
 Debriefing Techniques Utilized in Medical Simulation
Debriefing Techniques Utilized in Medical Simulation
Introduction
Simulation-based education (SBE), when used under the right conditions, correlates with significant effects on knowledge, skills, and behaviors and moderate effects on patient-related outcomes. Post-simulation debriefing is 1 of the most effective components of SBE and the cornerstone of the learning experience in the medical simulation setting.[1][2] Debriefing is the intentional discussion following the simulation experience that allows participants to understand their actions clearly and thought processes to promote learning outcomes and enhance future clinical performance.[2][3] It allows faculty and learners to reexamine the simulated case experience, share their mental model, and foster the reasoning behind their clinical judgment. Kolb’s experiential learning cycle involves a concrete experience—simulation, followed by observation and reflection on that experience through debriefing.[4][5] Experiential learning theory suggests that this leads to forming abstract concepts and generalizations, which are then used to test the hypothesis in future situations, resulting in new concrete experiences. The reflective process of debriefing is a cornerstone of the experiential learning theory.[1][4]
Training facilitators in debriefing techniques is critical to ensure effective debriefing among simulation faculty.[6] Historically, formal debriefing training has been provided through various faculty development programs, including simulation instructor training courses, conference-associated workshops, textbook readings, and online modules. Recently, several advanced simulation post-graduate degrees and fellowship programs have been developed.[6] Many simulation educators “learn by doing” and use adjunctive tools and debriefing methods to help guide them throughout the process. Peer teaching can help provide debriefing of the debriefer if multiple facilitators are available for simulation. A growing body of literature describes the characteristics of effective debriefing models and the utility of different debriefing techniques in medical simulation (See Image. Debriefing Techniques Used in Medical Simulation).[7][8][9]
With the vast amount of published literature regarding debriefing, it may be challenging for simulation educators to understand various techniques. This article briefly summarizes the most common debriefing methods and techniques. Additionally, it highlights the prevailing rules and essentials of effective debriefing.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Common Rules and Essentials of Effective Debriefing
In healthcare, multiple techniques and debriefing models have been proposed and utilized, but a gold standard debriefing technique remains unidentified.[10] Despite the diversity of debriefing techniques and frameworks, the majority involve similar “essential” elements described by Cheng (Table 1). These essential elements ensure the safety and efficacy of the debriefing environment regardless of the debriefing setting, the reason for debriefing, or the technique used.[3]
Table 1: Essential Elements of Debriefing and its Characteristics
1. Ensuring psychosocial safety
- ‘‘Behave or perform without fear of negative consequences to self-image, social standing, or career trajectory.”
- Essential to optimize learning outcomes by providing a supportive climate
- This should be conducted during the pre-simulation briefing and then during the debriefing
2. Having a debriefing stance or ‘‘basic assumption,’’
- Predefined basic assumption statement, “We believe that everyone participating in this simulation is intelligent, capable, cares about doing their best, and wants to improve.’’
3. Establishing debriefing rules
- A basic set of rules for debriefing among participants
- Confidential discussion
- Encourage all learners to participate actively
4. Establishing a shared mental model
- Review the event details with input from the facilitator
5. Addressing Key Learning Objectives
- Incorporate and analyze clear learning objectives during debriefing
6. Using open-ended questions
- Helps facilitate discussion and foster reflection
- Avoid close-ended or (yes/no) questions
7. Using silence
- A brief period of silence after a facilitator asks a question
- Promote an internal process within the debriefing learner’s mind
- Allows learners to formulate their thoughts and analyze their mental frames
Issues of Concern
Debriefing Techniques in the Simulation Literature
The science and the art of SBE debriefing have rapidly evolved with the exponential growth of SBE over the last 2 decades. There are descriptions of several diverse models.[10] Although the core of the debriefing process centers on the reflection part of the simulated exercise, there are usually phases that allow this to happen in a structured manner. Many debriefing techniques run naturally through 3 main phases: reaction/description, analysis/understanding, and application/summary, as listed in Table 2.
Table 2: Common Phases of the Debriefing Process
PHASES
1. Reaction/Description
- Time for learners to diffuse and decompress, "blow off steam"
- Open-ended questions about how learners feel?
- Review the facts of the event
2. Understanding/Analysis
- Preview topics/learning objectives
- Explore, discuss, inquire
- What happened? Why did it happen?
3. Application/Summary
- "Take-home messages."
- Apply learning experience to a future encounter
- Allow for learners' questions
However, sometimes debriefings move out of their traditional format based on many factors, including the complexity of the scenario, learners' experience, the amount of time allotted for the simulation exercise, the number of facilitators, or the debriefing skills of the facilitator. To date, no evidence supports 1 debriefing technique over another, leaving space for educators in simulation programs in healthcare to adopt their debriefing techniques based on the factors above.
