
Indications
Etanercept was the first anti-tumor necrosis factor (TNF) agent approved by the FDA to treat rheumatoid arthritis. As of this writing, there are five different anti-TNF agents and ongoing expansion in their indications and use in various diseases.[1][2][3][4] While anti-TNF agents have FDA approval for the treatment of several conditions (listed in media item 1), they are also used as off-label agents in various diseases, including graft-vs-host disease, pustular psoriasis, pyoderma gangrenosum, sarcoidosis, and Behcet disease.
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Tumor necrosis factor (TNF) plays a central role in the pathogenesis of several inflammatory conditions, including rheumatoid arthritis (RA). TNF is made intracellularly, mainly by activated macrophages. The precursor TNF is converted to soluble TNF after proteolysis by the TNF-converting enzyme. This soluble TNF then oligomerizes and forms the biologically active homotrimer TNF. There are two types of TNF, which are very closely related, TNF-alpha and TNF-beta. The activities of both TNFs are mediated through binding to the TNF receptors I and II (TNFRI and TNFRII), which are present on almost all cell types (except erythrocytes).[5][6][7]
The binding of TNF to TNFRI and TNFRII activates several signaling pathways, including transcription factor activation (nuclear factor-κB), proteases (caspases), and protein kinases (c-Jun N-terminal kinase, MAP kinase). This signaling leads to activation of the target cell leading to the inflammatory and immune response by releasing several cytokines and apoptotic pathway initiation. Thus, the biological effects of TNF include activation of other cells (macrophages, T-cells, B-cells), proinflammatory cytokine production (IL-1, IL-6), chemokine production (IL-8, RANTES), expression of adhesion molecule (ICAM-1, E-selectin), inhibition of regulatory T-cells, RANK-ligand expression upregulation, matrix metalloproteinase production and induction of apoptosis. The differences in structure and mechanism of action of various anti-TNF agents appear in the second table accompanying this article.
Administration
Etanercept administration is subcutaneous. The injection sites should be rotated and given at least one inch apart from previous injection sites.
Infliximab administration is via an infusion. The infusion should occur over at least 2 hours and should not be co-administered with other biological immunosuppressive agents. Infusion-related reactions are possible, and if necessary, antihistamines, acetaminophen, and corticosteroids can be used as pre-medications to prevent these reactions.
Adalimumab administration is by subcutaneous injection. The injection sites should be rotated and away from previous injection sites.
Certolizumab pegol is subcutaneously administered into the thigh or abdomen.
Golimumab can be administered intravenously (IV) or subcutaneously. Infusions should occur over 30 minutes and should not be co-administered with other biological immunosuppressive agents. Subcutaneous injections use an autoinjector.
Adverse Effects
Anti-TNF agents are generally well tolerated, with the common adverse effects being minor and not needing drug discontinuation. However, serious adverse effects have occurred, the most common being that of severe infections.
Common adverse effects of all anti-TNF agents (occurring in more than 10% of patients)[8][9][4][10][11] include headaches, injection site reaction with the subcutaneous route, and infusion reaction with the intravenous route of administration, rashes, anemia, transaminitis (usually mild), Upper respiratory tract infections, sinusitis, cough, pharyngitis, diarrhea, nausea, and abdominal pain.
Infections
Serious infections are a significant and concerning adverse effect of anti-TNF agents and may include bacterial, fungal, viral, or atypical infections. These infections may be fatal. Infections are more common in patients receiving multiple immunosuppressive agents such as methotrexate or corticosteroids combined with anti-TNF agents. Reports exist of the reactivation of tuberculosis and viral hepatitis B and C, and it is a recommendation to screen individuals for these before initiating an anti-TNF agent. In cases of reactivated latent tuberculosis, the reactivation occurs within the first few months of treatment with TNF-alpha inhibitors. Patients with latent tuberculosis should receive treatment with isoniazid or combination anti-tuberculosis agents before initiating anti-TNF agents. Patients living in areas with a higher incidence of certain fungal infections such as blastomycosis, coccidioidomycosis, or histoplasmosis should have screening for these conditions before initiating anti-TNF agents. Lastly, clinicians should hold anti-TNF therapy in patients who develop a serious infection, and they can consider resuming treatment after complete recovery from the infection, provided the benefits of restarting the anti-TNF therapy outweighs the risk of recurrent infections in the particular patient.
