
Introduction
A flap is used when more straightforward closure techniques, such as secondary intention, primary closure, or skin grafting, produce a functionally or cosmetically unacceptable result. Flaps can reduce and redirect tension, making them indispensable tools in wound closure. By using nearby tissue, flaps permit excellent skin color, texture, and thickness matching the recipient site. A skin flap uses a reservoir of tissue laxity to close a surgical defect known as the primary defect. The wound created by harvesting the flap is known as the secondary defect. Flaps, unlike grafts, remain attached to a vascular supply known as a pedicle. Local flaps, which use tissue adjacent to the primary defect for closure, are classified by their blood supply pattern. Axial flaps are supplied by a named artery, whereas random pattern flaps are supplied by the dermal plexus or unnamed musculocutaneous arteries.
It is common for flaps to be classified based on their primary motion as well. There are three basic types of tissue movement: transposition, advancement, and rotation. Transposition flaps, such as z-plasties, switch the positions of two or more areas of tissue to transfer skin into a defect. Advancement flaps recruit adjacent tissue to close a defect in a linear direction. Rotation flaps pivot adjacent tissue around an axis to close a primary defect, essentially rotating skin into the defect.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Transfer of local flaps, such as rotational flaps, requires the surgeon to understand the involved anatomy, specifically the vascular anatomy of the skin and the directionality of the relaxed skin tension lines. The skin is perfused by the subdermal plexus, which sends vertically-oriented perforating vessels upwards through the layers of the dermis: the deeper reticular dermis and the more superficial papillary dermis. Superficial to the papillary dermis lies the epidermis, which is composed of the following layers, from deep to superficial: stratum basale, stratum spinosum, stratum granulosum, and stratum corneum. If the subdermal plexus is injured during flap transfer, whether its arterial or its venous component, the tissue is likely to die because it will be too thick to function as a free skin graft; the subdermal plexus is located either within the subdermal fat or deep within the reticular dermis itself.
Within the face, another three concepts are essential to understand to plan flap transfer in a cosmetically acceptable fashion: relaxed skin tension lines (RSTLs) and the lines of maximum extensibility (LMEs), which run perpendicular to them, as well as aesthetic subunits. The RSTLs and LMEs are determined by the direction in which the mimetic muscles contract (perpendicular to RSTLs and parallel to LMEs). Rhytids often form in the RSTLs, and skin stretches most readily along LMEs; therefore, flaps are typically designed so that the incisions lie within RSTLs and/or aesthetic subunit boundaries while avoiding vectors of rotation that will distort cosmetically sensitive structures like lips, eyebrows, and eyelids. The aesthetic subunits of the face are the forehead, periorbital areas, nose, cheeks, perioral area, and chin; several of these, such as the nose and periorbital areas, are further subdivided into smaller subunits, the borders between which may also be used to hide incisions.
Indications
Rotation flaps should be used when other simpler types of closure fail to provide adequate functional or cosmetic results. Rotation flaps, despite their length and arc, can be used in many locations. They are most commonly used for lesions on the lateral face, cheeks, chin, and scalp. Rotation flaps are particularly useful for redirecting tension around a free margin to prevent distortion. Examples of this application include the reconstruction of the eyebrows and lips. There are also several named rotation flaps, such as Tenzel and Mustardé flaps, that are useful in specific situations that will be discussed below.
Contraindications
In addition to the indications for rotation flaps, it is also critical to consider the contraindications for these flaps. Flaps are contraindicated if any existing malignancy is not completely cleared. Failure to achieve clear margins before performing a flap may have disastrous consequences. Residual tumors may grow unrecognized beneath a flap for years. A tumor can spread along the plane of undermining, which can further add to the morbidity of the malignancy.
For this reason, most flaps are performed following Mohs micrographic surgery, as this technique is highly effective for obtaining clear margins. Additionally, patients should be evaluated for any signs of malignancy within or near a flap for the same reasons as above. Surgeons should be aware that future closure options for nearby malignancies may be severely limited by the previous use of a flap and should adjust their closure techniques accordingly.
Proper patient selection is essential in assuring quality outcomes. Limited functional status or access to care may obligate the use of different closure techniques than what might be employed for another patient. The quality of a flap's vascular supply and its durability are also very patient-specific. For example, a pedicle taken from within a scar or an area that underwent radiotherapy may have an impaired vascular supply, and therefore other reconstructive options should be considered.
Relative contraindications to rotational flap transfer include an increased risk of hemorrhage and active smoking. Smokers, in general, have a higher risk of developing complications following surgery. Specifically, they are at increased risk of flap necrosis, which means that other closure options may be preferable.[1] Smokers should be advised to stop or reduce smoking before and after the procedure to help maximize flap survival. Patients on anticoagulant therapy are at increased risk of perioperative and postoperative bleeding, which can also impair flap viability.[2] Current recommendations are to continue prescribed anticoagulant therapy for patients undergoing cutaneous procedures.[3][4] Surgeons should be mindful of these risks in planning wound closure to help decrease the likelihood of adverse outcomes.