A facilitator-guided post-event debriefing involves a "debriefer(s)" facilitating a discussion after a simulation event. The role of the facilitator could also be to act as a guide before the simulation (pre-briefing) and during the simulation. The facilitator directs and/or redirects the discussion when needed and ensures that learning objectives get discussed and that the debriefing process is flowing smoothly. The facilitators should position themselves as co-learners, not as a traditional "teacher."[1][10] The level of facilitation and the degree to which the facilitator is involved in the debriefing process depends on many factors like the complexity of the scenario, allotted time and levels, and learners (novice vs. experienced) or learners' personality traits (difficult vs. quite vs. defensive vs. others). This article lists described techniques and tools for debriefing and delineates significant differences and similarities between these techniques when conducting debriefing in the simulated setting. The detailed aspects of the role of the facilitator in the debriefing process are beyond the scope of this article
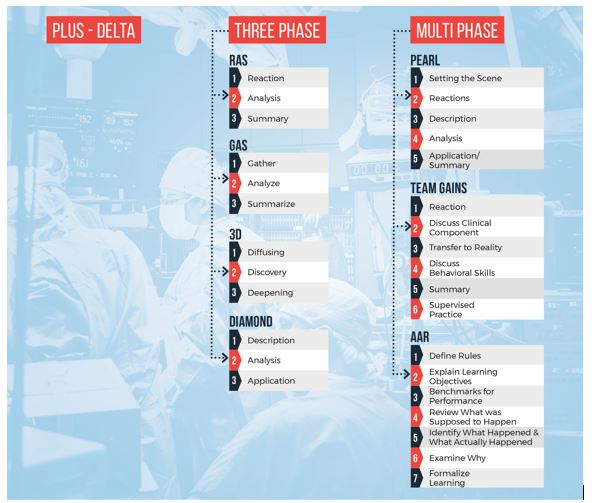
Common Debriefing Techniques
In a recent review article, Cheng et al emphasized that almost all debriefing methods are likely effective if used appropriately by well-trained facilitators. Additionally, a specific debriefing method or technique becomes less important than debriefing the act itself.[10] Given the nature of this article, we did not necessarily attempt to quantify different debriefing techniques or grade the level of evidence; instead, we are providing educators and facilitators with a "toolkit" for debriefing that they can choose from depending on their skill set, and preference, learning environment, and contexts. These debriefing techniques are summarized in Graph 1.
- Plus-delta
One of the most straightforward models among debriefing techniques involves using 2 columns, where the plus column (+) refers to good behaviors or actions. In contrast, the delta refers to behaviors or actions that need improvement or change in the future. This technique allows learners to participate in the discussion and is easily utilizable by novice debriefers.[7][9]
- 3-phase debriefing technique
Many "3-phase" techniques have been developed for use in debriefing. Rudolph et al described a debriefing model called "Debriefing with Good Judgment," where the debriefing session comprises reaction, analysis, and summary (RAS).[11] The reaction phase allows for exploring participants' responses and defusing following the simulation event.
A common question during this phase is "how did that feel?" which allows the facilitator to hear initial reactions, validate emotional responses, and take notes for the next debriefing phase. The analysis focuses on understanding what, why, and how actions evolved during the scenario. It allows both the facilitator and the learners to investigate the gaps noted during the scenario, understand the rationale behind it, and work together toward closing the gap and reflective discussion. A common theme applied during this phase is the advocacy inquiry, where the debriefer tries to unveil the learner's frames. Lastly, the summary phase focuses on lessons learned during the analysis phase and prepares "takeaway" points by learners. Other similar 3-phase techniques have been described by different educators, including the 3D model (defusing, discovery, and deepening), GAS (gather, analyze, and summarize), and the Diamond debriefing, which includes description, analysis, and application.[8][12][13]
- Multiphase debriefing techniques
Several "multiphase" debriefing techniques have been proposed, with additional phases added to allow focus on key themes of debriefing and support the debriefing conversation.
Promoting Excellence and Reflective Learning in Simulation (PEARL)
A blended 4-phase debriefing framework, where 3 phases are based on the same framework as RAS, with an additional descriptive phase to summarize key events encountered during the scenario and ensure a shared mental model between the facilitator and learners.[7] This tool has explicit debriefing steps with possible wording choices facilitators can use, making it an easy-to-implement debriefing tool.
