioration. The American Spinal Injury Association (ASIA) spine exam is traditionally used to assess neurological status, focusing on key motor groups, sensory function, digital rectal examination, and reflexes (see Image. ASIA Spinal Cord Injury Scoring Sheet).
Patients with cervical spine trauma may present with unilateral upper extremity symptoms indicative of nerve root injury or bilateral upper and lower extremity symptoms suggestive of spinal cord injury. Before performing an accurate ASIA exam, it is essential to ascertain whether the patient is in spinal shock. Spinal shock is characterized by a temporary loss of spinal cord function and reflex activity below the level of the spinal cord injury.[9] The presence of the bulbocavernosus reflex is initially evaluated to assess spinal shock. This reflex involves anal sphincter contraction when squeezing the glans penis in males or clitoris in females or by tugging on the Foley catheter. The absence of this reflex indicates that the patient is experiencing spinal shock, which typically lasts from 24 to 72 hours. An accurate neurological examination can be obtained once the patient is no longer in spinal shock.[10][11]
Key Examination Findings
The key examination findings associated with neurological injury are mentioned below.
- Occiput/C1: The occiput is closely related to the lower cranial nerves.
- Cranial nerves IX (glossopharyngeal nerve) and X (vagus nerve): When evaluating these nerves, the examiner should test the gag response and observe any uvula deviation away from the affected side.
- Cranial nerve XI (spinal accessory nerve): This nerve should be evaluated for its function in shrugging the shoulders (trapezius innervation) and turning the head from side to side (sternocleidomastoid).
- Cranial nerve XII (hypoglossal nerve): This nerve should be tested for its ability to protrude the tongue and move it from side to side while also observing for any fasciculations.
- C4: Injury to this nerve root can result in deficits in scapular stabilization, leading to scapular winging, as it primarily innervates the serratus anterior muscle.
- C5: Injury to this nerve root can cause deficits in shoulder abduction and elbow flexion (palm up), affecting the deltoid and biceps muscles. Additionally, there may be sensory deficits in the lateral arm and below the deltoid, along with an abnormal biceps reflex.
- C6: Injury to this nerve root can lead to deficits in elbow flexion (thumbs up) and wrist extension, primarily affecting the brachioradialis and extensor carpi radialis longus muscles. Sensory deficits may also be present in the thumb and radial hand, accompanied by an abnormal brachioradialis reflex.
- C7: Injury to this nerve root can result in deficits in elbow extension and wrist flexion, affecting the triceps and flexor carpi radialis muscles. Sensory deficits may occur in fingers 2, 3, and 4, with an abnormal triceps reflex.
- C8: Injury to this nerve root can cause deficits in finger flexion, handgrip, and thumb extension, primarily affecting the flexor digitorum superficialis, flexor digitorum profundus, and extensor pollicis longus muscles. Sensory deficits typically involve the small finger.
- T1: Injury to this nerve root can lead to deficits in finger abduction, affecting the hand interossei muscles. Sensory deficits in the medial elbow region may also be present.
Evaluation
The standard imaging protocol consists of plain radiographs, computed tomography (CT) scans, and magnetic resonance imaging (MRI) scans. During a standard trauma evaluation, 3 views—anteroposterior, lateral, and open-mouth odontoid plain films—are used. These plain films must include the entire cervical spine, especially the C7-T1 junction, as up to 17% of cervical spine injuries occur at this location, making it crucial to visualize T1 when assessing cervical trauma.[12] Therefore, if T1 is not visible on the standard 3-view series, a swimmer's view can be obtained to assess the cervical alignment on the lateral radiograph.
Signs of cervical facet dislocation can include vertebral body subluxation compared to the vertebral body below. This is observable with reversal or loss of the normal cervical lordosis using the 4 parallel lines of the cervical spine. Unilateral facet dislocation can lead to about 25% subluxation, while bilateral facet dislocation can result in about 50% subluxation. Loss of disk height may indicate a retropulsed disk in the canal. CT scans are rapidly becoming the standard of care for imaging in initial trauma evaluations due to their superior sensitivity and ability to better assess osseous anatomy compared to x-rays, particularly at the cervical-thoracic junction (C7/T1).[13]
Specific Radiographic Features
Specific radiographic features seen on CT that could indicate cervical instability and dislocations include the areas mentioned below.
