
Introduction
The base of the skull has multiple important foramina that allow the passing of vital tissues, primarily blood vessels and nerves. The two jugular foramina exist at the base of the skull lateral to the foramen magnum. Importantly the internal jugular veins, which drain blood from the brain and intracranial tissues, make their way out of the cranium and terminate at the subclavian veins and ultimately join the brachiocephalic vein.[1] Additionally, cranial nerves IX, X, and XI pass through this foramen, allowing them to send stimuli to multiple extracranial targets.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The jugular foramen is a cavity formed by the petrous part of the temporal bone anteriorly and the occipital bone posteriorly. Its major function is to act as a conduit for essential structures to pass through.
When viewing the skull inferior to superior from an extracranial aspect, the foramina exists lateral to the occipital condyles. Additionally, it sits directly posterior to the carotid canal. Lateral and superior to the jugular foramen sits the external acoustic meatus, which resides within the temporal bone.
Intracranially, the jugular foramen lies at the proximal end of the sigmoid groove. As the occipital bone accommodates the sigmoid sinus within this groove, the sigmoid sinus is led directly into the jugular foramen forming the jugular vein. The internal auditory meatus sits superiorly and slightly medial from the jugular foramen within the petrosal portion of the temporal bone. Closely medial to the jugular foramen sits the hypoglossal canal, which itself is directly lateral to the foramen magnum bilaterally. Superior to the groove of the sigmoid sinus sits the superior margin of the petrous, in which the superior petrous sinus lies. Posterior to the jugular foramen and the sigmoid sinus is the posterior cranial fossa, which accommodates the occipital lobe of the brain.
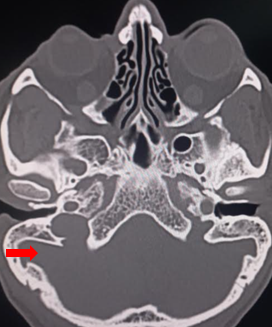
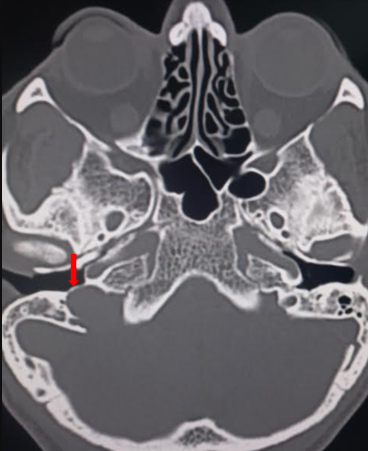
The foramen is divided by a fibro-osseous bridge that connects the jugular spine on the petrous part of the temporal bone and the jugular process of the occipital bone into two parts. The anteromedial compartment, the pars nervosa, contains the glossopharyngeal (IX) nerve, Jacobsen nerve, and the inferior petrosal sinus. The pars vascularis contains the jugular bulb, the vagus nerve (X), Arnold nerve, and the spinal accessory (XI) nerve. The pars vascularis is typically larger on the right causing asymmetry of the jugular foramina.[2][3]
Embryology
The petrous part of the temporal bone and the occipital bone derives from paraxial mesoderm. Both develop via endochondral ossification. As aging and development occur, the bones ossify and form rigid fibrous joints called sutures. Importantly, the joining of these two bones helps create various foramina for vital structures, including the jugular foramen. In rare cases, a persistent primitive artery can cause an abnormal anastomosis between the internal carotid artery and basilar artery.[4] This vestigial artifact can cause symptomatic carotid artery stenosis, as well as provide an avenue for embolic infarction of the brainstem originating from the carotid arteries.[5]
Blood Supply and Lymphatics
The location of the jugular foramina is at the base of the skull between the occipital bone and the temporal bone. The major venous sinuses that drain blood from the brain meet at an area posterior and medial to the occipital bone called the confluence of sinuses. The transverse sinuses, extend laterally from the confluence of sinuses and become the sigmoid sinuses as they begin to descend toward the jugular foramina. The occipital bone contains bony grooves on each side to accommodate the transverse and sigmoid sinuses. Superior and inferior petrosal veins join the sigmoid sinus as it nears the jugular foramen. As the inferior petrosal vein joins the sigmoid sinus, this now singular structure passes through the jugular foramen and becomes the internal jugular vein. In some cases, the inferior petrosal vein joins the internal jugular vein below the jugular foramen.[6]
In some variants, the posterior meningeal artery can enter the cranium via the jugular foramen. This artery supplies mainly the dura in the posterior portion of the cranium.[7]
Nerves
Cranial nerves IX, X, and XI, originate from the brainstem and exit the cranium via the jugular foramen. These nerves originate from the medulla, the inferior most portion of the brainstem.
