
Introduction
Urethral injury is a relatively rare medical condition accounting for less than 1% of all emergency department visits in the United States.[1] Injury patterns vary and encompass urethral crush, bruising, laceration, and transection. Urethral injuries are never life-threatening, but if left untreated can cause significant morbidity.[2] While most injuries are iatrogenic, traumatic etiologies often caused by high energy mechanisms certainly do carry mortality threats.[3] The injury extent and anatomical location are formative in the development of a management plan.
Clinicians classically use several anatomical landmarks in the evaluation, classification, and management of urethral injuries, which is particularly important among male patients. The male urethra subdivides into anterior and posterior divisions delineated by the urogenital diaphragm. The anterior segment consists of the penile and bulbar urethra while the posterior urethra consists of the membranous and prostatic portions.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of urethral injuries can commonly be classified as anterior or posterior injuries. With some exceptions, anterior injuries involve a crushing mechanism, whereas posterior injuries involve sheering forces. Injury to the anterior urethra is more common motor vehicle traumas, straddle injuries, and blunt/penetrating trauma, whereas pelvic fractures and iatrogenic etiologies are more consistent with injury to the posterior urethra.[4]
Iatrogenic injury secondary to improper urethral catheterization and transurethral instrumentation is the most common cause of urethral traumas worldwide.[2][3] Among men, some estimate that improper urinary catheterization accounts for between 6% to 32% of all urethral injuries.[5] Having an enlarged prostate is the most common risk factor as these individuals often have frequent visits to the emergency department for Foley catheter placement.[5] While common, most iatrogenic urethral injuries usually involve minor, superficial mucosal tears that heal on their own and carry a good prognosis.[6]
Another frequent cause of urethral trauma, especially in men, occurs when confused, disoriented or agitated patients pull out their Foley catheters resulting in urethral trauma. Traditionally, such patients have required restraints, sedation or a bedside sitter to prevent such traumas but more appropriate and highly successful methods have been described. Essentially, nurses are asked to make an assessment of all male patients with Foley catheters on their likelihood of inappropriate self extraction. If this is judged to be a potential problem, various steps are taken to minimize this which include:[7]
- Taping the catheter directly to the skin which makes it more difficult for patients to tightly grip the catheter.
- Running the catheter and tubing underneath the thigh which makes it much harder for confused patients to find.
- Liberal use of pads, pajamas, mesh pants and diapers to help protect the catheter.
- Use of decoy catheters taped over their pads or diapers. Such decoy catheters are not attached to anything so confused or disoriented patients can pull them all they want without any harm.
Because these steps are all initiated by nursing, no physician's order is required and therefore there is no delay to immediate utilization. Implementation of these procedures can dramatically reduce the incidence of patient self-induced urethral trauma from inappropriate Foley catheter extraction.[7]
Penile fractures will sometimes include a partial or compete urethral injury. These injuries are best managed by immediate surgical exploration and repair which is described elsewhere.[8][9][10]
In females, urethral trauma most commonly occurs as an obstetrical complication with 10.3 per 1000 vaginal deliveries resulting in some degree of urethral injury.[1] Damage to the anterior urethra is more common in straddle injuries associated with motor vehicle trauma, whereas pelvic fractures are more consistent with injury to the posterior urethra.[3] Other notable causes of urethral injuries include cases of penile fracture during vigorous sexual intercourse causing simultaneous urethral injury, followed by foreign body associated injuries and self-mutiliation among psychiatric patients.[2][3][6][11]
Epidemiology
Some sources suggest that up to 10% of patients involved in significant blunt or penetrating trauma have a urethral injury.[2] Among these, young males, ages 11 to 25, present most commonly.[2] Men are nearly ten times more likely to experience a urethral injury than women.[1] Anatomically, females are at lower risk because of their comparatively shorter and more mobile urethra as well as the mobility of the uterus.[1][2][3][6] Despite this gender advantage, the incidence of urethral injury among females with pelvic fractures is reportedly as high as 6%.[2][3]
Pathophysiology
Urethral injuries range from tissue contusions to complete open urethral transections. In the acute phase, local tissue swelling or urethral disruption can cause acute urinary retention. If not addressed, for instance, in an intubated patient, this retention can lead to hydronephrosis, acute kidney injury, or acute renal failure in extreme cases.[2] For this reason, there is an overwhelming consensus to prioritize bladder decompression. To some extent, all urethral injuries cause scar tissue formation and, if significant enough, can lead to fibrosis, stenosis, and/or stricture formation.[2] These can be relatively benign or can potentially cause clinically significant urinary retention.