Equipment
Equipment required for rotational flap transfer will vary based on surgeon preference but may include the following or similar:
- Local anesthetic agent (1% lidocaine with 1:100,000 epinephrine) in a hypodermic syringe
- Skin cleanser (povidone-iodine, chlorhexidine, isopropyl alcohol)
- Fine-tip surgical marker
- Scalpel (#15 blade or finer for small facial flaps)
- Adson-Brown or 0.5 mm Castroviejo forceps
- Kaye blepharoplasty, iris, or Westcott scissors
- Halsey or Castroviejo needle driver
- Joseph and/or Guthrie two-pronged skin hooks
- Bipolar electrocautery forceps
- Fine-tip monopolar electrocautery pencil
- Suture scissor
- Skin sutures, such as 6-0 polypropylene
- Deep dermal suture, such as 5-0 poliglecaprone
- Topical antibiotic ointment (bacitracin or mupirocin)
- Dressing supplies as necessary
Personnel
Personnel required for the transfer of a rotational flap include a surgeon and an assistant. The latter may be a nurse or a surgical tech; for larger reconstructions, having both available is helpful. Larger, more complicated reconstructions may also require sedation or general anesthesia, which would require the participation of an anesthesia provider as well.
Preparation
Typically, several different reconstructive options may be employed for a given defect, and engaging in a discussion regarding these options with the patient can help to provide realistic expectations. For patients who are amenable, showing them the defect prior to reconstruction can also help inform expectations regarding recovery and scarring.
The defect should be photographed preoperatively for the medical record, including a ruler or measuring tape for scale.
In the operating room, the defect and the surrounding area should be injected with a local anesthetic, including epinephrine, for hemostasis, and additional local anesthetic should be kept readily available on the sterile field for use in the event of insufficient pain control intraoperatively. Cleansing the skin can be performed before or after injection, depending on whether the injections are performed in a sterile fashion or not. A conservative volume of anesthetic should be injected to avoid distorting the area surrounding the defect. Skin preparation may be accomplished with povidone iodine, chlorhexidine, or isopropyl alcohol, according to surgeon preference. The use of non-colored cleansing agents may facilitate intraoperative selection of skin with an appropriate color and texture match, however. Marking the planned flap should be performed in a sterile fashion after skin cleansing, as an application of the cleansing agent is liable to smear or erase the surgical marks if they are made beforehand.
Technique or Treatment
Rotation flaps are elevated using an arcuate or curvilinear incision. Although they are referred to as rotation flaps, in practice, these flaps combine both advancement and rotation to pivot a flap into place (see Figure 1). Due to their arcuate shape, solitary rotation flaps are ideal for closing triangular defects. If a circular defect is being closed with a single rotation flap, the defect must be enlarged into an isosceles triangle along the arc of the tissue movement before flap transfer. The apex of the triangle must point to the center of the arc, and the base of the triangle must be continuous with the arc of the flap.[5] The isosceles triangle should ideally have a length two times the width of the base of the triangle.[5] If the primary defect is not enlarged into a triangle, an additional standing cutaneous deformity will result at the pivot point of the flap. In contrast, closures using multiple rotation flaps do not need to have the primary defect enlarged into a triangle.
Rotational flaps are unique in that they are subject to a tethering effect known as pivotal restraint. Because of this phenomenon, rotation flaps can fall short by not completely covering the most distal edge of the primary defect.[6] The point of pivotal restraint, located at the end of the curvilinear incision farthest from the defect, should be undermined widely to enhance the primary motion of the flap. Wide undermining may be all that is required to close the wound with minimal tension. Undermining is typically performed in the subcutaneous plane, with some exceptions: the nose should be undermined in the submuscular/supraperichondrial plane; the scalp should be undermined in the subgaleal plane; the periorbital area should be undermined above the orbicularis oculi, and the ear should be undermined just superficial to the perichondrium. Caution must be used in undermining, as excessive undermining can separate the pedicle from the perforating arteries supplying it.
Pivotal restraint should be considered in the planning stages of the flap. Pivotal restraint is addressed by making the radius of the arc greater than the length of the defect. Some authors suggest the radius should measure 1-2 times the length of the defect. This increase in radius makes the arc taller than the defect and effectively compensates for the loss of length that occurs as the flap is rotated. Another option is to add more of an advancement component to the flap. Doing so, however, increases the closing tension, which can impair the vascular supply to the tip of the flap.[6] Lastly, adding a back cut to the far end of the incision brings the pivot point closer to the primary defect and typically decreases pivotal restraint. A back cut, however, will decrease the width of the pedicle, which can compromise the vascularity of the flap. The mobility of the tissue is proportional to the length of the back cut, so the surgeon must balance the need for additional movement with the size of the pedicle.[5] A rule of thumb for random pattern facial flaps is to keep the length:width ratio of the pedicle to less than 4:1. The face is a vascularly privileged site and, therefore, can support flaps of this length; however, flaps located elsewhere on the body should have a length:width ratios of less than 2:1.