Malignancies
The risk of malignancies, especially lymphomas, has been an area of concern and debate since the introduction of anti-TNF agents. Theoretically, anti-TNF agents can decrease the host defense mechanisms against malignancy by inhibiting TNF. FDA has placed a black box warning on all anti-TNF agents regarding possible association with malignancies, especially lymphomas. The analysis by the FDA in 2003 showed an occurrence of lymphomas in 6 out of more than 6,000 RA patients treated with anti-TNF agents while none in the placebo-treated patients. However, the risk of lymphomas is higher in RA patients (2 to 3 times, especially non-Hodgkins lymphoma), especially with advancing age, and in those with higher RA disease activity. Several subsequent studies have not shown an increased lymphoma risk in RA patients treated with anti-TNF agents compared to those treated with conventional DMARDs.[12][13][14][15] Further studies may help clarify the lymphoma risk and the possible association with anti-TNF agents; caution is recommended in using anti-TNF agents in patients with prior malignancies and those with higher malignancy risk for other reasons.
Several studies have shown a higher risk of non-melanoma skin cancers (up to two times) in patients receiving anti-TNF agents, and annual skin examinations should be considered in patients receiving anti-TNF agents.
Congestive Heart Failure
Initial studies of anti-TNF agents in patients with RA and congestive heart failure NYHA Class III or IV showed poor cardiac outcomes, including increased mortality, an increase in hospitalizations, and a worsening of CHF.[16] However, there are no reports of increased incidence of the development of congestive heart failure in association with anti-TNF agents.[17][18] Clinicians should avoid anti-TNF agents in patients with severe congestive heart failure (NYHA Class III or IV) and use them cautiously in patients with mild congestive heart failure.
Drug-Induced Lupus
Up to 50% of patients receiving an anti-TNF agent can develop positive autoantibodies, including anti-nuclear antibody (ANA) and anti-Ds-DNA antibodies. However, the occurrence of drug-induced lupus is a rare occurrence (less than 1%). The common manifestations of drug-induced lupus from anti-TNF agents are kin rash, thrombocytopenia, leukopenia, hypocomplementemia, and rarely hemolytic anemia.[19] The occurrence of drug-induced lupus from one anti-TNF agent is not always associated with drug-induced lupus from another anti-TNF agent.[20] Symptoms usually resolve within weeks to months of discontinuation of the drug, although autoantibodies may stay positive for several years.
Demyelinating Disorders
There are several reported cases of demyelinating disorders, including optic neuritis, multiple sclerosis (including exacerbation of underlying multiple sclerosis), myelitis, encephalitis, Guillain-Barre syndrome, transverse myelitis, and chronic inflammatory demyelinating polyneuropathy, in patients taking anti-TNF agents.[21] Anti-TNF agents should be avoided or used with extreme caution in patients with an underlying demyelinating disorder.
Skin Reactions
Rashes are not uncommon in patients receiving anti-TNF agents. The most common rash is a local injection site reaction/erythema, although other diffuse cutaneous reactions may also occur. An allergic reaction may lead to a diffuse drug rash. There are also reports of lupus-like rashes, hypersensitivity vasculitis, urticaria, new-onset psoriasis, granuloma annulare, erythema multiforme, and cutaneous T-cell lymphoma.
Pregnancy and Lactation
No controlled trials have taken place to assess the safety of anti-TNF agents in pregnancy or lactation. Anti-TNF agents have been labeled as Class B pregnancy risk by the FDA. Several registries have shown a low risk of major congenital defects with the use of anti-TNF agents in pregnancy, not significantly higher in the disease-matched comparison cohort, and with no birth-defect patterns. Researchers observed no fetal harm or malformations in animal trials. Except for certolizumab, all other anti-TNF agents cross the placenta, exposing the infant to the anti-TNF agent. Anti-TNF agent use in pregnancy should be a consideration only if there is a clear and strong indication.
Similarly, there is no data regarding the use of anti-TNF agents in lactating females. Anti-TNF agents have been found in the human milk at less than 1% of the maternal serum concentration, and there are no reports of adverse effects of anti-TNF agents in breastfed infants or on milk production. It is not known if the infant absorbs the anti-TNF agents at these low concentrations in human milk or not. Until more data is available, clinicians should avoid anti-TNF agents in lactating females.