Cranial nerve IX courses laterally and anteriorly away from the superior medulla and exits the jugular foramen. Immediately after it exits, it creates a superior jugular ganglion, and further branches to innervate its target tissues. Cranial nerve IX also briefly enters the carotid sheath at its superior portion, right as it exits the jugular foramen.[8] This nerve's primary target tissue is the parotid gland, where it supplies parasympathetic innervation.
Cranial nerve X courses laterally and anteriorly away from the middle segment of the medulla and exits the jugular foramen. It then extends inferiorly and branches at many levels as it has many connections throughout the body. Importantly, the major descending branch will enter the carotid sheath and run alongside the carotid artery and internal jugular vein.[8] Cranial nerve X has many target tissues, some of which include vocal cords, heart, and gastrointestinal tract up to two-thirds of the way through the transverse colon. Importantly, within the gastrointestinal tract, it contributes to Auerbach's plexus, which is largely a controller of gut motility. It is the major parasympathetic controller throughout the body.
Cranial nerve XI courses laterally and anteriorly away from the inferior most segment of the medulla and exits the jugular foramen. Immediately as it exits the jugular foramen alongside the vagus nerve, it enters the carotid sheath briefly in its superior portion.[8] Cranial nerve XI passes around the jugular vein via its anterior wall in most cases.
Muscles
Various muscles are innervated by cranial nerves that exit the cranium via the jugular foramen.
Cranial nerve IX innervates the stylopharyngeus muscle, which plays a role in elevating the larynx, and pharynx, and helps to dilate the pharynx to assist with swallowing.
Cranial nerve X plays a significant role in controlling the heart rate via parasympathetic innervation. Additionally, the nerve has inputs in the intestinal musculature to assist with peristalsis and digestion.
Cranial nerve XI, appropriately named spinal accessory nerve, innervates the trapezius and the sternocleidomastoid muscles. The trapezius has many actions, including shoulder shrugging, neck movement, and overall stabilization of the scapula. The sternocleidomastoid primarily acts to rotate the head to the opposite side and flexion of the neck.
Surgical Considerations
Compression or injury at the jugular foramen can lead to jugular foramen syndrome.[9]
Clinical Significance