The angle of the arc should be greater than 90 degrees to distribute tension properly.[7] Extension beyond 90 degrees has minimal effect on decreasing tension but does potentially reduce the size of the standing cutaneous deformity. Ideally, the arc of a rotation flap should be between 90 to 180 degrees. Rotation flaps with arcs less than 90 are subject to higher tension at closure.[5][7] An arc of greater than 180 degrees, on the other hand, changes the vector of tension in a counter-productive manner, usually adding tension in a vector parallel to what would occur with primary wound closure.[8]
The vector of tension for a rotation flap is directed perpendicularly along the arc of the incision, which, in a classic rotation flap, is perpendicular to the tension vector for primary wound closure. Like most flaps, the area of greatest tension is at the closure of the secondary defect. For a pure rotation flap, the maximal tension is directed perpendicular to the arc of rotation, 90 to 135 degrees away from the defect.[7] If there is an advancement component to the flap, the point of maximal tension will be at the tip of the rotation flap. For larger defects, the length and curve of the incision required for flap transfer may run perpendicular to relaxed skin tension lines or cross into other cosmetic units, which can be a limiting factor for the use of rotational flaps. However, the length of the incision may be used advantageously to recruit distant tissue or to hide standing cone deformities in less aesthetically sensitive locations. A good example of a rotational flap used for aesthetic purposes is face lifting, which employs a large rotation-advancement flap to resuspend and smooth the soft tissues of the face.
Due to the primary motion of a rotation flap, a standing cutaneous deformity may be produced at the end of the arc opposite the defect, on the outside of the curve. A common way to address this is to take a Burow’s triangle at some point along the outside of the curve. In some instances, especially with longer incisions, the length difference between the cut skin edges on the inside and outside of the curve can be serially halved using sutures to compress and distribute the excess tissue over the length of the wound. If a back cut is necessary, it can be combined with a Burow’s triangle to create a Z-plasty at the end of the arc.
Double Rotation Flaps
Double Flap
Double rotation flaps are commonly used for defects too large to close with a single rotation flap. Typically, these flaps are used on the scalp or around free margins. These flaps produce a combination of both advancement and rotation, which can make categorization as either rotation or advancement flaps challenging. The design of a double rotation flap starts with a single point on the periphery of the defect, from which arcs proceed in opposite directions to form a semicircle with the defect at the apex of the arc (See figure). Each flap is mobilized and rotated in opposite directions to come together and close the defect. An analogy for this type of movement would be closing a book, where both sides are moving equally to meet in the middle. It is important to note that this defect is enlarged into a triangular defect, with the apex of the triangle pointing away from the apex of the semicircle, unlike the other double rotation flaps discussed below.
O to Z Flap
The O to Z flap is a double rotation flap commonly used on the central scalp or large lesions on the trunk.[8] Defects on the lateral scalp are typically closed with larger solitary rotation flaps. Scalp tissue can be very inelastic, which may necessitate the use of large flaps and long incisions. The scalp is ideal for this flap because the patient’s hair can provide excellent camouflage for these incisions. The flaps start at opposite ends of the defect, with both incisions taking off in the same manner, either clockwise or counterclockwise. Because the incisions are at opposite sides of the defect, the curve of the arcs is in different directions (see figure). Each flap will rotate to cover half of the lesion with minimal enlargement of the primary defect needed. In fact, the tip of each flap will need to be trimmed to inset the flaps properly. Typically, each arc is 180 degrees and rotates tissue in the same direction, meaning both flaps will either rotate in a clockwise or counterclockwise fashion. The final wound assumes an “S” like configuration. A variation of an O to Z flap uses three or more rotation flaps. As in the O to Z flap, all flaps are rotated in the same direction. Due to the configuration of the closure, this flap is called a pinwheel flap. Both the O to Z and the pinwheel flap can incorporate a variable amount of rotation and advancement. For example, the pinwheel flap, when it incorporates mostly advancement, will look like a three-pointed star. The pinwheel flap is also useful for scalp and truncal defects.