Team-Guided Team Self-Correction, Advocacy-Inquiry, and Systemic-Constructivist
(TeamGAINS)
A 6-phase hybrid debriefing technique for team training in simulated events that integrates 3 major key approaches: guided team self-correction, advocacy-inquiry, and systemic-constructivist techniques.[14]
The healthcare simulation after-action review (AAR)
This multiphase debriefing technique is based on the US Army's After-Action Review (AAR). This tool has been used by the US Army and civilian organizations for decades. This tool includes 7 sequential steps and has been proposed for use in the healthcare setting following simulation events. This structured format addresses learning objectives and performance and can provide even novice debriefers with a concise and effective debriefing framework.[9]
Graph 1: Different debriefing techniques utilized in medical simulation
Other Adjuncts and Tools in the Debriefing Process
Given that the facilitator's skills in conducting debriefing are paramount, various faculty development activities for training in debriefing have been described (workshops, webinars, full-day courses, or longitudinal programs). To date, there is no robust evidence regarding the best structure or format of these activities, making the potential of these methods unfulfilled.[1][15] Various debriefing adjuncts have been identified in the literature to help facilitators conduct the debriefing session and promote the learning environment. Chang et al published 3 major adjuncts that facilitators and educators in the simulated setting can utilize (table 3). Additionally, different debriefing online resources have been published and made available for facilitators to foster debriefing practices and support clinical medical educators.
Table 3: Debriefing Adjuncts
Adjunct
1. Codebriefing
Benefits
- More than 1 facilitator was involved in conducting the debriefing
- Allows for a large pool of expertise and viewpoint
- Facilitators complement each other style
Challenges
- Facilitators may have different agenda
- Facilitators interrupt each other
- One facilitator's domination of the discussion
- Open disagreement
2. Debriefing Script
Benefits
- This may improve the facilitator's ability to lead the debrief effectively
- It may enhance the acquisition of knowledge
3. Video Review
Benefits
- Helps to facilitate by grounding the discussion using the video as evidence
- Highlights areas of excellent and poor performance
Challenges
- No evidence of its benefit in enhancing educational outcomes when compared to debriefing without video
Clinical Significance
Debriefing is a powerful tool and a robust educational technique in medical education. The widespread use of debriefing in simulation programs has correlated with enhanced team performance and improved behavioral and technical skills of providers in simulated settings. Debriefing following clinical events has evolved in the last 2 decades and has improved clinical performance and patient care.[4][16] Promising research studies demonstrated the utility of post-clinical event debriefing in the acute care setting, particularly in the emergency department and the intensive care setting, in the context of rare and stressful events like cardiac arrest.[17][18][19][20] More specifically, post-cardiac arrest resuscitation debriefings have correlated with improved compliance with resuscitation guidelines and patient survival and neurologic outcomes.[20] The American Heart Association (AHA) endorses debriefing as a modality to improve the quality of cardiopulmonary resuscitation.
The 2 common debriefing formats following clinical events are hot (immediately, minutes, or hours after the event) and cold (days to weeks after the event). Hot debriefing usually relies on participants' memories and thought processes to discuss the clinical event. It incorporates the “qualitative” debriefing format to assess and address urgent issues following the event. In contrast, cold debriefing incorporates formal “quantitative” debriefing with a collection of quantitative data and follow-up patient information to enhance quality improvement opportunities and system improvement.[16][17][18]
Conclusion
Debriefing is the cornerstone of effective simulation-based medical education. While the evidence-based gold standard debriefing technique is yet to be determined, most of these techniques are likely effective if utilized appropriately by educators and facilitators.
Enhancing Healthcare Team Outcomes
Simulation debriefing can improve performance across many medical disciplines, including clinicians, nurses, pharmacists, and other allied healthcare providers. All healthcare team members involved in simulation and debriefing must have open communication channels to provide optimal feedback to the learners so they can focus on areas for improvement and replicate their strengths in the future.
