
 Anatomy, Shoulder and Upper Limb, Hand Extensor Pollicis Longus Muscle
Anatomy, Shoulder and Upper Limb, Hand Extensor Pollicis Longus Muscle
Introduction
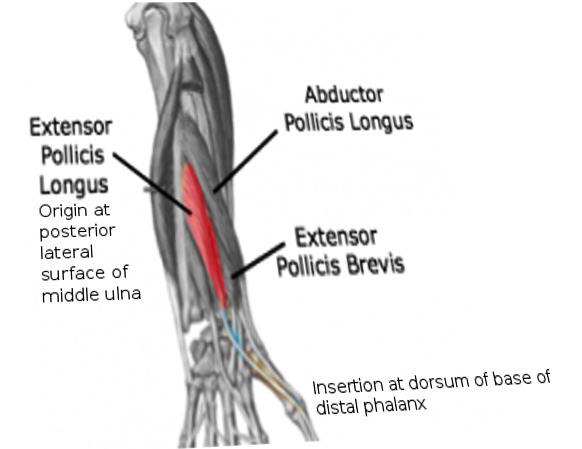
An important contributor to thumb function, the extensor pollicis longus (EPL) muscle is an extrinsic thumb muscle that extends and adducts the thumb metacarpophalangeal (MCP) and interphalangeal (IP) joints (see Image. Extensor Pollicis Longus). Innervated by the posterior interosseous nerve, the EPL receives its blood supply from the anterior interosseous artery, posterior interosseous artery, radial artery, and ulnar artery. Extensor pollicis longus variants are rare, with a prevalence of only 1%. The EPL tendon is associated with pathologies ranging from stenosing tenosynovitis to spontaneous tendon rupture.[1] These pathologies are often seen in association with either medical comorbidities (eg, rheumatoid arthritis) or as sequelae or associated pathology in the setting of trauma (eg, distal radius fractures).[2][3][4][5] Regarding the latter, the EPL may spontaneously rupture in up to 5% of adults following a non-displaced distal radius fracture or in pediatric patients with dorsal plating for a displaced distal radius fracture. Overall, it is important to understand the EPL well to understand the anatomy and potential pathologies, particularly as each relates to the potential compromise of dynamic thumb function.[6][7][8][9]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The extensor pollicis longus muscle is an extrinsic thumb muscle belonging to the deep dorsal forearm muscle group. The extensor pollicis longus originates on the middle third of the posterior ulnar diaphysis, traverses laterally along the forearm, passes over Lister's tubercle, goes through the third osteofibrous tunnel and travels superiorly to the extensor carpi radialis longus, and extensor carpi radialis brevis then inserts on the base of the distal phalanx of the pollex. An osteofibrous tunnel is a passageway found along synovial joints with a bony floor and a fascial roof, with the fascia running in a transverse pattern to help contain neurovascular structures and tendons. These tunnels also have the name of the extensor compartments. The EPL is the only anatomic occupant of the third extensor compartment. There are a total of 6 extensor compartments in the wrist.[2][10][11][12]
As the extensor pollicis longus crosses the wrist, the muscle belly transitions into a tendon (surrounded by a synovial tendon sheath), which forms the medial border of the anatomical snuffbox of the wrist. The tendon splits into 2 different parts, the proximal and distal tendonous divisions, which are separated by a fenestra. The total length of the tendon ranges from 6.7 to 9.7 cm, and the fenestra ranges from 3.1 to 3.5 cm in length. Three tendons form the anatomical snuffbox surface, from medial (ulnar) to lateral (radial):
- EPL tendon
- The extensor pollicis brevis (EPB) tendon
- The abductor pollicis longus (APL) tendon
The floor of the anatomical snuffbox comprises the scaphoid and trapezium bones and the extensor carpi radialis longus and brevis.[13][14][15] The anatomical snuffbox contains the radial artery, radial nerve, and cephalic vein. As the EPL tendon crosses the first MCP joint dorsally, it gets stabilized by the sagittal band (SB). The sagittal band is U-shaped and has radial and ulnar components, with the radial component originating on the palmar aspect of the MCP by the abductor pollicis brevis tendon and the ulnar component originating on the palmar aspect of the MCP by the adductor pollicis tendon.[16] While both components directly attach to the EPL, the radial component of the sagittal band is more crucial for EPL stabilization, and damage to it correlates with EPL instability.[10][17][18]
Extensor pollicis longus extends the terminal phalanx of the thumb. The abductor pollicis brevis and adductor pollicis both attach to the extensor pollicis longus tendon and can extend the thumb's interphalangeal joint to the neutral position. Only the extensor pollicis longus causes full hyperextension at the interphalangeal joint.