Modified Peng Flap
The Peng flap is used for medium to large nasal tip defects.[9] The original Peng flap was primarily an advancement flap, but the Peng flap can be modified to add more of a rotational component.[10] This is essentially a double rotation flap where the pivot point is located along the midline at the nasal root. Rotation flaps are taken from each nasal sidewall and rotated toward the midline to cover the defect. Some pitfalls to this flap include distortion of the symmetry of the nose if the defect is not centrally located. It can also lead to the lifting of the nasal tip or ala. Depending on the degree of cheek advancement, tenting may be noted at the base of the ala, which can be corrected with an incision along the alar groove.[10] This flap may be used as a single-stage alternative for defects that would otherwise require reconstruction with a paramedian forehead flap.
Unique Rotation Flaps
Dorsal Nasal Rotation Flap
Rieger first proposed the dorsal nasal rotation flap in 1967.[11] This flap is used for defects less than 2 to 3 cm in size on the distal nose.[11][12] This flap recruits a reservoir of tissue in the glabella and rotates this tissue along with the nasal dorsum inferiorly to cover the primary defect. The arc of this flap runs along the alar crease superiorly, along the nasal sidewall, and into the glabella. If further rotation is required, a back cut can be made along the contralateral side but should not extend beyond the level of the medial canthus.[8] Marchac et al. described an axial pattern flap using perforators from the angular artery coursing near the medial canthus.[13]
For this reason, back cuts beyond the level of the medial canthus should be avoided because they can compromise the vascular supply of the flap. Making a back cut typically results in a V-Y advancement component to the closure, which also makes categorizing the Rieger flap as a purely rotational technique somewhat incorrect. Patient selection is important in this flap because some patients may not have the tissue laxity necessary to transfer this flap. The Rieger flap can cause a loss of nasal symmetry, lifting of the nasal tip and ala, and distortion of the ala if it is not designed correctly.[12]
Mustardé/Tenzel Flap
The Mustardé flap is used for defects of the lower eyelid and cheek.[8] This flap distributes tension in a horizontal plane and is used to prevent excessive tension on the lower eyelid and subsequent ectropion. The defect is enlarged into a triangular shape, but if it is more than half the surface area of the cosmetic subunit, it may be advisable to remove the remainder of the subunit for aesthetic optimization and use the flap to recreate the entire subunit. The incision is directed laterally from the defect along the lower eyelid. The arc after the lateral canthus is directed superolaterally into the temple region. This exaggerated superior movement is made to counteract the increase in tension induced by pivotal restraint from the primary motion of the flap. The incision then descends along the preauricular skin. This is a large flap, and despite planning for pivotal restraint, it may still induce ectropion due to the weight of the flap. Tacking sutures between the undersurface of the flap and the maxillary periosteum is a frequently used option to offset the weight of the flap.[8] The primary motion of the flap can rotate the beard and sideburns onto the cheek, in some cases, making this closure less preferable in male patients with large defects.
A similar design, known as the Tenzel flap, is a myocutaneous rotation flap used for lower eyelid defects. This is smaller than a Mustardé flap, and it incorporates some of the orbicularis oculi muscle. The incision is carried along the lower eyelid and proceeds superiorly past the lateral canthus, similarly to a Mustardé flap. However, the Tenzel flap does not extend as far as the Mustardé flap. This flap relies on the rotation of the temporal skin and usually requires lysis of the lateral canthal tendon to fully mobilize the tissue being transferred.[8] Since this flap is smaller in size compared to a Mustardé flap, it does not usually need tacking sutures.
Spiral Flap
The spiral flap has several proposed uses, including lower eyelid and ventral fingertip defects.[14][15] However, the original indication for a spiral flap was for deep defects along the alar groove measuring up to 1.5 cm in size. This flap is useful for the ala because it has the potential to preserve the alar groove or sulcus. The flap is incised similarly to a classic rotation flap. However, because of the spiral shape, there are additional variables to consider, including the curvature of the spiral. Defects involving the alar groove should use a spiral where the width of each level of the spiral is the same. This will produce a prominent inward bend that will recreate the groove. Defects along the alar crease will require a shallower depression and should use an algorithmic spiral where each level of the spiral becomes progressively larger. The first arm of the spiral is responsible for the recreation of the alar crease or groove. To properly align this, the first arm of the spiral must have a width equal to the distance from the inferior aspect of the defect to the desired location of the alar groove. This arm will be sutured to the rest of the flap, thus initiating the spiral. The tissue for this flap can be taken from the nasal sidewall or an incision directed along the alar groove.[14][16][17]
The flap will move anteriorly and superiorly or inferiorly, depending on the location of the tissue reservoir. The take-off point of the incision is along the inferior aspect of the defect, with the arc extending anteriorly. As mentioned above, the first arm of the spiral is sutured to the flap to initiate the spiral and recreate the alar crease or groove. The second stitch anchors the flap to the point of maximal tension along the inferior aspect of the defect.