Contraindications
Patients should not receive anti-TNF agents if there is a history of hypersensitivity reaction to the agent. Clinicians should not initiate and should discontinue ongoing therapy in the presence of an active infection or sepsis. Anti-TNF agents are also contraindicated in patients with NYHA Class III or IV congestive heart failure.
While conventional non-biologic DMARDs such as methotrexate, leflunomide, sulfasalazine, and hydroxychloroquine can be used in combination with anti-TNF agents, concomitant use of an anti-TNF agent with another biological immunosuppressive agent is contraindicated.
Monitoring
Testing for active/latent tuberculosis and viral hepatitis B and C should occur before initiating anti-TNF agents. Clinicians should monitor patients for signs of infection before, during, and after treatment.[10][22] Additionally, complete blood counts and liver function tests are necessary at baseline and monitored closely (at least every 3 to 6 months). Despite the high incidence of autoantibody positivity, it is not necessary to monitor patients on anti-TNF agents for the development of ANA or anti-Ds-DNA antibodies routinely due to the low incidence of symptoms of drug-induced lupus despite the positive autoantibodies. However, patients who develop symptoms of SLE or another autoimmune disease should undergo this testing to help establish a diagnosis.
Patients on anti-TNF agents should not receive any live immunizations, and patients should be up to date with vaccinations before initiating anti-TNF agents.
Anti-TNF agents may be associated with a higher risk in patients undergoing major surgeries such as hip or knee replacement. The recommendation is to hold these medications one week and one dosing cycle before the surgery. They can be resumed two weeks after the surgery, provided there is no infection and incisions are healing well.[23]
Enhancing Healthcare Team Outcomes
As with many medications, there must be interprofessional communication regarding the dispensing and monitoring of the various TNF alpha inhibitors. With inflammatory bowel disease and other autoimmune disorders, physicians and pharmacists must be aware of the treatment guidelines when deciding to treat with TNF alpha inhibitors as opposed to other treatment options.[24] Pharmacists, nurses, and physicians must work together as an interprofessional team to ensure that proper dosing and dispensing protocols are in place and be aware of the possibility of adverse effects.[25]
For example, infliximab requires an infusion over a specified period, cannot be combined with other medications, and there is the possibility of infusion-related reactions. Nursing should be well educated about these facts and coordinate with the pharmacy regarding the dosing and administration. Pharmacy always needs to be involved in dose verification and closely monitor drug interactions, informing the physician if there are any concerns. The healthcare team must work together to ensure patient safety, and the use of electronic medical records may be useful in this setting.[26]
Additionally, the interprofessional healthcare team should be aware of the evolving nature of biosimilars as they relate to prescribing TNF alpha inhibitors and keep up-to-date on the available prescribing options.[27] Here again, the pharmacist is responsible for coordinating with the physicians to appraise them of the latest therapy options. Only through this type of interprofessional collaboration and communication can anti-TNF therapy obtain optimal therapeutic results with minimal adverse events. [Level 5]
Media
(Click Image to Enlarge)
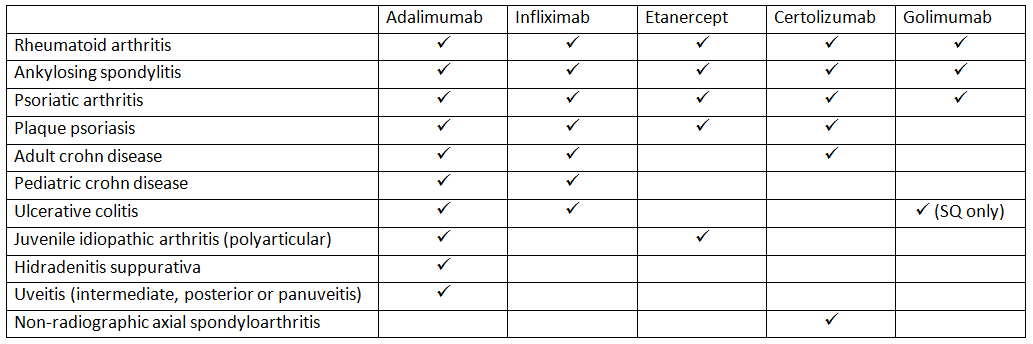
FDA-approved indications of various Anti-TNF agents.
