
Introduction
Chronic Thromboembolic Pulmonary Hypertension Overview
Chronic thromboembolic pulmonary hypertension (CTEPH) is a potentially life-threatening condition associated with high morbidity and mortality.[1] However, advances in medical and surgical treatments have markedly improved the outcomes.[2][3] CTEPH is a form of precapillary pulmonary hypertension associated with chronic thromboembolic disease. This condition falls under the World Health Organization's group 4 pulmonary hypertension classification.[4]
Acute pulmonary embolism, particularly when coupled with additional risk factors such as prothrombotic tendencies, recurrent thromboembolic events, genetic predisposition, and patient characteristics like comorbidities, has the potential to evolve into chronic thromboembolic disease over time. Chronic thromboembolism can result in CTEPH. Overt right heart failure can ensue if this condition is untreated at advanced stages. Thus, a low threshold is necessary when monitoring at-risk individuals for the development of CTEPH. Untreated cases eventually lead to significant functional capacity limitations and premature death due to worsening hemodynamics.[5][6]
Pulmonary Circulation
Understanding the anatomical features involved in CTEPH pathophysiology provides insights into how thromboembolic obstructions impact pulmonary hemodynamics, gas exchange, and right heart function. The pulmonary circulation involves the network of blood vessels transporting blood between the heart and lungs for oxygenation. This circulation begins at the right side of the heart. The right ventricle injects deoxygenated blood into the pulmonary arteries. The pulmonary arteries then branch into smaller vessels, eventually reaching the pulmonary capillaries within the lung parenchyma.
Gas exchange occurs in the pulmonary capillaries. Carbon dioxide is released from the capillary blood into the alveoli to be exhaled, while inhaled oxygen diffuses into the blood to be carried back to the heart. Once oxygenated, blood travels toward the left atrium via the pulmonary veins.
The pulmonary circulation is normally a low-pressure system compared to the systemic circulation. The right ventricle only needs to pump blood a short distance into the lungs' highly compliant blood vessels and back. This anatomy is well-adapted for efficient gas exchange, ensuring that blood is adequately oxygenated before systemic distribution. Additionally, the pulmonary vasculature is highly responsive to oxygen level changes, allowing for blood flow fine-tuning to match the body's metabolic demands.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Several theories regarding CTEPH's etiology exist. This condition develops similarly to deep vein thrombosis and acute pulmonary embolism in that organized thrombus material embolizes in the pulmonary circulation, causing vascular remodeling and subsequent pulmonary arterial hypertension. Current medical literature reports statistical associations with phospholipid antibodies, lupus anticoagulant, and elevated factor VIII levels, suggesting hypercoagulability and venous thrombosis state as predisposing factors.[7] Moreover, elevated levels of prothrombotic factor VIII were reported in 41% of patients with CTEPH.[8]
Multiple risk factors have been associated with CTEPH:[9]
- A previous history of pulmonary embolism (odds ratio is increased 19.0 times)
- Young age (odds ratio increases 1.79 times per decade of age)
- A large perfusion defect (odds ratio increases 2.22 times per decile decrement in perfusion on lung scan)
Acute pulmonary embolism is reported in nearly 90% of individuals with CTEPH, with recurrent pulmonary embolism found in almost half of all cases.[10] Pulmonary embolism clots usually resolve spontaneously to restore pulmonary circulation. However, the factors contributing to incomplete pulmonary embolus resolution in some cases remain unknown. Several mechanisms have been suggested, including difficulty in lysing large clots entirely or, in some cases, the embolic substance having more fibrin-rich material and red blood cells that make them more resistant to breakdown.