Cervicofacial Flap
The cervicofacial flap is used for very large defects of the cheek. The flap is created similarly to a Mustardé flap, with the incision carried farther onto the neck. The incision runs from the superior aspect of the defect superolaterally to the preauricular cheek. The incision is then extended, crossing under the ear and inferiorly along the lateral neck. The arterial supply comes from perforators of the facial and submental arteries. The cervical skin is an excellent source of redundant tissue and allows for improved tissue matching compared to a skin graft or a flap taken from a distant site. As in the Mustardé flap, cervicofacial flaps can rotate facial hair from the beard and sideburns onto the cheek in male patients with large defects. This is also a very large flap which may necessitate the use of tacking sutures [18]. In essence, a cervicofacial lap is the opposite of a facelift flap in that the tissue is moved medially rather than laterally and superiorly.
Complications
There are a number of complications that can occur following the transfer of a rotational flap. Most complications can be avoided with cautious planning and sound technique. Excessive tension at the time of closure or wound contracture post-operatively can result in distortion of surrounding tissue. Rotation flaps that do not properly distribute tension vectors can distort sensitive structures such as the eyelids or the lips, producing ectropion or eclabium.
Transferring that flap can result in trapdoor deformity or pincushioning if a flap is not sized correctly compared to the defect. A trapdoor deformity makes the healed flap appear as a depressed area compared to the surrounding tissue. This occurs when there is a lack of supporting tissue under the flap or when the flap is thinned too aggressively. Pincushioning, on the other hand, presents with a noticeably raised flap compared to the surrounding tissue. This occurs when there is excess tissue due to too much thickness or if an oversized flap was not adequately trimmed to fit into the defect.
Flap necrosis results from ischemia of the distal end of the flap due to impaired blood flow. Blood flow within a flap can be compromised by making the pedicle too narrow to support the flap or by making the flap too thin and disrupting the blood supply. Flap necrosis can present as epidermal sloughing or a dark eschar. It is difficult to assess how much of the flap is viable when an eschar is present, but it is imperative to avoid debriding the area until the wound has healed. In some cases, only the epidermal portion of the flap necroses, and debriding the flap can disrupt underlying viable tissue. Even in cases of the flap has necrosis, the eschar over the wound will act as a biologic dressing that will allow the wound to heal by secondary intention.
As with any surgery, wound infection is a potential complication with rotational flap transfer. If a surgical site infection is suspected, the wound should be cultured, and the patient should be given an antibiotic with staphylococcal coverage until a culture and sensitivity are available. If there is a significant amount of purulent drainage, the wound may need to be opened, cleaned, and all foreign material, such as sutures, removed.
Dehiscence can occur as a result of excessive tension or from an infection. If a wound dehisces within 24 hours after surgery, another closure can be attempted; however, closures after this time may increase the risk of infection. Typically, dehisced wounds are allowed to heal by secondary intention, with revision considered after the wound has healed.
Bleeding is another potential complication. Fortunately, most cases can be controlled with firm, continuous pressure. In some instances, it may be necessary to reopen the wound to stop the bleeding. Bleeding can also result in hematoma formation. Stable hematomas can be drained or allowed to reabsorb over time. Hematomas may act as a nidus for infection, though, so antibiotic prophylaxis should be considered. Expanding hematomas should be treated by reopening the wound to evacuate the hematoma and stop any bleeding, putting pressure on the flap's pedicle and compromising its blood supply.[19]
Clinical Significance
With proper planning and execution, rotation flaps provide a range of options that can be used in several situations to produce excellent functional and cosmetic reconstructions of small to medium-sized soft tissue defects.