History and Physical
The constellation of historical and physical exam findings associated with a urethral injury is rarely occult. Patients typically present with the recent history of trauma, urological surgery, or sudden onset of pain during intercourse.[2] Physical examination findings suggestive of urethral injury include blood at the urethral meatus, pain or inability to void, pelvic instability, palpable bladder secondary to inability to void, scrotal or labial swelling, high-riding prostate, and a "butterfly" pattern of bruising on the perineum.[2][3][11] A high index of suspicion should be maintained if the patient presents with any of these physical exam findings. Furthermore, in the traumatic setting, The American College of Surgeons, as a part of the advanced trauma life support (ATLS) guidelines, emphasizes the triad of blood at the urethral meatus, inability to void and a palpable bladder as a cause for evaluation of urethral injury.[4]
Evaluation
Retrograde urethrography (RUG) is generally accepted as the gold standard modality for evaluation of the urethra. The RUG has good utility among trauma patients and is easily performed at the bedside. The procedure involves injecting 20 to 30 mL of diluted, water-soluble contrast into the urethral meatus and then obtaining an x-ray. A positive RUG study will demonstrate extravasation of contrast outside of the serpentine cylinder of the urethral tract.[2] A retrograde urethrogram is highly sensitive in detecting urethral injuries but falls short in identifying the precise location of the injury and is somewhat operator-dependent.[2][6][11]
Several other imaging modalities can be options to evaluate urethral injuries. Computed tomography (CT) is the test of choice to assess the intra-abdominal urinary system, including the kidneys, ureters, and bladder.[2] In many cases of blunt traumatic injury, a CT scan will be ordered but this does not replace the need for a retrograde urethrogram as CT fails to adequately evaluate the penile urethra.[2]
The use of magnetic resonance imaging is theoretically attractive but often logistically challenging. Some have advocated for its use among children with a urethral injury where advanced imaging is warranted and this is not unreasonable.[3][12]
Using ultrasonography as a preliminary screening tool for urethral injury is another possibility.[13] In the clinically suspicious setting of a pelvic trauma with possible urethral injury, ultrasonography can be useful for the detection of air within the bulbocavernosus. If air is present, then a more invasive radiographic studies, such as a RUG or CT should be ordered.[13][14]
Classification and proper description of urethral injuries are important in the development of treatment plans and inter-provider communication. Several classification systems exist. Perhaps the most common is the Unified Anatomical Mechanical Classification of Urethral Injuries and is as follows:[15]
- Type 1: Posterior urethra is stretched but intact
- Type 2: Pure posterior urethral injury with a tear of the membranous urethra above the urogenital diaphragm (UGD); partial or complete
- Type 3: Combined anterior and posterior urethral injury with the involvement of UGD; partial or complete
- Type 4: Bladder neck injury with extension into the urethra
- Type 4a: Injury of the base of the bladder with periurethral extravasation
- Type 5: Pure anterior urethral injury; partial or complete
Treatment / Management
Once a urethral injury is identified, an emergent consultation with urology should take place, or patients should be transferred to a center with experienced urological specialists. Treatment of urethral injuries is often multifactorial and somewhat controversial.[16] In the setting of severe multi-trauma, urethral injury is considered not immediately life-threatening so evaluation is often postponed but should not be forgotten.[2][6] (B3)
Surgical intervention is categorized as immediate (0 to 10 days), delayed (10 to 14 days), and late (more than three months) repairs.[2] Surgical intervention, when indicated, should either occur: 1) as soon as possible in cases of penetrating trauma or open injury or 2) later in penile fracture injuries.[2] Principles of surgical intervention involve debridement of penetrating or open urethral injuries, epithelial apposition, the establishment of bladder neck competence, and adequate blood supply to the anastomosis.[2]
There are several main therapeutic principles upon which experts generally agree. The first is that if the patient cannot urinate or if they have blunt trauma to the anterior urethra, the urinary bladder should undergo decompression to prevent further extravasation of urine into the pelvic soft tissue and/or abdomen.[2][3][17][18] Next, all penetrating and open urethral injuries require urgent surgical exploration and possible debridement.[6] Finally, antibiotic administration is recommended to prevent subsequent secondary infection.[3][6](B2)
There are several options for the immediate management of acute urethral injuries after pelvic trauma. An endoscopic realignment is an elegant option for early urethral realignment, particularly in experienced centers. Only normal saline irrigation should be used. A flexible cystoscope or ureteroscope is introduced suprapubically through the bladder and into the prostatic urethra. Simultaneously, a standard cystoscope is placed transurethrally and an attempt is made to pass a guidewire between the two. Once a guidewire has been successfully passed, a Foley catheter can be placed over the wire through the penis and the urethra is realigned. This catheter will remain (with monthly exchanges) until urethral healing is complete and patency has been established; on average, between four weeks and three months.[2] Similar realignment can be attempted non-endoscopically. If these attempts are not successful, a suprapubic tube should be placed and a delayed urethroplasty can be performed later; typically at about 3 months post-injury.