Embryology
The precursor extensor muscle mass gives rise to the musculature in the forearm by differentiating into 3 portions. The radial portion gives rise to the extensor carpi radialis longus, extensor carpi radialis brevis, and brachioradialis. The superficial portion gives rise to the extensor digitorum communis, extensor carpi ulnaris, and extensor digiti minimi. The deep portion gives rise to the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis. The radial and superficial portions of the extensor muscle mass appear to be well conserved among different primate species. In contrast, significant differences between the deep portions exist, which can explain why many variations of the muscles and tendons in that portion can be present. However, variations of the EPL are quite rare, having a prevalence of only 1%.[8]
Blood Supply and Lymphatics
The extensor pollicis longus receives vascular supply from many arterial branches, described below, going from proximal to distal:
- Proximal EPL to the musculotendinous junction (before a synovial tendon sheath surrounds it): supplied by the anterior interosseous artery and its muscular branches.
- Distal to the musculotendinous junction, in the proximal tendon where the synovial tendon sheath starts, the posterior ramus of the anterior interosseous artery gives off branches that penetrate the synovial tendon sheath and supply the tendon.
- Two to 3 branches of the posterior ramus of the anterior interosseous artery supply the edges of the tendon, while 1 branch sometimes supplies the middle.
- In the distal tendon, the dorsal carpal arch (made up of the dorsal carpal branches of the ulnar and radial arteries, which anastomose with the anterior and posterior interosseous arteries) gives off 2 arterial branches: 1 that goes to the periphery of the tendon and 1 that can be found by the end of the synovial tendon sheath.
- Once the 2 arterial branches reach the tendon, they form a “T” shape, giving rise to smaller branches descending towards the tendon's palmar surface and ascending branches returning dorsally.
- The arterial branches of the distal and proximal tendon anastomose.
- The distal portion of the EPL tendon that crosses the first metacarpal, where a synovial tendon sheath does not cover it, is supplied directly by the radial artery.
- The distal portion of the EPL tendon that runs along the phalanges receives supply from the first dorsal metacarpal artery’s digital branch, which originates from the radial artery.[6]
Nerves
The extensor pollicis longus gets innervated by a motor branch of the posterior interosseous nerve, which belongs to the deep group of branches from the posterior interosseous nerve. The posterior interosseous nerve originates from the radial nerve. The radial nerve origin is from the posterior cord of the brachial plexus, C5-T1. The radial nerve splits into the posterior interosseous nerve and the superficial radial nerve by the lateral epicondyle. The posterior interosseous nerve supplies the extensor carpi radialis brevis and supinator muscle, then travels through the supinator muscle for an average length of 4.45 cm and then divides into superficial and deep groups of branches. The superficial group of branches innervates the extensor digitorum communis, extensor digiti minimi, and extensor carpi ulnaris. The deep group of branches innervates the abductor pollicis longus, extensor pollicis brevis, EPL, and extensor indices.[3][4][5]
Muscles
Intrinsic thumb muscles: abductor pollicis brevis, opponens pollicis, adductor pollicis, and the flexor pollicis brevis.
- The abductor pollicis brevis abducts the thumb
- The opponens pollicis flexes and abducts the thumb
- The adductor pollicis flexes and adducts the thumb
- The flexor pollicis brevis flexes and adducts the thumb [2][19]
Extrinsic thumb muscles: EPL, extensor pollicis brevis, abductor pollicis longus, and flexor pollicis longus.
- The EPL extends and adducts the thumb
- The extensor pollicis brevis extends and slightly abducts the thumb
- The abductor pollicis longus extends and abducts the thumb
- The flexor pollicis longus flexes the thumb [2][19]
The deep muscle group of the dorsal forearm consists of EPL, extensor pollicis brevis, abductor pollicis longus, extensor indices, and the supinator.
- The EPL extends and adducts the thumb
- The extensor pollicis brevis extends the thumb
- The abductor pollicis longus abducts the thumb
- The extensor indicis extends the index finger
- The supinator performs supination of the forearm [10][20]
Superficial muscle group of dorsal forearm muscles: extensor digitorum communis, extensor digiti minimi, extensor carpi ulnaris, and the anconeus.