Media
(Click Image to Enlarge)
Debriefing Techniques Used in Medical Simulation
Contributed by B Bokhart
References
Fanning RM, Gaba DM. The role of debriefing in simulation-based learning. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2007 Summer:2(2):115-25. doi: 10.1097/SIH.0b013e3180315539. Epub [PubMed PMID: 19088616]
Dieckmann P, Molin Friis S, Lippert A, Ostergaard D. The art and science of debriefing in simulation: Ideal and practice. Medical teacher. 2009 Jul:31(7):e287-94 [PubMed PMID: 19811136]
Gardner R. Introduction to debriefing. Seminars in perinatology. 2013 Jun:37(3):166-74. doi: 10.1053/j.semperi.2013.02.008. Epub [PubMed PMID: 23721773]
Sawyer T, Loren D, Halamek LP. Post-event debriefings during neonatal care: why are we not doing them, and how can we start? Journal of perinatology : official journal of the California Perinatal Association. 2016 Jun:36(6):415-9. doi: 10.1038/jp.2016.42. Epub 2016 Mar 31 [PubMed PMID: 27031321]
Chmil JV, Turk M, Adamson K, Larew C. Effects of an Experiential Learning Simulation Design on Clinical Nursing Judgment Development. Nurse educator. 2015 Sep-Oct:40(5):228-32. doi: 10.1097/NNE.0000000000000159. Epub [PubMed PMID: 25763781]
Cheng A, Grant V, Dieckmann P, Arora S, Robinson T, Eppich W. Faculty Development for Simulation Programs: Five Issues for the Future of Debriefing Training. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2015 Aug:10(4):217-22. doi: 10.1097/SIH.0000000000000090. Epub [PubMed PMID: 26098492]
Bajaj K, Meguerdichian M, Thoma B, Huang S, Eppich W, Cheng A. The PEARLS Healthcare Debriefing Tool. Academic medicine : journal of the Association of American Medical Colleges. 2018 Feb:93(2):336. doi: 10.1097/ACM.0000000000002035. Epub [PubMed PMID: 29381495]
Jaye P, Thomas L, Reedy G. 'The Diamond': a structure for simulation debrief. The clinical teacher. 2015 Jun:12(3):171-5. doi: 10.1111/tct.12300. Epub [PubMed PMID: 26009951]
Sawyer TL,Deering S, Adaptation of the US Army's After-Action Review for simulation debriefing in healthcare. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2013 Dec [PubMed PMID: 24096913]
Sawyer T, Eppich W, Brett-Fleegler M, Grant V, Cheng A. More Than One Way to Debrief: A Critical Review of Healthcare Simulation Debriefing Methods. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2016 Jun:11(3):209-17. doi: 10.1097/SIH.0000000000000148. Epub [PubMed PMID: 27254527]
Rudolph JW, Simon R, Dufresne RL, Raemer DB. There's no such thing as "nonjudgmental" debriefing: a theory and method for debriefing with good judgment. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2006 Spring:1(1):49-55 [PubMed PMID: 19088574]
Zigmont JJ, Kappus LJ, Sudikoff SN. The 3D model of debriefing: defusing, discovering, and deepening. Seminars in perinatology. 2011 Apr:35(2):52-8. doi: 10.1053/j.semperi.2011.01.003. Epub [PubMed PMID: 21440811]
Burke H,Mancuso L, Social cognitive theory, metacognition, and simulation learning in nursing education. The Journal of nursing education. 2012 Oct [PubMed PMID: 22909039]
Järvisalo J, Saris NE. Action of propranolol on mitochondrial functions--effects on energized ion fluxes in the presence of valinomycin. Biochemical pharmacology. 1975 Sep 15:24(18):1701-5 [PubMed PMID: 13]
Level 3 (low-level) evidenceCheng A, Grant V, Huffman J, Burgess G, Szyld D, Robinson T, Eppich W. Coaching the Debriefer: Peer Coaching to Improve Debriefing Quality in Simulation Programs. Simulation in healthcare : journal of the Society for Simulation in Healthcare. 2017 Oct:12(5):319-325. doi: 10.1097/SIH.0000000000000232. Epub [PubMed PMID: 28538446]
Level 2 (mid-level) evidenceKessler DO, Cheng A, Mullan PC. Debriefing in the emergency department after clinical events: a practical guide. Annals of emergency medicine. 2015 Jun:65(6):690-8. doi: 10.1016/j.annemergmed.2014.10.019. Epub 2014 Nov 15 [PubMed PMID: 25455910]
Wolfe H, Zebuhr C, Topjian AA, Nishisaki A, Niles DE, Meaney PA, Boyle L, Giordano RT, Davis D, Priestley M, Apkon M, Berg RA, Nadkarni VM, Sutton RM. Interdisciplinary ICU cardiac arrest debriefing improves survival outcomes*. Critical care medicine. 2014 Jul:42(7):1688-95. doi: 10.1097/CCM.0000000000000327. Epub [PubMed PMID: 24717462]
Mullan PC, Wuestner E, Kerr TD, Christopher DP, Patel B. Implementation of an in situ qualitative debriefing tool for resuscitations. Resuscitation. 2013 Jul:84(7):946-51. doi: 10.1016/j.resuscitation.2012.12.005. Epub 2012 Dec 21 [PubMed PMID: 23266394]
Level 2 (mid-level) evidenceDine CJ, Gersh RE, Leary M, Riegel BJ, Bellini LM, Abella BS. Improving cardiopulmonary resuscitation quality and resuscitation training by combining audiovisual feedback and debriefing. Critical care medicine. 2008 Oct:36(10):2817-22. doi: 10.1097/CCM.0b013e318186fe37. Epub [PubMed PMID: 18766092]
Level 1 (high-level) evidenceEdelson DP, Litzinger B, Arora V, Walsh D, Kim S, Lauderdale DS, Vanden Hoek TL, Becker LB, Abella BS. Improving in-hospital cardiac arrest process and outcomes with performance debriefing. Archives of internal medicine. 2008 May 26:168(10):1063-9. doi: 10.1001/archinte.168.10.1063. Epub [PubMed PMID: 18504334]