Other CTEPH risk factors include recurrent embolic events, thrombophilias, immunological disorders, ventriculoatrial shunts, pacemakers, peripherally inserted central catheter ("PICC lines"), malignancy, inflammatory bowel disease, splenectomy, chronic osteomyelitis, right ventricular dysfunction, large arterial thrombi, diabetes, hypothyroidism, younger age, acute pulmonary embolism with more significant perfusion defect, and idiopathic pulmonary embolism.[11][12] Determining whether these patients already harbored undiagnosed pulmonary hypertension or had CTEPH masquerading as acute pulmonary embolism presents a considerable challenge.[13]
Epidemiology
Limited studies delve into CTEPH's epidemiology.[14] The condition's incidence is estimated to be 2% to 6%, and its prevalence is around 26 to 38 cases per million.[15] The annual CTEPH incidence is estimated to be 1% at 6 months following pulmonary embolism and 3% at 1 year.[9] The development of CTEPH is rare 2 years after an acute pulmonary embolism episode.[16]
In the US, CTEPH's incidence after the initial pulmonary embolism event ranges from 0.1% to 9.1%.[17] A meta-analysis showed that <1% of all patients with a prior diagnosis of pulmonary embolism have CTEPH at the population level. CTEPH is frequently misdiagnosed, and its prevalence is underestimated due to limited clinician awareness and the so-called "honeymoon period"—the time interval between pulmonary embolism episodes and the onset of CTEPH symptoms.[18]
The European Society of Cardiology and the European Respiratory Society recently introduced a new term, "chronic thromboembolic pulmonary disease" (CTEPD), which is independent of the presence of pulmonary hypertension. Patients with CTEPD have similar symptoms, perfusion defects, and pulmonary vessel obstructions with or without pulmonary hypertension at rest. CTEPD is estimated to be present in 20% of individuals suspected of CTEPH.[19] These patients usually present younger than those with CTEPH and have a better functional status based on the 6-minute walk test distance.
Pathophysiology
The pathophysiology of CTEPH is still unclear. According to the generally accepted theory, CTEPH emerges following one or multiple pulmonary embolism episodes, predominantly from venous thrombosis.[20] The condition may also arise due to in situ thrombosis in the lung from primary arteriopathy and endothelial dysfunction, similar to PAH. This hypothesis may explain why up to 63% of patients with CTEPH do not have a history of acute pulmonary embolism (see Image. Chronic Thromboembolic Pulmonary Hypertension Proposed Pathophysiology).[21]
Histopathology
The histopathology slides of several patients diagnosed with CTEPH who underwent thromboendarterectomy show small vessel arteriopathy, microvascular thrombosis, intimal proliferation, and reduced pulmonary artery cross-sectional area from thrombosis.[22]
History and Physical
CTEPH symptoms may include breathlessness, chest pain, dizziness, fainting, and fatigue. These symptoms may be mild initially but can worsen without treatment. The most common presenting symptoms are exertional dyspnea and declining exercise tolerance. Other infrequent symptoms include cough, episodic hemoptysis, atypical chest pain, and palpitations.[23]
The physical examination may be nonspecific during CTEPH's early stages. In most cases, the diagnosis of CTEPH is established only in the later stages of the disease, when symptoms and signs of right ventricular dysfunction, such as peripheral edema, exertional chest pain, dyspnea during exercise, peripheral edema, dizziness, or syncopal episodes, have already appeared.
Auscultation findings include an accentuated second heart sound (P2), S4 gallop, and systolic ejection click over the pulmonary artery. However, the presence of pulmonary flow murmurs over the lung fields is more CTEPH-specific. This manifestation is described as subtle, high-pitched bruits with blowing quality, accentuated on inspiration and usually heard while holding the breath. These bruits arise from obstruction of medium-to-large pulmonary arteries.[24]
With the progression of pulmonary hypertension, a tricuspid regurgitation murmur, pedal edema, jugular venous distention, hepatomegaly, ascites, and other right ventricular failure symptoms appear. Hypoxemia is common in CTEPH due to ventilation-perfusion mismatching.[25] The level of hypoxia correlates with pulmonary vascular resistance, mean pulmonary artery pressure (PAP), and degree of vascular obstruction.
Evaluation
Diagnostic tests should be reserved for patients presenting with new or persistent symptoms, ie, dyspnea or exercise intolerance, after at least 3 months of anticoagulation.[26] Early diagnosis of this condition is challenging due to the initially nonspecific symptoms and delayed specific manifestations.