Physiologic Variants
Anomalies of the extensor pollicis longus can be organized by utilizing the Turker Classification:
1a:
- The patient has an extra muscle, with its tendon running through the fourth dorsal compartment, and joins the extensor pollicis longus tendon at the first metacarpal mid-shaft but attaches separately from the EPL at the base of the distal phalanx of the first digit.
1b:
- Patients have an extra muscle, with its tendon running along with the extensor pollicis longus in the third dorsal compartment. However, it attaches separately from the EPL at the base of the distal phalanx of the first digit.
1c:
- The patient has an extra muscle, with its tendon going through the fourth dorsal compartment. It then turns obliquely and runs parallel to the extensor pollicis longus, attaching to the distal EPL tendon.
1d:
- Patients have an extra muscle, with its tendon runs within the fourth dorsal compartment, then turns in an oblique manner, crosses over the extensor carpi radialis tendons, then over the EPL, and attaches to the proximal phalanx of the first digit.
1e:
- Patients have an extra muscle named the extensor pollicis and indicis communis, which originates on the ulna between the extensor pollicis longus and extensor indicis. The muscle splits 2 slips, 1 which courses alongside the EPL on the thumb and the extensor indicis on the index finger. The slip that runs along with the EPL on the thumb inserts at the same location on the distal phalanx as the EPL.
1f:
- The patient has 1 extensor pollicis longus muscle belly, giving rise to 2 separate slips of the EPL tendon: the radial slip and the ulnar slip. The radial slip passes between the first and second extensor compartments, and the ulnar slip passes over the extensor retinaculum. The metacarpophalangeal joint combines them back together and then continues towards the distal phalanx.
1g:
- Patients have an extensor pollicis longus muscle belly, which gives rise to 2 separate slips of the EPL tendon, which run within the third extensor compartment.[8]
A study discovered a cadaver with a unilateral, duplicated tendon of the EPL, which had its muscle belly. In that case, the EPL is bifurcated into 2 tendons by the extensor carpi radialis longus tendon, with 1 tendon running along the normal course of the EPL and inserting at the same location as it and the other tendon (along with its small muscle belly) running along the extensor indicis pathway, inserting at the same location. The muscle belly for the duplicated EPL tendon originated from the normal EPL muscle belly and interosseous membrane. While this may appear to be a Turker Type 1e EPL anomaly, since the duplicated tendon had its muscle belly within the third extensor compartment, it does not fit in the 1e classification since that’s only an anomaly of the number of tendons, not the number of muscle bellies.[21]
It has been described in the case of an asymptomatic patient with hypoplasia of the thumb musculature that the extensor pollicis longus may run through the third extensor compartment and then attach to the radial aspect of the proximal phalanx of the first digit. This arrangement may be an adaptive response to compensate for missing abductor pollicis longus and extensor pollicis brevis muscles and preserve thumb extension and abduction.[2]
There has also been a case report about a patient with a fused muscle belly of the abductor pollicis longus and extensor pollicis brevis, separated into their respective tendons. The EPL went under the extensor retinaculum and into the first compartment attached to the patient’s extensor pollicis brevis.[22]
Finally, a case of the EPL running through the second extensor compartment has also been reported, with the third extensor compartment not containing any tendinous structures. However, the exact insertion of the EPL running through the secondary extensor compartment was not identified.[12] Overall, it is important to be aware of the rare yet significant variations of the EPL, as it helps surgeons and clinicians confidently and precisely treat patients with wrist and hand pathologies.