Axial spine:
- The alignment of the occipitocervical joint in case of dislocation can be measured by the "power ratio." The power ratio is frequently used to determine instability and is calculated by measuring distances.
- The equation is as follows: Power ratio = Basion to posterior arch/Anterior arch to opisthion
- A ratio of approximately 1 is considered normal, greater than 1 indicates anterior dislocation, and less than 1 is considered posterior dislocation.
- Another commonly used measurement is the Harris rule of 12. This is the distance from the basion to the tip of the dens; greater than 12 mm suggests occipitocervical dissociation.
Subaxial spine:
- Facet dislocations are best appreciated in the sagittal plane. Notably, it is key to examine the sagittal CT scan to examine the mid-sagittal and parasagittal cascade of the anterior vertebral column, posterior vertebral column, spinolaminar line, and interspinous line. These lines should be smooth and continuous. In the axial plane, the facet joints resemble hamburger buns, with the flat portions articulating.
- Signs of dislocation can include facet joint diastasis or dislocation and translation of the vertebral body compared to vertebrae below on the sagittal plane. The naked facet sign (also known as the hamburger sign or reverse hamburger bun sign) is seen on the axial plane when a locked facet results from facet joint dislocation.[14] This indicates spinal instability, where the superior articular process is the bun on the top of the patty, the facet joint space is the hamburger, and the inferior articular process is the bun beneath the patty.
MRI scans are highly sensitive in detecting disk herniations and injuries to the spinal cord, nerve roots, and the posterior ligamentous complex. However, they are less accurate than CT scans in assessing osseous anatomy. Therefore, an MRI scan is recommended only for patients with an abnormal neurological exam or in unconscious or intoxicated patients where a spinal cord injury is suspected.
Treatment / Management
The initial step in management is to accurately classify the injury according to the preferred classification system, assess the severity of the lesions, and differentiate between surgical and nonsurgical approaches for cervical trauma.
Timing
Previously, timing was considered a significant factor for neurological recovery following spine trauma. However, its impact remains debated. Current evidence does not show statistical differences in neurological outcomes between early and late surgical interventions for spinal cord injury. Based on the available literature, performing surgery within 72 hours of trauma, contingent upon general conditions and comorbidities, appears reasonable.
Conservative Treatment
A cervical orthosis is indicated only for cervical facet fractures without significant subluxation, dislocation, or kyphosis or in patients who are poor candidates for surgery. Typically, these injuries result from trauma and often require some form of operative stabilization.
Historically, high-dose methylprednisolone (30 mg/kg bolus, followed by 5.4 mg/kg infusion) within 8 hours of injury was the standard of care for acute spinal cord injury, based on the National Acute Spinal Cord Injury Studies (NASCIS). However, recent evidence suggests that high-dose steroids may increase the risk of respiratory infections and gastrointestinal hemorrhage. Steroids are still used in cervical trauma, primarily for medicolegal reasons and at significantly lower doses.
Unilateral or bilateral facet dislocations are almost always treated with surgical management. The posterior ligamentous complex must be injured for the facets to dislocate, and instrumentation is required to stabilize the spine. Typically, stabilization involves instrumentation at least 1 level above and below the injury levels. However, a longer fusion construct may be recommended for adequate stabilization in cases involving multiple levels.[15][16]
Operative Treatments
Immediate closed reduction, followed by MRI and surgical stabilization:
- This procedure is indicated for awake and cooperative patients presenting with unilateral or bilateral facet dislocation and neurological deficits.
- The procedure involves inserting cranial tongs for axial traction with added weights.
- Traction weight varies based on patient size and the extent of dislocation, typically starting with 10 lbs (head weight) plus an additional 5 lbs per level.