Enhancing Healthcare Team Outcomes
An interprofessional team consisting of a surgeon and a nurse will provide the best care for patients undergoing rotational flap transfer; a dermatologist and/or a surgical oncologist may also be involved in treating the lesion that initially led to the creation of the cutaneous defect that required rotational flap reconstruction. Clinicians, such as the surgeon and nurses experienced in wound management and postoperative care of local flaps, should follow the patient closely to identify early complications like infection, hematoma, and venous congestion and promptly manage these problems to mitigate long-term sequelae, exercising open communication if any concerns arise. [Level 5]
Media
(Click Image to Enlarge)
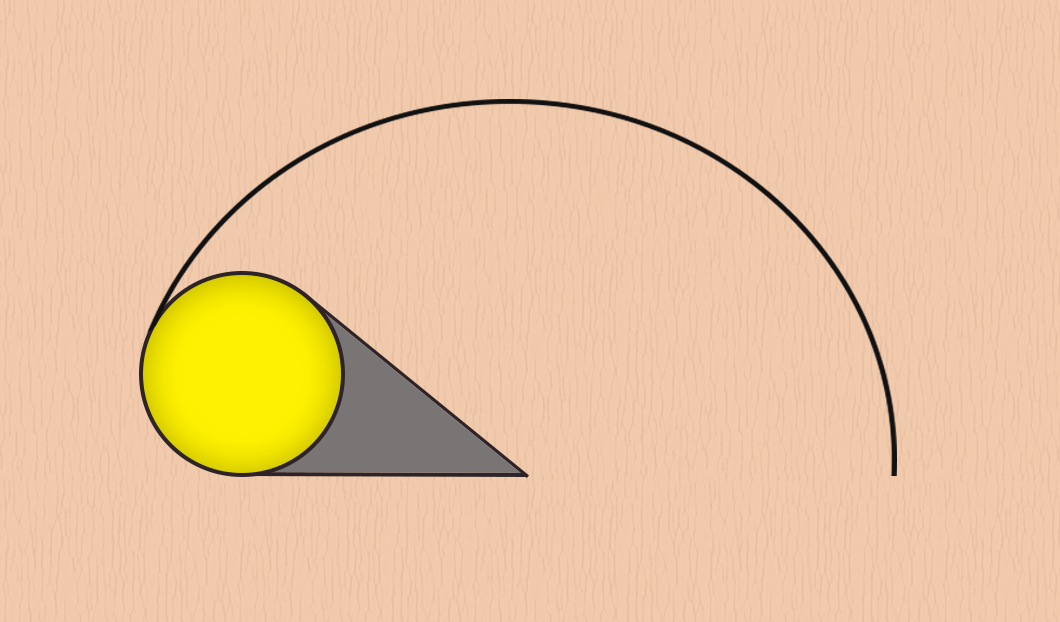
Figure 1. Illustration of a pure rotation flap
Illustrations courtesy of Anthony Burbatt. Reprinted with permission.
(Click Image to Enlarge)

Rotation Flap Reverse Sural Artery Flap for reconstruction of non-healing heel ulcer.
Contributed by Mark A. Dreyer, DPM, FACFAS
(Click Image to Enlarge)
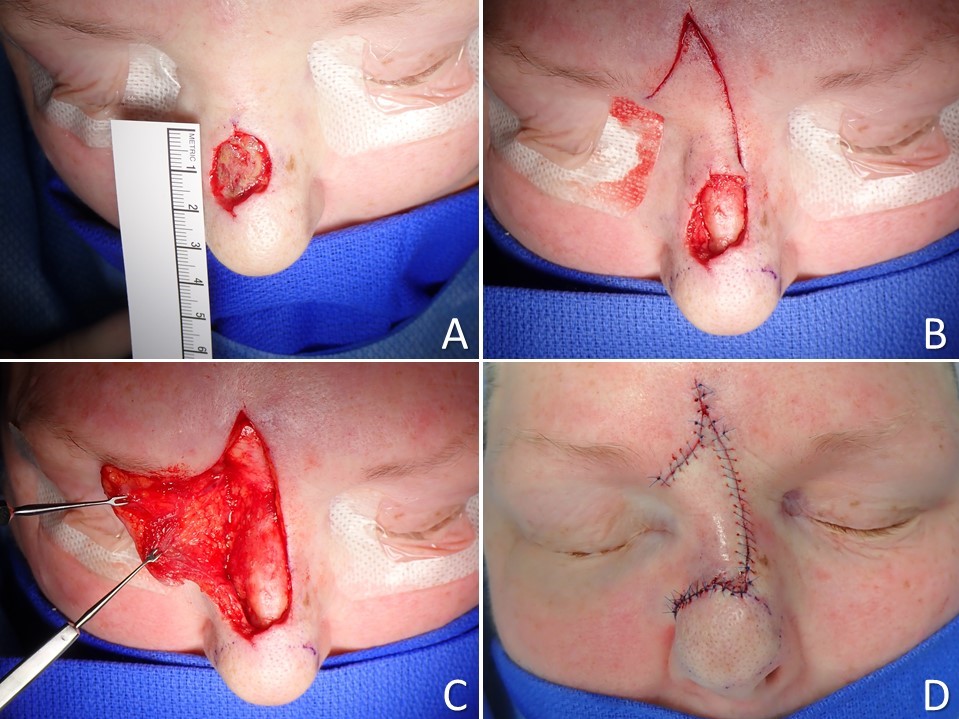
Rieger Dorsal Nasal Rotation-Advancement Flap. A) An approximate 2-cm defect of the nasal dorsum resulted from a Mohs resection of a basal cell carcinoma. B) The wound bed was excised down to the supraperichondrial plane to facilitate flap elevation, and the flap incisions were made to permit rotation as well as a V to Y advancement in the glabella. C) The flap is elevated in a supraperichondrial/supraperiosteal plane with care taken to avoid injuring the dorsal nasal and infratrochlear vessels that perfuse the flap. D) The flap is inset; note the slight resulting elevation of the nasal tip.