Surgical Considerations
EPL tenosynovitis
Patients with extensor pollicis longus stenosing tenosynovitis, a rare condition, likely require surgical treatment because there have not been any documented successful attempts at treating patients non-operatively. Additionally, as previously advocated in the literature, the importance of surgical treatment for EPL tenosynovitis is inevitably linked to concerns about EPL tendon rupture with chronic attrition. When performing the surgical correction, the EPL tendon must be completely released and transposed into the subcutaneous tissue on the radial aspect of Lister's tubercle. Transposing the EPL tendon prevents the recurrence of tenosynovitis and tendon bowstringing and prevents compromise of its function.[7]
Distal Radius Fractures
Displaced distal radius fractures that require open reduction and internal fixation (ORIF) may receive surgical treatment with dorsal or volar plating procedures. Patients treated with a dorsal plate have an increased risk for iatrogenic injury to the extensor tendons in the wrist and hand through mechanical irritation of the tendons, which may lead to a ruptured extensor pollicis longus tendon. Although technological advancements in low-profile dorsal plating procedures have continued to evolve in mitigating the risk of iatrogenic extensor tendon injury,[23] this complication remains a known risk.[24]
Tendon transfers
Patients requiring surgical reconstruction of a ruptured extensor pollicis longus tendon may get a tendon transfer or a free tendon graft. The extensor indicis is commonly used for tendon transfer, while other usable tendons include the palmaris longus, extensor carpi radialis longus, extensor carpi radialis brevis, and abductor pollicis longus. While the palmaris longus tendon is avascular, a palmaris longus tendon transfer may be performed to preserve index finger extension power, which commonly decreases after a tendon transfer involving the extensor indicis. It is essential to ensure appropriate tension in the reconstructed tendon; if there is too much tension, the thumb is hyperextended and unable to flex correctly. Without enough tension, there are extension deficits. A surgical technique to approximate the appropriate tension is to lay the patient’s hand on the table, with the forearm pronated and the wrist in a neutral position, and measure the distance of the center of the patient’s thumbnail edge to the table. The distance should be 2 cm. Suppose it is more or less the suturing holding it together. In that case, the reconstruction should be removed and re-done to achieve appropriate tension in the reconstructed EPL so that the thumbnail edge remains 2 cm off the table.[25]
The thumb's sagittal band is vital to stabilizing the extensor pollicis longus tendon, especially the radial component of the sagittal band. When lacerations occur near the MCP joint of the thumb, damage to the radial and ulnar components of the sagittal band may occur, as well as damage to the surrounding tendinous structures such as the EPL and the extensor pollicis brevis. Therefore, it is crucial to repair the damaged structures, especially if there is damage to the radial sagittal band since its function stabilizes the EPL tendon. If the radial sagittal band is not repaired surgically, EPL tendon subluxation may occur. In patients who have rheumatoid arthritis, contracture of the ulnar sagittal band may occur, along with weakness of the radial sagittal band. Ultimately, that can lead to a boutonniere deformity in the thumb. When patients have early rheumatoid arthritis, performing a surgical release of the contracting ulnar sagittal band and fortifying the radial sagittal band through augmenting it may treat the boutonniere deformity.[18]
Patients with EPL tendon anomalies typically are asymptomatic, without deficits in thumb extension or wrist/hand pain. EPL tendon anomalies are often found during surgery while correcting another wrist/hand pathology. In those cases, surgical intervention is not indicated because the patient is not having symptoms. However, when patients are having symptoms, surgical correction through procedures such as an extensor retinaculum release and Lister's tubercle removal is indicated to decrease the amount of EPL tendon compression within the extensor compartment.[8]
Clinical Significance