- Cervical flexion and rotation are incorporated to assist in reduction. For instance, a C6 dislocation might require approximately 40 lbs (10 lbs for the head + 30 lbs for the C6 level).
Additional weight is incrementally added up to a maximum of 100 lbs, with serial neurological exams and plain lateral radiographs conducted after each increment. If the neurological exam deteriorates, all weights are promptly removed, and an emergent MRI must be performed. An MRI should always be obtained after reduction to determine the optimal approach for surgical stabilization.
Immediate MRI, followed by open reduction and surgical stabilization: This procedure is indicated for patients with facet dislocations accompanied by mental status changes or uncooperative patients, as well as those who fail closed reduction.
Anterior open reduction and anterior cervical decompression and fusion:
- These procedures are indicated when an MRI demonstrates cervical disk herniation with significant anterior spinal cord compression.
- Open reduction is performed using Caspar pins to distract vertebral bodies and add rotation.
- While effective for unilateral facet dislocations, it is less effective in reducing bilateral facet dislocations.
Posterior reduction and instrumented stabilization:
- These procedures are indicated when closed or anterior approaches fail, and there is no anterior spinal cord compression from a herniated cervical disk.
- The posterior approach becomes necessary in cases of a locked (irreducible) cervical facet dislocation due to a late or incorrect diagnosis or if both open and closed reduction attempts have failed.
- Traditionally, this procedure has been conducted using lateral mass screws. However, advancements in neuronavigation have led to an increasing preference for pedicle screws due to their enhanced stability.
Combined anterior decompression and posterior reduction or stabilization:
- This approach is indicated when cervical disk herniation is present that requires decompression in a patient, and reduction cannot be achieved through closed or open anterior technique.
- The procedure begins with an anterior approach for diskectomy and decompression, followed by a posterior approach for reduction and instrumentation.
- Bilateral facet dislocation indicates performing a combined anterior and posterior approach, either in a single phase or, if not feasible, in 2 phases. When conducted in 2 phases, initiating with posterior fixation is typically preferred (see Image. Bilateral Facet Fracture Dislocation of the Cervical Spine).
Management of Associated Conditions
Deep venous thrombosis prophylaxis:
- Patients are at high risk for deep venous thrombosis.
- Compression devices should be immediately applied, and chemical prophylaxis should be initiated within 72 hours if the operating surgeon considers it safe.
Cardiopulmonary management:
- Hypotension should be avoided to prevent hypoperfusion to the spinal cord.
- Sinus bradycardia, the most common dysrhythmia occurring in the acute phase following spinal cord injury, can be managed with β2-adrenergic agonists (such as salbutamol), chronotropic agents (such as atropine and adrenaline), or phosphodiesterase inhibitors (such as aminophylline and theophylline).
- Early tracheostomy is recommended for mechanical ventilation in the acute phase of high spinal cord injury care. Both open and percutaneous tracheostomies can be performed soon after anterior cervical spinal surgery without increasing the risk of infection.
Pain management: Proper analgesia should be administered to prevent symptoms of pain-induced dysautonomia.
Autonomic dysreflexia management: The management involves positioning the patient upright, removing tight-fitting clothing, identifying and addressing the triggering stimulus, and administering quick-onset, short-acting antihypertensive medications to lower blood pressure promptly.
Bladder and bowel care: Bladder and bowel care are essential in managing acute spinal cord injury. Initiating a bowel management program for all patients is crucial. Bladder management focuses on preserving upper urinary tract structures and reducing the incidence of urinary tract infections.
Mobilization
Mobilization through physical and occupational therapies should commence within the first week following acute spinal cord injury once the patient is medically optimized, even if they require sedation, vasoactive support, or mechanical ventilation.