Currently, when a urethral disruption is present, the standard recommendation is to surgically place a suprapubic cystotomy tube. Attempts can initially be made at early endoscopic or non-endoscopic urethral realignment and Foley catheter placement but such attempts should not be overly prolonged to avoid contamination and extravasation. If unsuccessful, a suprapubic tube should be placed with an expectation that a delayed urethroplasty will likely be needed.
Differential Diagnosis
- External genital injury
- Bony pelvic fracture, open vs. closed
- Retroperitoneal hematoma
- Renal injury
- Urinary bladder injury
- Ureteral injury
- Penile fracture
- Urethral contusion
- Complete vs. incomplete urethral disruption
Prognosis
Urethral injuries are never life-threatening, but they are often closely associated with other significant blunt and penetrating traumatic injuries with significant comorbidities, which may complicate treatment.[2] Prognosis is generally good, but many well documented long-term sequelae do exist. In cases that involve children, predicting the prognosis of a urethral injury is particularly difficult. The tissues are less developed and, therefore, less vascularized.[3] An evaluation of sexual function and continence among children should be reserved until after puberty.[6]
Multiple studies and reviews have been done in adults to compare the rates of erectile dysfunction, incontinence and stricture formation between the various treatment options. Many of these studies are of relatively poor quality but taken together they suggest that the rates of erectile dysfunction (15%-20%) and incontinence (4%-6%) are about the same regardless of the selected therapy, but there appears to be a significant difference in stricture rates. Early urethral realignment techniques have an overall stricture rate of about 45%-53% which increases to 89%-97% with suprapubic tube placement and delayed urethroplasty.[19][20][21]
Complications
Without question, urethral injury places the patient at risk for future morbidity. Complications can subdivide into early and late. Early complications center around secondary infection, including abscess formation, and in extreme cases, Fournier's gangrene.[2] Late complications include urethral stricture and stenosis, fibrosis, obliteration of the urethral lumen, urethrocutaneous fistula formation, urinary incontinence, and erectile dysfunction.[2][6][18] As the most common cause, iatrogenic injuries often involve partial urethral injuries and carry the best complication profile.[6]
Management of small strictures of the anterior urethra is by dilatation, whereas more extensive strictures (greater than 2 cm) may require urethrotomy or urethroplasty.[2] Due to the thinner urethral wall of the bulbous urethra, posterior urethral injuries are managed conservatively if possible and then by urethroscopy if necessary.[2] Urethroplasty can be done for the more extensive strictures.