Tenosynovitis, or inflammation of the synovial tendon sheath that surrounds tendons, commonly occurs in the tendons contained in the first extensor compartment of the wrist, the abductor pollicis longus, and extensor pollicis brevis tendons. In patients who do not have rheumatoid arthritis, it is not commonly found in the other extensor compartments. However, there have been reports of patients developing tenosynovitis of the EPL synovial tendon sheath in the third extensor compartment. Patients often present with non-specific wrist pain after performing repetitive motions of their wrist/thumb and may have tenderness along Lister's tubercle and the EPL tendon. Patients can have pain with passive motion of the first digit IP joint. It might take months for the pain to localize to the third extensor compartment, so this diagnosis is a challenging one. In the limited number of case reports on this condition, it has been noted that all of the patients had an EPL musculotendinous junction that ended within the third extensor compartment, which may have made them more prone to tenosynovitis since there is a tighter compartment.[7]
Distal radius fractures comprise one-sixth of all fractures treated in the emergency room. An uncommon yet documented complication of non-displaced distal radius fractures in adults is a rupture of the EPL several weeks following the fracture. Proposed mechanisms of the ruptured EPL include hematoma and callus formation from the fracture, which causes compression of the third extensor compartment, causing ischemia, irritation, and degeneration of the EPL, leading to rupture. When patients are diagnosed with a distal radius fracture and return a few weeks later complaining of an inability to actively initiate extension of the thumb at the MCP and IP joints but have a full passive range of motion, evaluating the integrity of their EPL is important. When patients have limited active extension of the thumb at the MCP and IP joints but have a full passive range of motion with extension, it’s important to include EPL tendon rupture in the differential diagnosis. Patients may feel a popping sensation when the rupture occurs, and they may have tenderness over Lister’s tubercle.[9][26]
In patients who have thumb muscle hypoplasia, which can present with the EPL tendon inserted on the radial aspect of the proximal phalanx of the thumb, it is important to rule out any general medical syndromes that the thumb hypoplasia can be associated with. Examples are Fanconi anemia, which also presents with pancytopenic anemia, Holt-Oram syndrome, which also presents with congenital heart defects; Cornelia de Lange syndrome, which also presents with dwarfism, Okihiro syndrome, which also presents with impaired eye movement and deafness, VACTERL, or thrombocytopenia with the absence of the radius.[2]
Patients who sustain avulsion fractures of the 2 metacarpals at the insertion of the extensor carpi radialis longus tendon may experience a rupture of their EPL tendon by the avulsed fragment if it is not properly fixated. Therefore, internal fixation of fracture fragments is essential in patients with avulsion fractures at the insertion of the extensor carpi radialis longus tendon to prevent complications.[27]
Media
(Click Image to Enlarge)
Extensor Pollicis Longus
Contributed by O Chaigasame, MD
References
Kardashian G, Vara AD, Miller SJ, Miki RA, Jose J. Stenosing synovitis of the extensor pollicis longus tendon. The Journal of hand surgery. 2011 Jun:36(6):1035-8. doi: 10.1016/j.jhsa.2011.02.004. Epub [PubMed PMID: 21636022]
Hong J, Kim DK, Kang SH, Seo KM. Anomalous course of the extensor pollicis longus with multiple absences of thumb muscles. Annals of rehabilitation medicine. 2013 Feb:37(1):151-5. doi: 10.5535/arm.2013.37.1.151. Epub 2013 Feb 28 [PubMed PMID: 23526731]
Horton TC. Isolated paralysis of the extensor pollicis longus muscle: a further variation of posterior interosseous nerve palsy. Journal of hand surgery (Edinburgh, Scotland). 2000 Apr:25(2):225-6 [PubMed PMID: 11062588]
Level 3 (low-level) evidenceZhang L, Dong Z, Zhang CL, Gu YD. Surgical Anatomy of the Radial Nerve at the Elbow and in the Forearm: Anatomical Basis for Intraplexus Nerve Transfer to Reconstruct Thumb and Finger Extension in C7 - T1 Brachial Plexus Palsy. Journal of reconstructive microsurgery. 2016 Nov:32(9):670-674 [PubMed PMID: 27351936]
Gragossian A, Varacallo M. Radial Nerve Injury. StatPearls. 2024 Jan:(): [PubMed PMID: 30725989]
Zbrodowski A, Gajisin S, Grodecki J. Vascularization of the tendons of the extensor pollicis longus, extensor carpi radialis longus and extensor carpi radialis brevis muscles. Journal of anatomy. 1982 Sep:135(Pt 2):235-44 [PubMed PMID: 7174499]