Differential Diagnosis
When evaluating cervical dislocations, clinicians must consider a differential diagnosis that encompasses a spectrum of spinal injuries. This evaluative approach aids in accurately identifying the specific pathology and guiding appropriate treatment interventions. The differential diagnoses for cervical dislocations include:
- Blunt neck trauma
- Cervical fractures
- Jefferson
- Hangman
- Burst
- Injuries to the spinous and transverse processes
- Cervical strain
- Penetrating neck trauma
- Spinal cord infarct
- Hypovolemic shock
Prognosis
Complete spinal cord injuries typically show improvement by 1 ASIA grade in about 80% of patients, by 2 grades in about 20% of patients, and result in complete recovery in about 1% of patients at the time of hospital diagnosis.[17] Prognosis primarily depends on neurological status at first presentation and time to surgical decompression and stabilization.[18]
Examples of the level of complete injury and corresponding functional statuses are mentioned below.
- C1 to C4: Patients are ventilator-dependent and require an electric wheelchair operated by head and chin control.
- C5: Patients are ventilator-independent, have function in the biceps and deltoid muscles allowing for elbow flexion, but lack wrist supination and extension (unable to feed themselves). They use an electric wheelchair with hand control and can perform independent activities of daily living.
- C6/C7: Patients have the ability to bring their hand to their mouth due to intact wrist extension and supination (able to feed themselves). They live independently, use a manual wheelchair, and can drive using manual controls.
- C8/T1: Patients show improved hand and finger strength and dexterity, enabling independent transfers.
Complications
Complications associated with cervical dislocations, whether treated surgically or nonsurgically, can be severe and multifaceted.
Complications Following Surgical Intervention
Complications from surgical interventions include:[19]
- Infection
- Vertebral artery and carotid injury
- Dysphagia
- Recurrent laryngeal, superior laryngeal, and hypoglossal nerve injuries
- Horner syndrome
- Pseudoarthrosis
- Adjacent segment disease
Other Complications
- Skin problems: Skin issues typically occur in tetraplegic or quadriplegic patients. Treatment focuses on prevention, skincare, and frequent repositioning.
- Major depressive disorder: This disorder is common in patients following spinal cord injury and can be associated with suicidal ideations. Education and proactive treatment are essential in both acute and chronic settings.
- Venous thromboembolism: This condition arises from venous stasis. Risk can be reduced with immediate anticoagulation, sequential compressive devices, and early ambulation when feasible.
- Urosepsis: This sepsis is common among patients with loss of bladder control. Strict adherence to aseptic technique during catheterization is crucial to reducing its occurrence. Notably, it is important to prevent bladder overdistension, as this significantly increases the risk of urinary tract infections.
Postoperative and Rehabilitation Care
Postoperative and rehabilitation care in cervical dislocations have a pivotal role in optimizing patient recovery and functional outcomes. After surgical intervention to stabilize the cervical spine, patients need vigilant monitoring in the immediate postoperative period to evaluate neurological status, control pain, and mitigate risks such as infection or implant failure. Subsequently, rehabilitation focuses on restoring mobility, strength, and proprioception through a customized regimen of physical and occupational therapies, as well as therapeutic exercises. Gradual increase in activity levels is emphasized while maintaining proper alignment and spinal stability. Patient education on proper body mechanics, ergonomic principles, and injury prevention strategies is also essential for long-term spinal health and reducing the risk of recurrent injuries. Close collaboration among healthcare providers, including surgeons, therapists, and primary care physicians, is crucial for comprehensive care and supporting patients in achieving their functional goals.
Deterrence and Patient Education
Deterrence and patient education are crucial in mitigating the risk of cervical dislocations and promoting spinal health. Patients should receive information about the mechanisms of cervical spine injuries, with a focus on practicing safe behaviors such as using seat belts in vehicles, wearing protective gear during sports, and avoiding risky maneuvers that may cause falls or collisions. Education on proper lifting techniques, maintaining good posture, and ergonomic principles can also help minimize strain on the cervical spine and reduce the risk of injury. Furthermore, patients should be educated about the signs and symptoms of cervical dislocations, emphasizing the importance of seeking prompt medical evaluation after trauma or suspected spinal injury. By empowering patients with knowledge and preventive strategies, healthcare professionals can significantly contribute to reducing the incidence of cervical dislocations and promoting spinal wellness.