Deterrence and Patient Education
Healthcare workers and patients that self-catheterize should receive education about the risks associated with improper catheterization techniques and have appropriate training to avoid urethral injuries. Also, community education on how to prevent motor vehicle injuries, and the proper use of seatbelts can decrease urethral injuries. Finally, inappropriate patient self-extraction of Foley catheters with resultant urethral trauma can be minimized by implementation of a prevention plan as described above.[7]
Enhancing Healthcare Team Outcomes
Appropriate referral/transfer should take place to centers with urological surgeons familiar with urethral reconstruction, particularly in pediatric patients.[3] [Level 5]
Clinicians must maintain a high index of suspicion for urethral injuries, especially in blunt trauma. [Level 5]
While there are many imaging modalities described, RUG has continued to be the test of choice. [Level 3]
It is a known fact that there is a decreased incidence of urethral injury and false passage formation if healthcare practitioners perform dilation of urethral strictures with a guidewire.[6] [Level 5]
An interprofessional team approach is the optimal management course, to include all specialties as cited above. Urology registered nursing staff is an invaluable asset in these cases, providing assistance before, during, and after all procedures, answering patient questions, and administering medications (e.g., antibiotics, analgesics, etc.) as needed. This interprofessional approach with open communication among all staff members and specialties optimizes results while minimizing adverse outcomes. [Level 5]
Media
(Click Image to Enlarge)
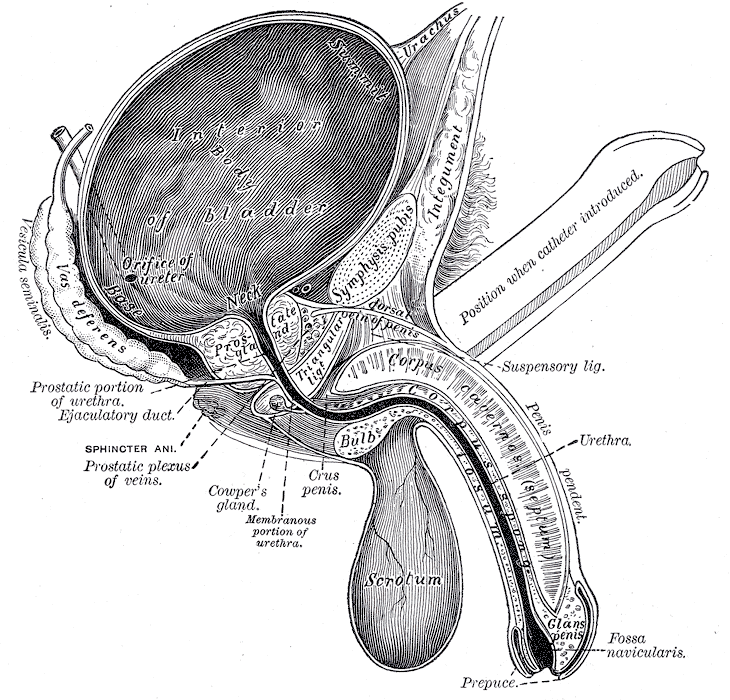
The Penis, Vertical section of bladder, penis, and urethra
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
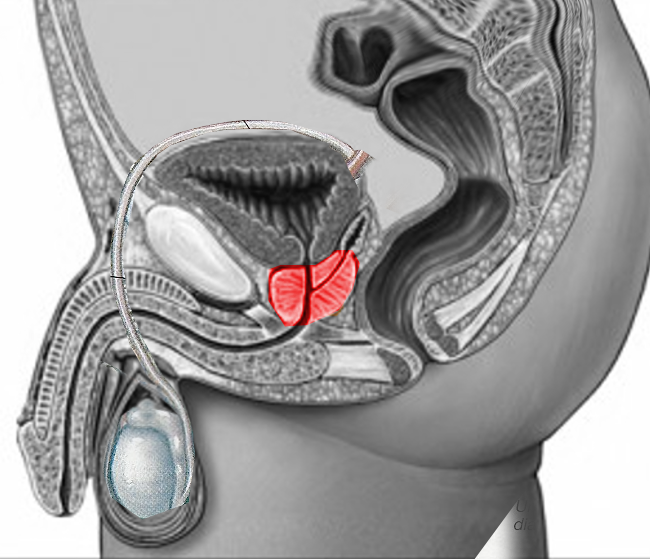
The Prostate gland
Image courtesy S Bhimji MD
(Click Image to Enlarge)
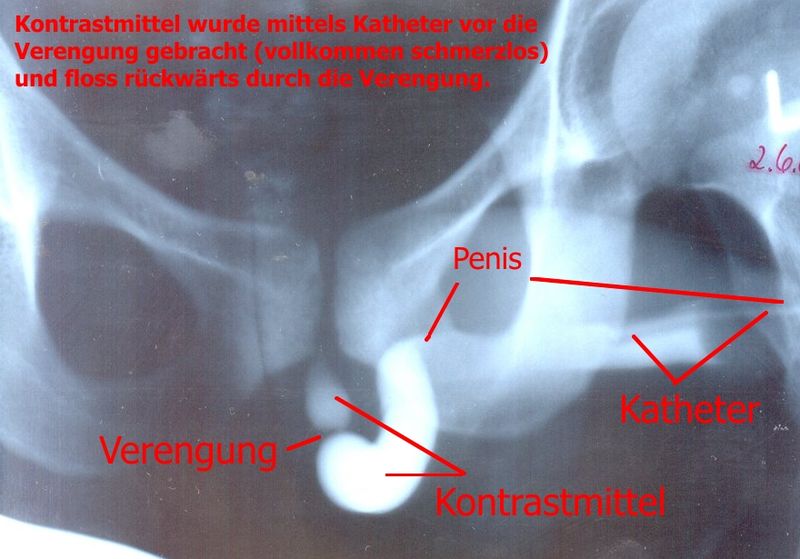
Urethral stricture
Image courtesy: https://commons.wikimedia.org/wiki/File:Urethra_stricture.jpg
(Click Image to Enlarge)
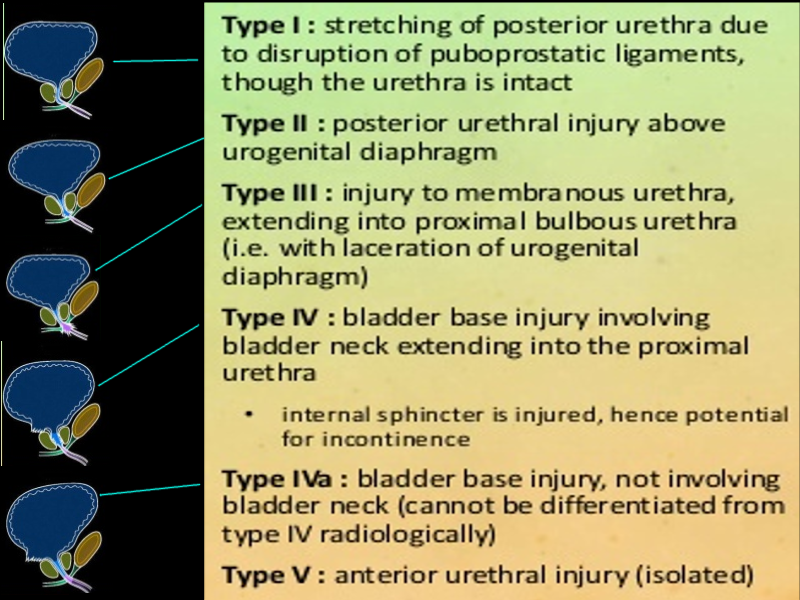
Types of urethral injuries
Image courtesy S Bhimji MD
(Click Image to Enlarge)
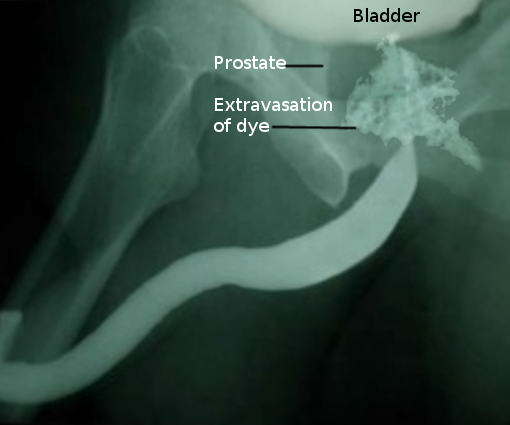
Retrograde urethrogram
Image courtesy S Bhimji MD
References