The initial evaluation of a dyspneic patient usually includes a chest x-ray, which may be normal in early CTEPH. In contrast, late CTEPH chest radiography often shows pulmonary hypertension signs, cardiac chamber enlargement, and segmental oligemia with pleuroparenchymal scarring.[27]
A CTEPH suspicion based on chest computed tomography (CT) findings of an obstructive thrombus, venous thromboembolism history, or characteristic bruits may be confirmed by ventilation/perfusion (V/Q) scanning, echocardiography, and pulmonary function tests. Diagnostic confirmation requires combining techniques, such as right heart catheterization and CT pulmonary angiography.
Transthoracic echocardiography primarily diagnoses pulmonary hypertension but is nonspecific, as it cannot differentiate between acute and chronic pulmonary embolism.[28] V/Q scanning has high sensitivity (90% to 100%) and specificity (94% to 100%) and is a first-line screening tool for diagnosing CTEPH.[29][30] Hence, a normal V/Q scan can reliably exclude the diagnosis of chronic venous thromboembolism. However, V/Q scanning may underestimate the size of pulmonary vascular obstruction in central locations and other V/Q mismatch etiologies.
Diagnostic criteria for CTEPH include mean PAP over 20 mm Hg, pulmonary arterial wedge pressure below 15 mm Hg, pulmonary vascular resistance greater than 3 Woods units (>240 dynes per second per cm), and evidence of chronic pulmonary embolism on CT or V/Q scan.
Right heart catheterization with conventional pulmonary angiography is the gold standard in diagnosing CTEPH, especially since a negative CT scan cannot exclude the condition.[31] Novel techniques such as dual-energy CT, dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), and optical coherence tomography are valuable diagnostic tools for evaluating patients with CTEPH. Digital subtraction techniques for pulmonary angiography are the gold standard in confirming a CTEPH diagnosis and determining surgical eligibility. The combination of different diagnostic tools can provide additional information and assist in ruling out other conditions, planning interventions, and assessing treatment response.
Treatment / Management
Patients with CTEPH should be evaluated and treated in an adequately equipped center by a specialized team of experts. All patients with suspected CTEPH should be prescribed anticoagulation for at least 3 months. The disease can regress during this period, and significant hemodynamic improvement or complete resolution of pulmonary hypertension may occur. Symptom resolution confirms a CTEPH diagnosis and distinguishes it from subacute pulmonary embolism, which often involves small pulmonary vessels. Diagnostic confirmation paves the way for definitive management.
Surgical Treatment
Pulmonary endarterectomy (PEA) is a complex surgical intervention in selected operable patients. The procedure can normalize pulmonary hemodynamics and improve exercise capacity and survival.[32] Individuals who may benefit from the surgery include patients consenting to the procedure or with proximal thromboembolic burden, minimal comorbidities, and significant hemodynamic and ventilatory impairments.[33]
The University of California-San Diego proposed a classification of CTEPH, which helps guide surgeons regarding the complexity and expertise needed for the treatment. The category level increases with increasing complexity. Level 0 includes patients without surgical evidence of chronic thromboembolic disease. Level 1 denotes blockade at the main pulmonary level. Levels 2, 3, and 4 show lobar, segmental, and subsegmental pulmonary artery obstruction, respectively.[34]
PEA removes obstructive and hardened thrombi and markedly improves hemodynamic measures such as mean PAP, pulmonary vascular resistance, and cardiac output. The procedure can reverse right ventricular remodeling due to right-sided cardiac function normalization.[35][36] CTEPH may persist in 5% to 35% of cases after PEA.[37] Notably, evidence suggests that patients may need to be on lifelong anticoagulation post-PEA to prevent further venous thromboembolism recurrence. Compared to direct-acting oral anticoagulants, vitamin K antagonists significantly lower recurrent thromboembolism risk.[38] Right ventricular function improves significantly after a PEA. Additionally, normalization of gas exchange, exercise capacity, and quality of life are reported.[33](B2)
More than 30% of the patients are inoperable. However, pulmonary balloon angioplasty (BPA) may be a promising alternative for these patients.[39][40] Studies on BPA's effect on CTEPH patients continue after some have been completed. The Expert Consensus on the Evaluation and Treatment of Pulmonary Hypertension Using Balloon Pulmonary Angioplasty plans to conduct an international observational study regarding BPA's effect on patients with CTEPH at rest and during exercise. The International BPA registry currently has an ongoing prospective study evaluating BPA's efficacy and safety on patients with CTEPH. A 2019 meta-analysis showed that BPA was superior to riociguat therapy in improving exercise intolerance and hemodynamic parameters.[41](A1)
BPA is known to cause general angioplasty complications like wire injury, vessel dissection, vessel rupture, and complications specific to lung angioplasty, including reperfusion pulmonary edema, pulmonary parenchymal bleeding, and hemothorax. However, the use of targeted vasodilators should be reserved for patients with right ventricular failure or severe pulmonary hypertension.