Created and contributed by Pankaj Bansal, MD
(Click Image to Enlarge)
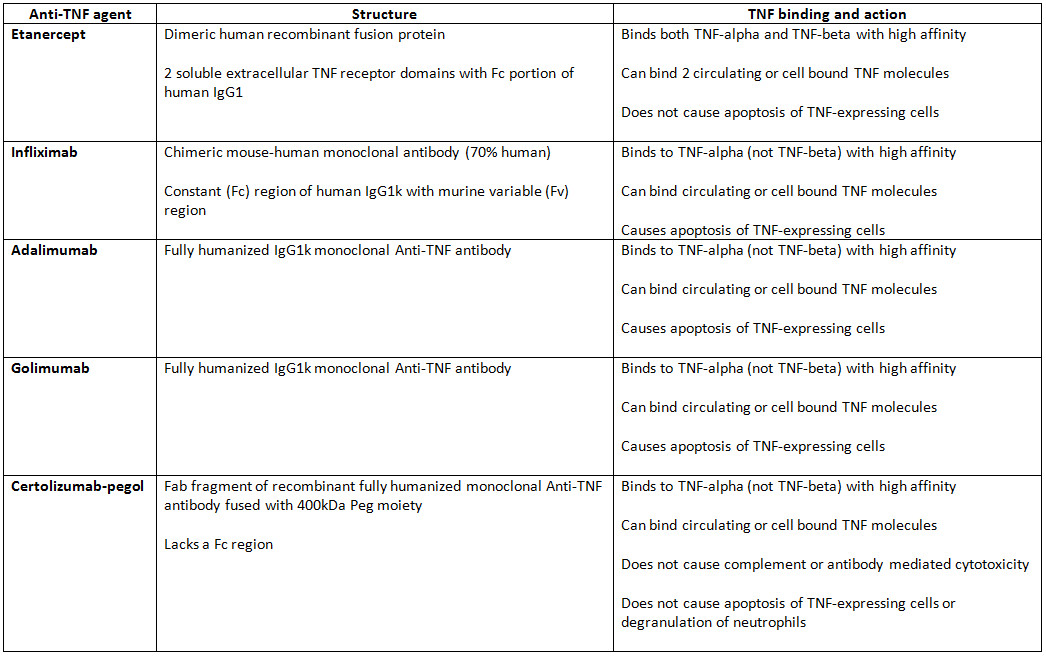
Description of structure and mechanism of action of various Anti-TNF agents.
Created and contributed by Amandeep Goyal, MD and Pankaj Bansal, MD
References
Meroni PL, Valentini G, Ayala F, Cattaneo A, Valesini G. New strategies to address the pharmacodynamics and pharmacokinetics of tumor necrosis factor (TNF) inhibitors: A systematic analysis. Autoimmunity reviews. 2015 Sep:14(9):812-29. doi: 10.1016/j.autrev.2015.05.001. Epub 2015 May 15 [PubMed PMID: 25985765]
Level 1 (high-level) evidenceKomaki Y, Yamada A, Komaki F, Kudaravalli P, Micic D, Ido A, Sakuraba A. Efficacy, safety and pharmacokinetics of biosimilars of anti-tumor necrosis factor-α agents in rheumatic diseases; A systematic review and meta-analysis. Journal of autoimmunity. 2017 May:79():4-16. doi: 10.1016/j.jaut.2017.02.003. Epub 2017 Feb 13 [PubMed PMID: 28209290]
Level 1 (high-level) evidenceRubbert-Roth A, Atzeni F, Masala IF, Caporali R, Montecucco C, Sarzi-Puttini P. TNF inhibitors in rheumatoid arthritis and spondyloarthritis: Are they the same? Autoimmunity reviews. 2018 Jan:17(1):24-28. doi: 10.1016/j.autrev.2017.11.005. Epub 2017 Nov 3 [PubMed PMID: 29108829]
Haraoui B. Differentiating the efficacy of the tumor necrosis factor inhibitors. Seminars in arthritis and rheumatism. 2005 Apr:34(5 Suppl1):7-11 [PubMed PMID: 15852248]
Feldmann M, Maini RN. Anti-TNF alpha therapy of rheumatoid arthritis: what have we learned? Annual review of immunology. 2001:19():163-96 [PubMed PMID: 11244034]
Level 3 (low-level) evidenceGottlieb AB. Tumor necrosis factor blockade: mechanism of action. The journal of investigative dermatology. Symposium proceedings. 2007 May:12(1):1-4 [PubMed PMID: 17502861]
Level 3 (low-level) evidenceRoach DR, Bean AG, Demangel C, France MP, Briscoe H, Britton WJ. TNF regulates chemokine induction essential for cell recruitment, granuloma formation, and clearance of mycobacterial infection. Journal of immunology (Baltimore, Md. : 1950). 2002 May 1:168(9):4620-7 [PubMed PMID: 11971010]
Level 3 (low-level) evidenceMocci G, Marzo M, Papa A, Armuzzi A, Guidi L. Dermatological adverse reactions during anti-TNF treatments: focus on inflammatory bowel disease. Journal of Crohn's & colitis. 2013 Nov:7(10):769-79. doi: 10.1016/j.crohns.2013.01.009. Epub 2013 Mar 1 [PubMed PMID: 23453887]
Cheifetz A, Smedley M, Martin S, Reiter M, Leone G, Mayer L, Plevy S. The incidence and management of infusion reactions to infliximab: a large center experience. The American journal of gastroenterology. 2003 Jun:98(6):1315-24 [PubMed PMID: 12818276]