Patients with cervical dislocation may receive a referral from their clinician to see a physical therapist who will develop a personalized cervical spine rehabilitation program. The physical therapist will evaluate the patient's condition to determine the most effective strategies for pain relief and improving cervical mobility. Additionally, patients will receive counseling on cervical spine care to manage pain and prevent further injury. The patient has a crucial role in their recovery. At-home practices such as using ice and heat therapy, performing stretching and strengthening exercises, and undergoing posture training are essential. These efforts reduce strain on the affected area and contribute significantly to preventing future recurrence.
Enhancing Healthcare Team Outcomes
The management of cervical dislocations is challenging and complex, which requires proper diagnosis and treatment from an interprofessional team of healthcare professionals. This team includes emergency room physicians, advanced care practitioners, nurses, radiologists, neurosurgeons or orthopedic spine surgeons, and other specialists. Without timely and appropriate management, the morbidity and mortality rates for patients with cervical dislocations can be significant. Upon arrival of a patient with suspected cervical trauma, the emergency room physician assumes responsibility for coordinating care, which involves:
- Immobilizing the cervical spine with a rigid collar in a neutral position.
- Performing ATLS protocols in unstable patients.
- Monitoring the patient for signs and symptoms of mental status change, respiratory depression, and neurological decline.
- Monitoring for hypotension and bradycardia associated with neurogenic shock.
- Obtaining proper initial imaging of the cervical spine.
- Consulting with a neurosurgeon or orthopedic spine surgeon.
If the patient presents with spinal cord injury and neurological deficits, early intervention with reduction, decompression, and/or stabilization leads to improved outcomes. In the postoperative phase, the roles of a nurse, physical or occupational therapist, and social work teams are crucial. Nurses monitor the patient's neurological status, pain, and wound drainage, as well as facilitate frequent offloading to prevent pressure ulcers. Physical and occupational therapists focus on early ambulation, range of motion exercises, strength training, gait training, and activities of daily living. Social workers help to arrange and coordinate the patient's needs relating to equipment and physical therapy at home or a rehabilitation facility. Furthermore, consulting with a psychiatrist and psychologist can assist in diagnosing and preventing mental health disorders associated with these patients. Collaboration among interprofessional healthcare teams enhances patient-centered care, optimizes outcomes, ensures patient safety, and promotes team performance in managing cervical dislocations.[3]
Media
(Click Image to Enlarge)
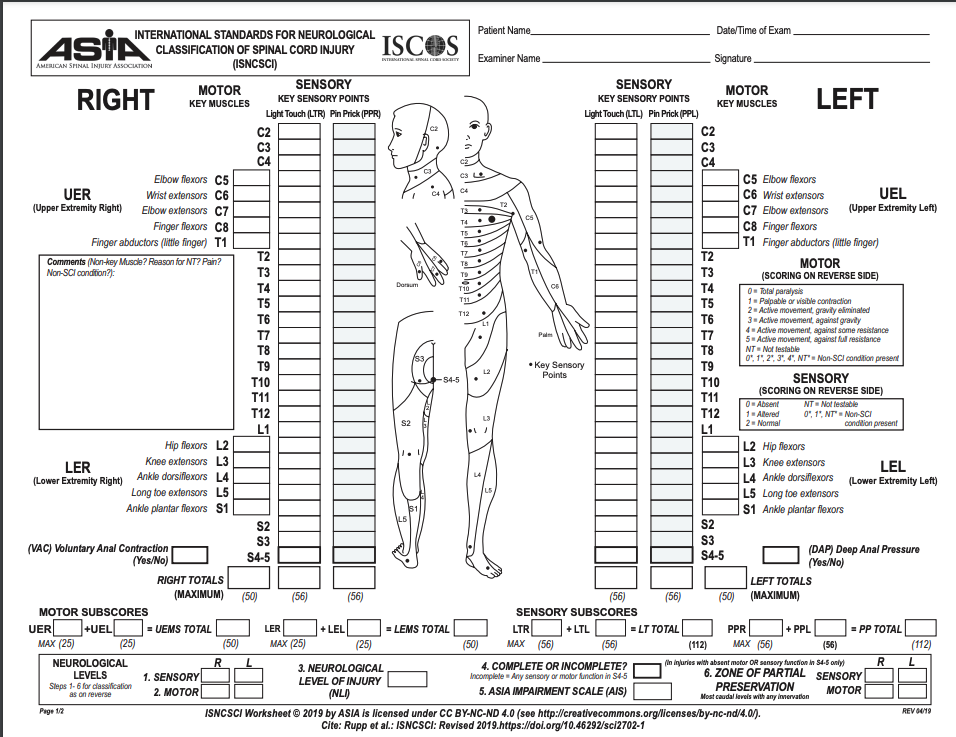
ASIA Spinal Cord Injury Scoring Sheet. The ASIA scoring sheet is useful for physical examination and assessment of all patients suspected of spinal cord injury.