Patel DN, Fok CS, Webster GD, Anger JT. Female urethral injuries associated with pelvic fracture: a systematic review of the literature. BJU international. 2017 Dec:120(6):766-773. doi: 10.1111/bju.13989. Epub 2017 Sep 7 [PubMed PMID: 28805298]
Level 1 (high-level) evidenceChapple CR. Urethral injury. BJU international. 2000 Aug:86(3):318-26 [PubMed PMID: 10930940]
Pichler R, Fritsch H, Skradski V, Horninger W, Schlenck B, Rehder P, Oswald J. Diagnosis and management of pediatric urethral injuries. Urologia internationalis. 2012:89(2):136-42. doi: 10.1159/000336291. Epub 2012 Mar 19 [PubMed PMID: 22433843]
Kong JP, Bultitude MF, Royce P, Gruen RL, Cato A, Corcoran NM. Lower urinary tract injuries following blunt trauma: a review of contemporary management. Reviews in urology. 2011:13(3):119-30 [PubMed PMID: 22114545]
Manalo M Jr, Lapitan MC, Buckley BS. Medical interns' knowledge and training regarding urethral catheter insertion and insertion-related urethral injury in male patients. BMC medical education. 2011 Sep 27:11():73. doi: 10.1186/1472-6920-11-73. Epub 2011 Sep 27 [PubMed PMID: 21951692]
Mundy AR, Andrich DE. Urethral trauma. Part II: Types of injury and their management. BJU international. 2011 Sep:108(5):630-50. doi: 10.1111/j.1464-410X.2011.10340.x. Epub [PubMed PMID: 21854524]
Leslie SW, Sajjad H, Sharma S. Prevention of Inappropriate Self-Extraction of Foley Catheters. StatPearls. 2023 Jan:(): [PubMed PMID: 29489183]
Diaz KC, Cronovich H. Penis Fracture. StatPearls. 2023 Jan:(): [PubMed PMID: 31869082]
Ge G, Wang H, Chen Y, Li G, Ma L. Complete urethral injury in the penile fracture: a case report and literature review. Translational andrology and urology. 2021 Feb:10(2):969-975. doi: 10.21037/tau-20-1155. Epub [PubMed PMID: 33718097]
Level 3 (low-level) evidenceMathew J, Parmar K, Chandna A, Kumar S. Penile fracture associated with complete urethra and bilateral corpora cavernosa transection. Annals of the Royal College of Surgeons of England. 2021 Mar:103(3):e88-e90. doi: 10.1308/rcsann.2020.7042. Epub [PubMed PMID: 33645282]
Chapple C, Barbagli G, Jordan G, Mundy AR, Rodrigues-Netto N, Pansadoro V, McAninch JW. Consensus statement on urethral trauma. BJU international. 2004 Jun:93(9):1195-202 [PubMed PMID: 15180604]