Level 2 (mid-level) evidenceThalayasingam N, Isaacs JD. Anti-TNF therapy. Best practice & research. Clinical rheumatology. 2011 Aug:25(4):549-67. doi: 10.1016/j.berh.2011.10.004. Epub [PubMed PMID: 22137924]
Moreland LW, Schiff MH, Baumgartner SW, Tindall EA, Fleischmann RM, Bulpitt KJ, Weaver AL, Keystone EC, Furst DE, Mease PJ, Ruderman EM, Horwitz DA, Arkfeld DG, Garrison L, Burge DJ, Blosch CM, Lange ML, McDonnell ND, Weinblatt ME. Etanercept therapy in rheumatoid arthritis. A randomized, controlled trial. Annals of internal medicine. 1999 Mar 16:130(6):478-86 [PubMed PMID: 10075615]
Level 1 (high-level) evidenceWolfe F, Michaud K. The effect of methotrexate and anti-tumor necrosis factor therapy on the risk of lymphoma in rheumatoid arthritis in 19,562 patients during 89,710 person-years of observation. Arthritis and rheumatism. 2007 May:56(5):1433-9 [PubMed PMID: 17469100]
Askling J, Baecklund E, Granath F, Geborek P, Fored M, Backlin C, Bertilsson L, Cöster L, Jacobsson LT, Lindblad S, Lysholm J, Rantapää-Dahlqvist S, Saxne T, van Vollenhoven R, Klareskog L, Feltelius N. Anti-tumour necrosis factor therapy in rheumatoid arthritis and risk of malignant lymphomas: relative risks and time trends in the Swedish Biologics Register. Annals of the rheumatic diseases. 2009 May:68(5):648-53. doi: 10.1136/ard.2007.085852. Epub 2008 May 8 [PubMed PMID: 18467516]
Level 2 (mid-level) evidenceMariette X, Matucci-Cerinic M, Pavelka K, Taylor P, van Vollenhoven R, Heatley R, Walsh C, Lawson R, Reynolds A, Emery P. Malignancies associated with tumour necrosis factor inhibitors in registries and prospective observational studies: a systematic review and meta-analysis. Annals of the rheumatic diseases. 2011 Nov:70(11):1895-904. doi: 10.1136/ard.2010.149419. Epub 2011 Sep 1 [PubMed PMID: 21885875]
Level 2 (mid-level) evidenceWolfe F, Michaud K. Biologic treatment of rheumatoid arthritis and the risk of malignancy: analyses from a large US observational study. Arthritis and rheumatism. 2007 Sep:56(9):2886-95 [PubMed PMID: 17729297]
Level 1 (high-level) evidenceChung ES, Packer M, Lo KH, Fasanmade AA, Willerson JT, Anti-TNF Therapy Against Congestive Heart Failure Investigators. Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure: results of the anti-TNF Therapy Against Congestive Heart Failure (ATTACH) trial. Circulation. 2003 Jul 1:107(25):3133-40 [PubMed PMID: 12796126]
Level 3 (low-level) evidenceWolfe F, Michaud K. Heart failure in rheumatoid arthritis: rates, predictors, and the effect of anti-tumor necrosis factor therapy. The American journal of medicine. 2004 Mar 1:116(5):305-11 [PubMed PMID: 14984815]
Cole J, Busti A, Kazi S. The incidence of new onset congestive heart failure and heart failure exacerbation in Veteran's Affairs patients receiving tumor necrosis factor alpha antagonists. Rheumatology international. 2007 Feb:27(4):369-73 [PubMed PMID: 17028862]