American Spinal Cord Injury Association
(Click Image to Enlarge)

Cervical Collar
Contributed by S Bhimji, MD
(Click Image to Enlarge)

Bilateral Facet Fracture Dislocation of the Cervical Spine
Contributed by C DiPompeo, MD
(Click Image to Enlarge)

Traumatic Cervical Spondyloptosis of the C6-C7 Segments.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
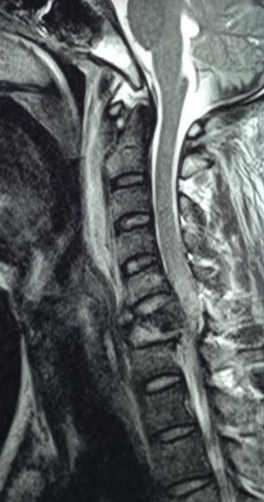
Cord Compression Following Cervical Spine Injury
Contributed by S Munakomi, MD
References
Lowery DW, Wald MM, Browne BJ, Tigges S, Hoffman JR, Mower WR, NEXUS Group. Epidemiology of cervical spine injury victims. Annals of emergency medicine. 2001 Jul:38(1):12-6 [PubMed PMID: 11423805]
Chen Y, He Y, DeVivo MJ. Changing Demographics and Injury Profile of New Traumatic Spinal Cord Injuries in the United States, 1972-2014. Archives of physical medicine and rehabilitation. 2016 Oct:97(10):1610-9. doi: 10.1016/j.apmr.2016.03.017. Epub 2016 Apr 22 [PubMed PMID: 27109331]
Zaveri G, Das G. Management of Sub-axial Cervical Spine Injuries. Indian journal of orthopaedics. 2017 Nov-Dec:51(6):633-652. doi: 10.4103/ortho.IJOrtho_192_16. Epub [PubMed PMID: 29200479]
Raniga SB, Menon V, Al Muzahmi KS, Butt S. MDCT of acute subaxial cervical spine trauma: a mechanism-based approach. Insights into imaging. 2014 Jun:5(3):321-38. doi: 10.1007/s13244-014-0311-y. Epub 2014 Feb 21 [PubMed PMID: 24554380]
Clayton JL, Harris MB, Weintraub SL, Marr AB, Timmer J, Stuke LE, McSwain NE, Duchesne JC, Hunt JP. Risk factors for cervical spine injury. Injury. 2012 Apr:43(4):431-5. doi: 10.1016/j.injury.2011.06.022. Epub 2011 Jul 2 [PubMed PMID: 21726860]
Hodler J, Kubik-Huch RA, von Schulthess GK, Chang CY, Pathria MN. Spine Trauma. Musculoskeletal Diseases 2021-2024: Diagnostic Imaging. 2021:(): [PubMed PMID: 33950617]
Duane TM, Dechert T, Wolfe LG, Aboutanos MB, Malhotra AK, Ivatury RR. Clinical examination and its reliability in identifying cervical spine fractures. The Journal of trauma. 2007 Jun:62(6):1405-8; discussion 1408-10 [PubMed PMID: 17563656]
Prasad VS, Schwartz A, Bhutani R, Sharkey PW, Schwartz ML. Characteristics of injuries to the cervical spine and spinal cord in polytrauma patient population: experience from a regional trauma unit. Spinal cord. 1999 Aug:37(8):560-8 [PubMed PMID: 10455532]
Level 2 (mid-level) evidenceZiu E, Weisbrod LJ, Mesfin FB. Spinal Shock. StatPearls. 2024 Jan:(): [PubMed PMID: 28846241]