Huang HW, Strauch RJ. Extensor pollicis longus tenosynovitis: a case report and review of the literature. The Journal of hand surgery. 2000 May:25(3):577-9 [PubMed PMID: 10811765]
Level 3 (low-level) evidenceTordjman D, Pierrart J, Bellity J, Delgrande D, Masmejean E. Accessory extensor pollicis longus: A rare tendon anomaly. Hand surgery & rehabilitation. 2018 Feb:37(1):60-63. doi: 10.1016/j.hansur.2017.10.234. Epub 2017 Dec 14 [PubMed PMID: 29248395]
Bogart R, Vidlock K. Ruptured Extensor Pollicis Longus Tendon After a Nondisplaced Distal Radius Fracture in a Young Adult Soccer Player. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine. 2020 Jan:30(1):e23-e24. doi: 10.1097/JSM.0000000000000708. Epub [PubMed PMID: 30550417]
Precerutti M, Garioni E, Ferrozzi G. Dorsal forearm muscles: US anatomy Pictorial Essay. Journal of ultrasound. 2010 Jun:13(2):66-9. doi: 10.1016/j.jus.2010.07.007. Epub 2010 Jul 24 [PubMed PMID: 23396199]
Martinoli C, Bianchi S, Gandolfo N, Valle M, Simonetti S, Derchi LE. US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. Radiographics : a review publication of the Radiological Society of North America, Inc. 2000 Oct:20 Spec No():S199-213; discussion S213-7 [PubMed PMID: 11046171]
Kim YJ, Lee JH, Baek JH. Variant course of extensor pollicis longus tendon in the second wrist extensor compartment. Surgical and radiologic anatomy : SRA. 2016 May:38(4):497-9. doi: 10.1007/s00276-015-1541-5. Epub 2015 Aug 8 [PubMed PMID: 26253859]
Tang A, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Carpal Bones. StatPearls. 2024 Jan:(): [PubMed PMID: 30571003]
Hayat Z, Varacallo M. Scaphoid Wrist Fracture. StatPearls. 2024 Jan:(): [PubMed PMID: 30725592]
Lane R, Tafti D, Varacallo M. Scapholunate Advanced Collapse. StatPearls. 2024 Jan:(): [PubMed PMID: 30725809]
Acosta JR, Graefe SB, Varacallo M. Anatomy, Shoulder and Upper Limb, Hand Adductor Pollicis. StatPearls. 2024 Jan:(): [PubMed PMID: 30252315]
Hallett S, Jozsa F, Ashurst JV. Anatomy, Shoulder and Upper Limb, Hand Anatomical Snuff Box. StatPearls. 2024 Jan:(): [PubMed PMID: 29489241]
Jaibaji M, Rayan GM, Chung KW. Functional anatomy of the thumb sagittal band. The Journal of hand surgery. 2008 Jul-Aug:33(6):879-84. doi: 10.1016/j.jhsa.2008.01.039. Epub [PubMed PMID: 18656759]
Smutz WP, Kongsayreepong A, Hughes RE, Niebur G, Cooney WP, An KN. Mechanical advantage of the thumb muscles. Journal of biomechanics. 1998 Jun:31(6):565-70 [PubMed PMID: 9755041]
Javed O, Maldonado KA, Ashmyan R. Anatomy, Shoulder and Upper Limb, Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 29494017]
Talbot CE, Mollman KA, Perez NM, Zimmerman AM, Drew N, Tsung I, Wade C, Finnegan PS, Fredieu JR. Anomalies of the extensor pollicis longus and extensor indicis muscles in two cadaveric cases. Hand (New York, N.Y.). 2013 Dec:8(4):469-72. doi: 10.1007/s11552-013-9512-y. Epub [PubMed PMID: 24426969]
Level 3 (low-level) evidenceRosa RC, de Oliveira KM, Léo JA, Elias BA, Dos Santos PR, de Santiago HA. Anomalous bilateral contribution of extensor pollicis longus and muscle fusion of the first compartment of the wrist. Revista brasileira de ortopedia. 2016 Mar-Apr:51(2):235-8. doi: 10.1016/j.rboe.2016.02.008. Epub 2016 Feb 26 [PubMed PMID: 27069895]
Yu YR, Makhni MC, Tabrizi S, Rozental TD, Mundanthanam G, Day CS. Complications of low-profile dorsal versus volar locking plates in the distal radius: a comparative study. The Journal of hand surgery. 2011 Jul:36(7):1135-41. doi: 10.1016/j.jhsa.2011.04.004. Epub [PubMed PMID: 21712136]
Level 2 (mid-level) evidenceDevaux N, Henning J, Haefeli M, Honigmann P. The Retinaculum Flap for Dorsal Fixation of Distal Radius Fractures. The Journal of hand surgery. 2018 Apr:43(4):391.e1-391.e7. doi: 10.1016/j.jhsa.2018.01.011. Epub [PubMed PMID: 29618418]
Kamoi F, Kondo M, Hayashi M, Uchiyama S, Kato H. A new technique to determine the tension in extensor pollicis longus reconstruction. The Journal of hand surgery, European volume. 2019 Oct:44(8):790-794. doi: 10.1177/1753193419845281. Epub 2019 May 2 [PubMed PMID: 31046534]
Kitridis D, Bei G, Dogramatzis K, Givissis P. Death of an Extensor Pollicis Longus due to a Funeral. Journal of orthopaedic case reports. 2018 Sep-Oct:8(5):89-91. doi: 10.13107/jocr.2250-0685.1228. Epub [PubMed PMID: 30740386]
Level 3 (low-level) evidenceCassell OC, Vidal P. An unreported cause of rupture of the extensor pollicis longus tendon. Journal of hand surgery (Edinburgh, Scotland). 1996 Oct:21(5):640-1 [PubMed PMID: 9230951]
Level 3 (low-level) evidence