Medical Treatment
Current guidelines recommend using anticoagulants, diuretics, and oxygen if needed for optimal medical treatment of CTEPH. Patients with PEA contraindications or refractory pulmonary hypertension, despite surgical treatment, may improve pulmonary pressures from the targeted medical therapy riociguat. Bilateral lung transplantation is considered the last resort in people who are not PEA candidates, failed PEA, or have contraindications to targeted medical therapy with vasodilators.
Patients with a confirmed CTEPH diagnosis should be placed immediately on lifelong anticoagulation, which can also prevent in situ pulmonary artery thrombosis and further thromboembolism. The anticoagulants recommended by the Expert Panel and CHEST guidelines are as follows:
- First line: Direct oral anticoagulants dabigatran, rivaroxaban, apixaban or edoxaban
- Second line: Vitamin K antagonist therapy
- Third line: Low-molecular-weight heparin
Inferior vena cava filter placement should be considered in patients with CTEPH with an increased bleeding risk. Anticoagulation can be started once the bleeding tendency diminishes.[42]
PAH-targeted therapy in CTEPH includes the administration of endothelin-receptor antagonists, phosphodiesterase type-5 inhibitors, and prostanoids. Treprostinil and macitentan were extensively studied and proven beneficial in these patients.[43] The best PAH treatment option for individuals with CTEPH is riociguat, a guanylate-cyclase stimulator currently used in patients ineligible for surgery or with persistent disease post-PEA.(B3)
Differential Diagnosis
CTEPH is a curable disease, and clinicians should distinguish it from other conditions that may cause thrombotic and fibrotic pulmonary arterial changes. Notably, CTEPH must be differentiated from idiopathic pulmonary artery hypertension (IPAH).[44] On CT scan, IPAH lacks thromboembolic material or fibrotic obstructions in the pulmonary arteries but has significantly decreased segmental and subsegmental arterial diameter. A key IPAH finding is the presence of corkscrew-like pulmonary arteries, representing plexogenic arteriopathy.[45] A noninvasive test to differentiate between CTEPH and IPAH is possible using Doppler ultrasound. PAP waveforms differ significantly in patients with CTEPH and IPAH, with pulse pressure in CTEPH usually being markedly larger.
Another differential diagnosis is primary pulmonary arterial sarcoma, an extremely rare disease with nonspecific symptoms that make it hard to differentiate from CTEPH. Sarcoma appears as a solid lobulated mass in the central pulmonary arteries on CT or MRI and is unresponsive to anticoagulation treatment. Positron-emission tomography (PET) with F-fludeoxyglucose can be performed to distinguish sarcoma from CTEPH.[46]
In rare cases, right heart failure with acute pulmonary thromboembolism can mimic CTEPH. However, the emboli of acute thromboembolism form at an acute angle with the pulmonary artery wall, whereas the angle in CTEPH is often obtuse. Also, right ventricle hypertrophy, a chronic feature, is less likely to be seen in acute pulmonary embolism.[47]
Other CTEPH differential diagnoses include thrombosis in situ, Takayasu arteritis, congenital proximal pulmonary artery interruption, malignant and benign pulmonary artery tumors, Von Recklinghausen and Osler-Weber-Randu diseases, malignant and nonmalignant pulmonary artery tumors, arteritis, congenital pulmonary artery stenosis, and fibrosing mediastinitis.[48][49][50][51]
Prognosis
PEA is the best option for improving operable patients' survival rates. A 2017 study demonstrated the five-year survival rate after PEA to be 70% to 80%.[52] Hemodynamic severity and systolic PAP significantly improve after PEA.[53] The period between the last pulmonary embolism episode and PEA is considered a risk factor for in-hospital mortality, signifying the importance of timely diagnosis of CTEPH for a favorable outcome. CTEPH's long-term prognosis after surgical thrombus removal is currently excellent.