Level 3 (low-level) evidenceWang Z, Song G, Xiao Y, Liang T, Wang F, Gu Y, Zhang J, Xu Y, Jin S, Fu Q, Song L. The value of magnetic resonance imaging geometric parameters in pre-assessing the surgical approaches of pelvic fracture urethral injury. Translational andrology and urology. 2020 Dec:9(6):2596-2605. doi: 10.21037/tau-20-1064. Epub [PubMed PMID: 33457232]
Dell'Atti L. The role of ultrasonography in the diagnosis and management of penile trauma. Journal of ultrasound. 2016 Sep:19(3):161-6. doi: 10.1007/s40477-016-0195-4. Epub 2016 Jan 22 [PubMed PMID: 27635160]
Wongwaisayawan S, Krishna S, Sheikh A, Kaewlai R, Schieda N. Imaging spectrum of traumatic urinary bladder and urethral injuries. Abdominal radiology (New York). 2021 Feb:46(2):681-691. doi: 10.1007/s00261-020-02679-0. Epub 2020 Jul 28 [PubMed PMID: 32725483]
Goldman SM, Sandler CM, Corriere JN Jr, McGuire EJ. Blunt urethral trauma: a unified, anatomical mechanical classification. The Journal of urology. 1997 Jan:157(1):85-9 [PubMed PMID: 8976222]
Kommu SS, Illahi I, Mumtaz F. Patterns of urethral injury and immediate management. Current opinion in urology. 2007 Nov:17(6):383-9 [PubMed PMID: 17921771]
Level 3 (low-level) evidenceBryk DJ, Zhao LC. Guideline of guidelines: a review of urological trauma guidelines. BJU international. 2016 Feb:117(2):226-34. doi: 10.1111/bju.13040. Epub 2015 Jul 6 [PubMed PMID: 25600513]
Cavalcanti AG, Krambeck R, Araújo A, Rabelo PH, Carvalho JP, Favorito LA. Management of urethral lesions in penile blunt trauma. International journal of urology : official journal of the Japanese Urological Association. 2006 Sep:13(9):1218-20 [PubMed PMID: 16984556]
Level 2 (mid-level) evidenceWarner JN, Santucci RA. The management of the acute setting of pelvic fracture urethral injury (realignment vs. suprapubic cystostomy alone). Arab journal of urology. 2015 Mar:13(1):7-12. doi: 10.1016/j.aju.2014.08.003. Epub 2014 Sep 17 [PubMed PMID: 26019971]
Light A, Gupta T, Dadabhoy M, Daniel A, Nandakumar M, Burrows A, Karthikeyan S. Outcomes Following Primary Realignment Versus Suprapubic Cystostomy with Delayed Urethroplasty for Pelvic Fracture-Associated Posterior Urethral Injury: A Systematic Review with Meta-Analysis. Current urology. 2019 Nov:13(3):113-124. doi: 10.1159/000499282. Epub 2019 Nov 13 [PubMed PMID: 31933589]
Level 1 (high-level) evidenceKoraitim MM. Pelvic fracture urethral injuries: evaluation of various methods of management. The Journal of urology. 1996 Oct:156(4):1288-91 [PubMed PMID: 8808856]