Traumatic injury to the base of the skull may result in a compromise of structures passing through the jugular foramina, which can result in hemorrhage or air embolism due to damage to the jugular vein.[1] Additionally, it could damage the three cranial nerves IX, X, or XI, causing associated issues. Cranial nerve IX damage may result in impaired taste in the posterior one-third of the tongue, as well as cause dysphagia. Cranial nerve X damage can result in a myriad of dysfunctions, including dysphagia, speaking, gastrointestinal issues, and cardiac issues. Cranial nerve XI damage primarily results in muscular pain in the shoulder, and neck, as well as weakness, affecting the sternocleidomastoid and trapezius.[10]
Media
(Click Image to Enlarge)
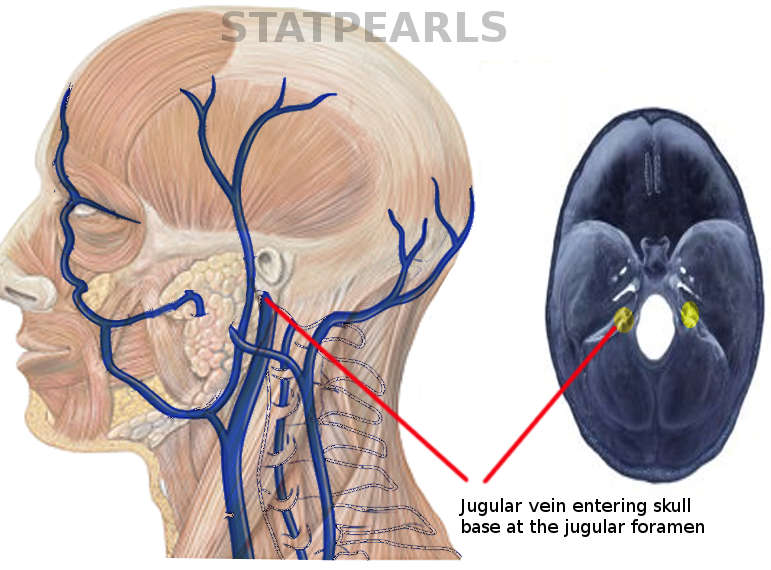
Course of jugular vein
Image courtesy S Bhimji MD
(Click Image to Enlarge)
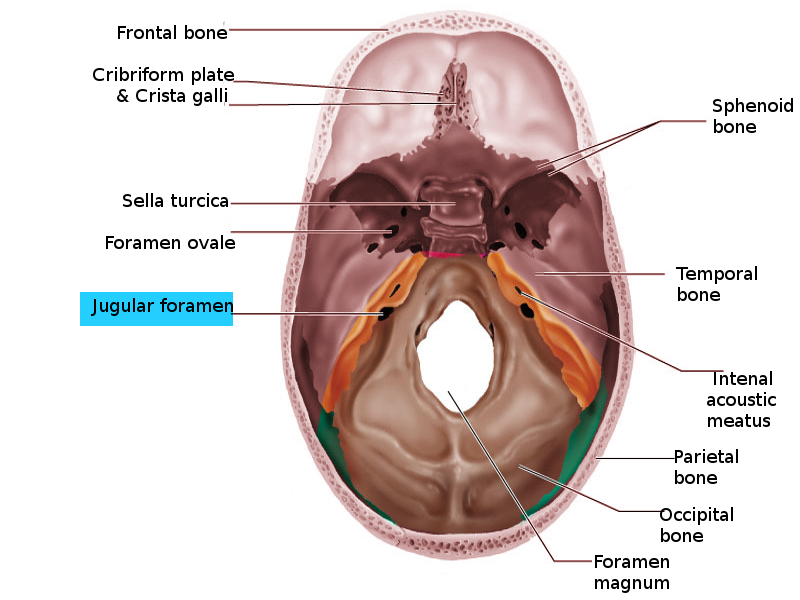
Jugular foramen
Image courtesy S Bhimji MD
(Click Image to Enlarge)

Pars nervosa
Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
Pars vascularis
Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
Jugular spine
Contributed by Sunil Munakomi, MD
References
Rivard AB, Kortz MW, Burns B. Anatomy, Head and Neck: Internal Jugular Vein. StatPearls. 2023 Jan:(): [PubMed PMID: 30020630]
Daniels DL, Williams AL, Haughton VM. Jugular foramen: anatomic and computed tomographic study. AJR. American journal of roentgenology. 1984 Jan:142(1):153-8 [PubMed PMID: 6606950]
Vogl TJ, Bisdas S. Differential diagnosis of jugular foramen lesions. Skull base : official journal of North American Skull Base Society ... [et al.]. 2009 Jan:19(1):3-16. doi: 10.1055/s-0028-1103121. Epub [PubMed PMID: 19568338]
Ryu B, Anami H, Ishikawa T, Inoue T, Sugiura M, Kawamata T. Extremely rare persistent primitive artery passing through the jugular foramen with symptomatic ipsilateral carotid artery stenosis. Acta neurochirurgica. 2016 Oct:158(10):1925-9. doi: 10.1007/s00701-016-2896-z. Epub 2016 Jul 29 [PubMed PMID: 27473392]
Ryu B, Ishikawa T, Hashimoto K, Shimizu M, Yagi S, Shimizu T, Kawamata T. Internal carotid artery stenosis with persistent primitive hypoglossal artery treated with carotid artery stenting: A case report and literature review. The neuroradiology journal. 2016 Apr:29(2):115-21. doi: 10.1177/1971400915626427. Epub 2016 Jan 29 [PubMed PMID: 26825135]
Level 3 (low-level) evidenceFreitas CAF, Santos LRMD, Santos AN, Amaral Neto ABD, Brandão LG. Anatomical study of jugular foramen in the neck. Brazilian journal of otorhinolaryngology. 2020 Jan-Feb:86(1):44-48. doi: 10.1016/j.bjorl.2018.09.004. Epub 2018 Oct 9 [PubMed PMID: 30348503]
Wang G, Yu J, Hou K, Guo Y, Yu J. Clinical importance of the posterior meningeal artery: a review of the literature. The neuroradiology journal. 2019 Jun:32(3):158-165. doi: 10.1177/1971400919840843. Epub 2019 Mar 29 [PubMed PMID: 30924401]
Garner DH, Kortz MW, Baker S. Anatomy, Head and Neck: Carotid Sheath. StatPearls. 2023 Jan:(): [PubMed PMID: 30137861]
M Das J, Al Khalili Y. Jugular Foramen Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 31751061]
AlShareef S, Newton BW. Accessory Nerve Injury. StatPearls. 2023 Jan:(): [PubMed PMID: 30335278]