Gómez-Flores G, Gutiérrez-Herrera LE, Dufoo-Olvera M, Ladewig-Bernáldez GI, Collado-Arce MGL, Oropeza-Oropeza E, López-Palacios JJ, García-López O, May-Martínez ED, Pérez-Jacobo G, Silvas-Vásquez MR. [Traumatic spondyloptosis C7-T1 without neurologic deficit]. Acta ortopedica mexicana. 2020 Nov-Dec:34(6):412-416 [PubMed PMID: 34020522]
Slocum C, Shea C, Goldstein R, Zafonte R. Early Trauma Indicators and Rehabilitation Outcomes in Traumatic Spinal Cord Injury. Topics in spinal cord injury rehabilitation. 2020:26(4):253-260. doi: 10.46292/sci20-00017. Epub 2021 Jan 20 [PubMed PMID: 33536730]
Goldberg W, Mueller C, Panacek E, Tigges S, Hoffman JR, Mower WR, NEXUS Group. Distribution and patterns of blunt traumatic cervical spine injury. Annals of emergency medicine. 2001 Jul:38(1):17-21 [PubMed PMID: 11423806]
Cabrera JP, Yurac R, Joaquim AF, Guiroy A, Carazzo CA, Zamorano JJ, Valacco M, AO Spine Latin America Trauma Study Group. CT Scan in Subaxial Cervical Facet Injury: Is It Enough for Decision-Making? Global spine journal. 2023 Mar:13(2):344-352. doi: 10.1177/2192568221995491. Epub 2021 Mar 17 [PubMed PMID: 33729870]
Daffner SD, Daffner RH. Computed tomography diagnosis of facet dislocations: the "hamburger bun" and "reverse hamburger bun" signs. The Journal of emergency medicine. 2002 Nov:23(4):387-94 [PubMed PMID: 12480021]
Ifthekar S, Ahuja K, Mittal S, Sarkar B, Deep G, Thomas W, Kandwal P. Management of Neglected Upper Cervical Spine Injuries. Indian journal of orthopaedics. 2021 Jun:55(3):673-679. doi: 10.1007/s43465-020-00227-y. Epub 2020 Aug 13 [PubMed PMID: 33995872]
Mubark I, Abouelela A, Hassan M, Genena A, Ashwood N. Sub-Axial Cervical Facet Dislocation: A Review of Current Concepts. Cureus. 2021 Jan 8:13(1):e12581. doi: 10.7759/cureus.12581. Epub 2021 Jan 8 [PubMed PMID: 33575145]
Scivoletto G, Tamburella F, Laurenza L, Torre M, Molinari M. Who is going to walk? A review of the factors influencing walking recovery after spinal cord injury. Frontiers in human neuroscience. 2014:8():141. doi: 10.3389/fnhum.2014.00141. Epub 2014 Mar 13 [PubMed PMID: 24659962]
Cao BH, Wu ZM, Liang JW. Risk Factors for Poor Prognosis of Cervical Spinal Cord Injury with Subaxial Cervical Spine Fracture-Dislocation After Surgical Treatment: A CONSORT Study. Medical science monitor : international medical journal of experimental and clinical research. 2019 Mar 16:25():1970-1975. doi: 10.12659/MSM.915700. Epub 2019 Mar 16 [PubMed PMID: 30877267]
Cheung JP, Luk KD. Complications of Anterior and Posterior Cervical Spine Surgery. Asian spine journal. 2016 Apr:10(2):385-400. doi: 10.4184/asj.2016.10.2.385. Epub 2016 Apr 15 [PubMed PMID: 27114784]