Complications
CTEPH itself is a complication of chronic thromboembolism. If left untreated, the condition can lead to severe right heart failure, significant shortness of breath, decreased exercise tolerance, syncope, and death, with a 3-year mortality rate estimated to be 90%.[51]
Deterrence and Patient Education
In the general population, preventive measures against acute pulmonary embolism help prevent CTEPH. Patients on prolonged hospitalization should be given appropriate anticoagulation during their visit. Inflatable compression devices or compression stockings may also help prevent clot formation. Individuals who travel frequently and have longer airplane time should ensure they walk about every 1 to 2 hours or change their seating positions regularly.
Meanwhile, patients diagnosed with CTEPH should be educated on medication adherence and follow-up before discharge. Close follow-up is crucial in patients with multiple comorbidities, as managing concurrent medical conditions helps significantly improve functional capacity. Patients traveling by air must be assessed for possible oxygen needs during the in-flight journey.
Pearls and Other Issues
CTEPH is a rare, dangerous, but potentially curable thromboembolic disease. The lack of predictable predisposing factors, including a prior medical history of acute pulmonary embolism, does not rule out this condition in patients with a progressive reduction in exercise tolerance. CTEPH should be considered in all patients with pulmonary hypertension, as this is the only potentially correctible PAH cause.
V/Q scanning is the first-line screening tool for diagnosing CTEPH. Diagnostic criteria for CTEPH include mean PAP greater than 20 mm Hg, pulmonary arterial wedge pressure less than 15 mm Hg, pulmonary vascular resistance greater than 3 Woods units, and evidence of chronic pulmonary embolism on CT, MRI, or V/Q scanning.
Current medical treatment for CTEPH primarily consists of PAH-targeted therapy and oral anticoagulation. PEA is the surgical treatment of choice in patients with CTEPH.
Enhancing Healthcare Team Outcomes
CTEPH is a difficult diagnosis, and the management is not straightforward. Treatment delays correlate with high mortality rates. Improved outcomes are evident with surgical treatments. All potential surgical candidates should undergo evaluation for surgical thromboendarterectomy. Clinicians should also be aware of the management options for patients who are not surgical candidates. Options include BPA, PAH-targeted medical therapy, and lifelong anticoagulation.
Primary care clinicians and nurses should educate patients on medication adherence and follow-up before discharge. Managing concurrent medical conditions helps significantly improve functional capacity in patients with multiple comorbidities; thus, close follow-up is crucial. If pharmacotherapy is indicated, a specialty pharmacist should assist with medication selection and dosing, especially when using novel agents. Clinicians and nurses should assess patients traveling by air for in-flight oxygen requirements.
Nurses and pharmacists should also be empowered to inform clinicians if thromboembolism prophylaxis may be indicated for hospitalized patients. Close communication between interprofessional team members is vital to ensure that the patient receives the current standard of care. The interprofessional team, including clinicians, specialists, nurses, and pharmacists, must collaborate to implement these measures and advance positive outcomes in treating CTEPH.