Level 2 (mid-level) evidenceSolhjoo M, Goyal A, Chauhan K. Drug-Induced Lupus Erythematosus. StatPearls. 2023 Jan:(): [PubMed PMID: 28722919]
Williams VL, Cohen PR. TNF alpha antagonist-induced lupus-like syndrome: report and review of the literature with implications for treatment with alternative TNF alpha antagonists. International journal of dermatology. 2011 May:50(5):619-25. doi: 10.1111/j.1365-4632.2011.04871.x. Epub [PubMed PMID: 21506984]
Level 3 (low-level) evidenceShin IS, Baer AN, Kwon HJ, Papadopoulos EJ, Siegel JN. Guillain-Barré and Miller Fisher syndromes occurring with tumor necrosis factor alpha antagonist therapy. Arthritis and rheumatism. 2006 May:54(5):1429-34 [PubMed PMID: 16645971]
Level 3 (low-level) evidenceRosenblum H, Amital H. Anti-TNF therapy: safety aspects of taking the risk. Autoimmunity reviews. 2011 Jul:10(9):563-8. doi: 10.1016/j.autrev.2011.04.010. Epub 2011 May 5 [PubMed PMID: 21570495]
Goodman SM, Springer B, Guyatt G, Abdel MP, Dasa V, George M, Gewurz-Singer O, Giles JT, Johnson B, Lee S, Mandl LA, Mont MA, Sculco P, Sporer S, Stryker L, Turgunbaev M, Brause B, Chen AF, Gililland J, Goodman M, Hurley-Rosenblatt A, Kirou K, Losina E, MacKenzie R, Michaud K, Mikuls T, Russell L, Sah A, Miller AS, Singh JA, Yates A. 2017 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. Arthritis care & research. 2017 Aug:69(8):1111-1124. doi: 10.1002/acr.23274. Epub 2017 Jun 16 [PubMed PMID: 28620917]
Clark M, Colombel JF, Feagan BC, Fedorak RN, Hanauer SB, Kamm MA, Mayer L, Regueiro C, Rutgeerts P, Sandborn WJ, Sands BE, Schreiber S, Targan S, Travis S, Vermeire S. American gastroenterological association consensus development conference on the use of biologics in the treatment of inflammatory bowel disease, June 21-23, 2006. Gastroenterology. 2007 Jul:133(1):312-39 [PubMed PMID: 17631151]
Level 3 (low-level) evidenceCummings JR, Keshav S, Travis SP. Medical management of Crohn's disease. BMJ (Clinical research ed.). 2008 May 10:336(7652):1062-6. doi: 10.1136/bmj.39547.603218.AE. Epub [PubMed PMID: 18467414]
Sharpless BR, Del Rosario F, Molle-Rios Z, Hilmas E. Use of Electronic Health Record Tools to Facilitate and Audit Infliximab Prescribing. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG. 2018 Jan-Feb:23(1):18-25. doi: 10.5863/1551-6776-23.1.18. Epub [PubMed PMID: 29491748]
Chingcuanco F, Segal JB, Kim SC, Alexander GC. Bioequivalence of Biosimilar Tumor Necrosis Factor-α Inhibitors Compared With Their Reference Biologics: A Systematic Review. Annals of internal medicine. 2016 Oct 18:165(8):565-574. doi: 10.7326/M16-0428. Epub 2016 Aug 2 [PubMed PMID: 27479870]
Level 1 (high-level) evidence