Contributed by Marc H Hohman, MD, FACS
(Click Image to Enlarge)
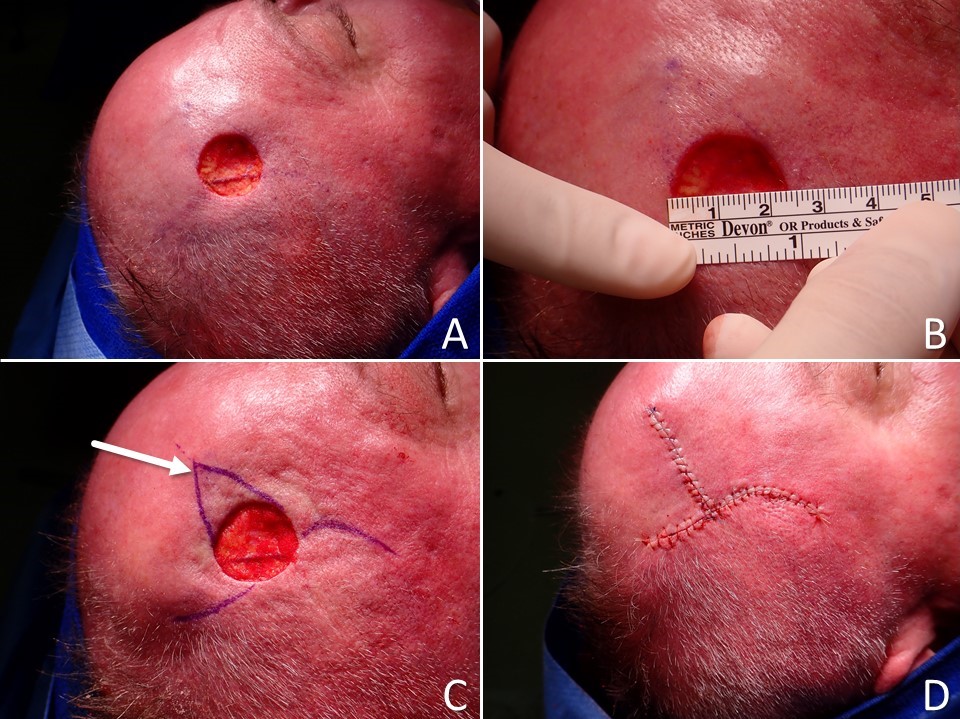
O to T Double Rotation Flap. A) circular full-thickness skin defect resulting from wide local excision of a melanoma. B) The defect measures 22 mm in diameter. C) Double rotation flaps are planned for closure with the inferior (right side of image) flap having an advancement component that permits the back cut to lie along the temporal hairline, and the superior flap (left side of image) having a more conventional design (the arrow indicates the triangular standing cutaneous deformity that will be removed). D) The defect is closed with the limbs of the incision well hidden along the hairline and within a transverse forehead rhytid.
Contributed by Marc H Hohman, MD, FACS
(Click Image to Enlarge)
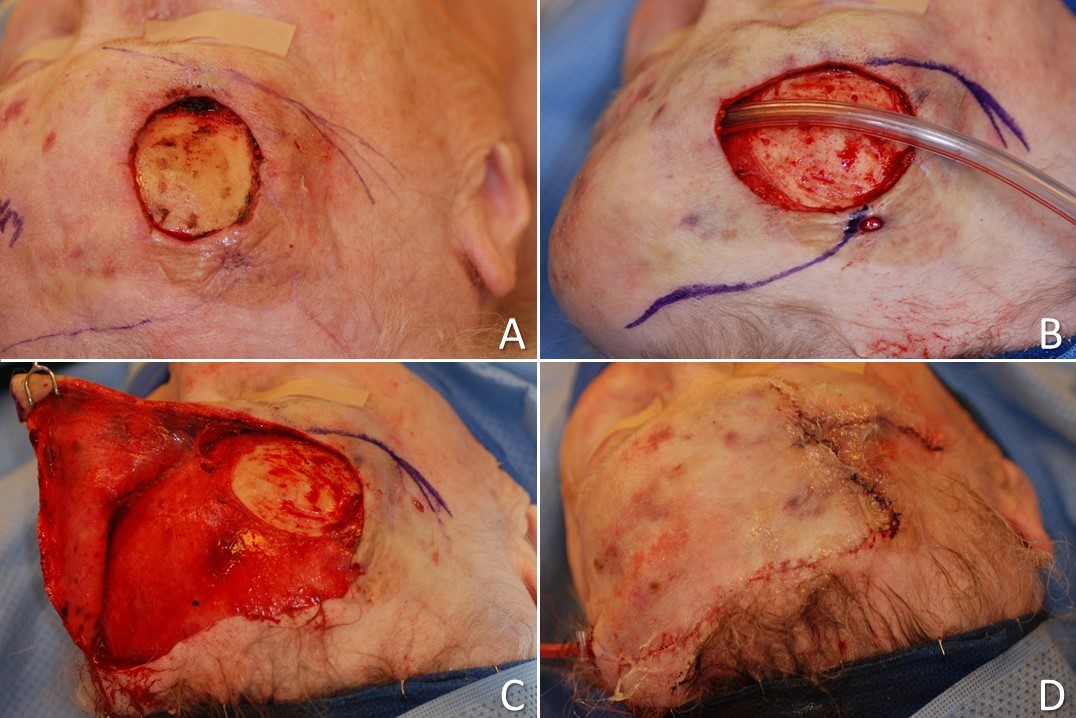
O to Z double rotation flap: A) circular full thickness defect with exposed calvarium due to recurrent and aggressive basal cell carcinoma measures ~3 cm in diameter, B) O to Z incisions are planned and intraoperative tissue expansion is performed using a Foley catheter balloon, C) the first flap is elevated in a subgaleal plane, D) the rotational flaps are transferred over a suction drain, leaving the characteristic Z-shaped scar.
Contributed by Marc H Hohman, MD, FACS and Wayne J Harsha, MD
References
Smoking increases facial skin flap complications., Kinsella JB,Rassekh CH,Wassmuth ZD,Hokanson JA,Calhoun KH,, The Annals of otology, rhinology, and laryngology, 1999 Feb [PubMed PMID: 10030230]
Level 2 (mid-level) evidenceA meta-analysis of complications attributed to anticoagulation among patients following cutaneous surgery., Lewis KG,Dufresne RG Jr,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2008 Feb [PubMed PMID: 18093204]
Level 1 (high-level) evidenceSerious adverse vascular events associated with perioperative interruption of antiplatelet and anticoagulant therapy., Alam M,Goldberg LH,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2002 Nov [PubMed PMID: 12460291]
Level 3 (low-level) evidenceControversies in perioperative management of blood thinners in dermatologic surgery: continue or discontinue?, Alcalay J,Alkalay R,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2004 Aug [PubMed PMID: 15274698]
The ideal rotation flap: an experimental study., Lo CH,Kimble FW,, Journal of plastic, reconstructive & aesthetic surgery : JPRAS, 2008 Jul [PubMed PMID: 18448409]
The dynamics of flap movement: effect of pivotal restraint on flap rotation and transposition., Dzubow LM,, The Journal of dermatologic surgery and oncology, 1987 Dec [PubMed PMID: 3680750]
The biomechanics of advancement and rotation flaps., Larrabee WF Jr,Sutton D,, The Laryngoscope, 1981 May [PubMed PMID: 7231022]
Level 3 (low-level) evidenceRotation Flaps-Principles and Locations., LoPiccolo MC,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2015 Oct [PubMed PMID: 26418690]
"Pinch modification" of the linear advancement flap., Peng VT,Sturm RL,Marsh TW,, The Journal of dermatologic surgery and oncology, 1987 Mar [PubMed PMID: 3546432]
The Peng flap: reviewed and refined., Ahern RW,Lawrence N,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2008 Feb [PubMed PMID: 18093195]
Level 2 (mid-level) evidenceRieger RA. A local flap for repair of the nasal tip. Plastic and reconstructive surgery. 1967 Aug:40(2):147-9 [PubMed PMID: 5340490]
Beyond Rieger's original indication; the dorsal nasal flap revisited., Eren E,Beden V,, Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery, 2014 Jul [PubMed PMID: 23830767]
The axial frontonasal flap revisited., Marchac D,Toth B,, Plastic and reconstructive surgery, 1985 Nov [PubMed PMID: 4059408]
Use of the spiral flap for closure of small defects of the lower eyelid., Lin H,Li W,, Annals of plastic surgery, 2009 Nov [PubMed PMID: 19801924]
The spiral flap for fingertip resurfacing: short-term and long-term results., Lim GJ,Yam AK,Lee JY,Lam-Chuan T,, The Journal of hand surgery, 2008 Mar [PubMed PMID: 18343289]
Level 2 (mid-level) evidenceThe spiral flap for nasal alar reconstruction: our experience with 63 patients., Mahlberg MJ,Leach BC,Cook J,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2012 Mar [PubMed PMID: 22093402]
Level 2 (mid-level) evidenceSpiral subcutaneous island pedicle advancement flap for repair of alar defects., Stoner JG,Stoner JG Jr,, Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.], 2005 Apr [PubMed PMID: 15871324]
Level 3 (low-level) evidenceThe Cervicofacial Flap in Cheek Reconstruction: A Guide for Flap Design., Al Shetawi AH,Quimby A,Fernandes R,, Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons, 2017 Dec [PubMed PMID: 28886355]
Woodard CR, Complications in facial flap surgery. Facial plastic surgery clinics of North America. 2013 Nov; [PubMed PMID: 24200378]