Media
(Click Image to Enlarge)
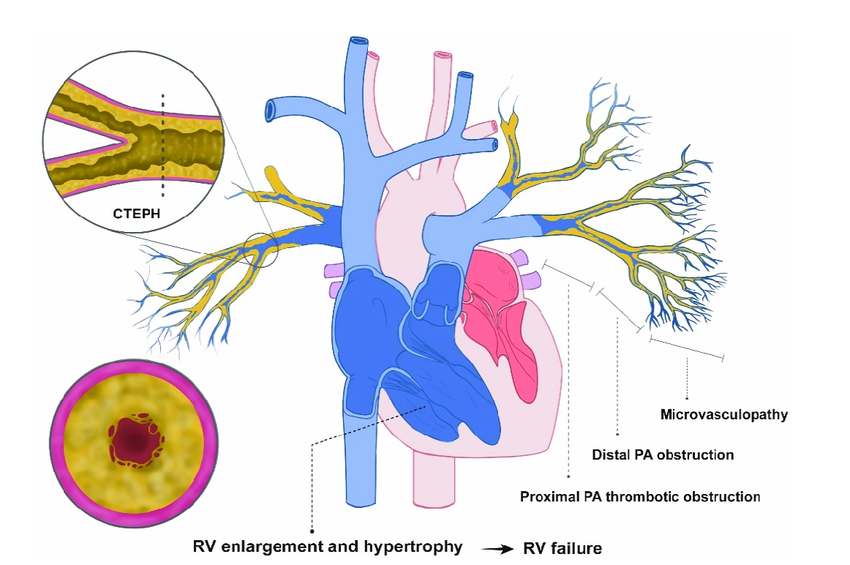
Chronic Thromboembolic Pulmonary Hypertension Proposed Pathophysiology. This illustration shows the proposed pathophysiology of chronic thromboembolic pulmonary hypertension. A thrombus or embolus chronically obstructs the distal and proximal pulmonary arteries. Chronically high pressures in the medium-to-large pulmonary arteries cause right ventricular enlargement and hypertrophy. Abbreviations: CTEPH — chronic thromboembolic pulmonary hypertension; PA — pulmonary artery; and RV — right ventricle.
Mi-Hyang Jung, Hae-Ok Jung, Soo Jin Kwon, Suyon Chang. Clinical presentations and multimodal imaging diagnosis in chronic thromboembolic pulmonary hypertension. J Clin Med. 2022;11(22):6678. doi: 10.3390/jcm11226678.
(https://creativecommons.org/licenses/by/4.0)
References
Becattini C, Agnelli G, Pesavento R, Silingardi M, Poggio R, Taliani MR, Ageno W. Incidence of chronic thromboembolic pulmonary hypertension after a first episode of pulmonary embolism. Chest. 2006 Jul:130(1):172-5 [PubMed PMID: 16840398]
Condliffe R, Kiely DG, Gibbs JS, Corris PA, Peacock AJ, Jenkins DP, Hodgkins D, Goldsmith K, Hughes RJ, Sheares K, Tsui SS, Armstrong IJ, Torpy C, Crackett R, Carlin CM, Das C, Coghlan JG, Pepke-Zaba J. Improved outcomes in medically and surgically treated chronic thromboembolic pulmonary hypertension. American journal of respiratory and critical care medicine. 2008 May 15:177(10):1122-7. doi: 10.1164/rccm.200712-1841OC. Epub 2008 Feb 21 [PubMed PMID: 18292468]
Level 2 (mid-level) evidenceNg C, Jenkins DP. Surgical management of chronic thromboembolic pulmonary hypertension. British journal of hospital medicine (London, England : 2005). 2013 Jan:74(1):31-5 [PubMed PMID: 23593675]
Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, Ferreira DS, Ghofrani HA, Giannakoulas G, Kiely DG, Mayer E, Meszaros G, Nagavci B, Olsson KM, Pepke-Zaba J, Quint JK, Rådegran G, Simonneau G, Sitbon O, Tonia T, Toshner M, Vachiery JL, Vonk Noordegraaf A, Delcroix M, Rosenkranz S, ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European heart journal. 2022 Oct 11:43(38):3618-3731. doi: 10.1093/eurheartj/ehac237. Epub [PubMed PMID: 36017548]
Oldroyd SH, Manek G, Sankari A, Bhardwaj A. Pulmonary Hypertension. StatPearls. 2024 Jan:(): [PubMed PMID: 29494070]
Farishta M, Sankari A. Pulmonary Hypertension Due to Lung Disease or Hypoxia. StatPearls. 2024 Jan:(): [PubMed PMID: 36508532]
Lang IM, Pesavento R, Bonderman D, Yuan JX. Risk factors and basic mechanisms of chronic thromboembolic pulmonary hypertension: a current understanding. The European respiratory journal. 2013 Feb:41(2):462-8. doi: 10.1183/09031936.00049312. Epub 2012 Jun 14 [PubMed PMID: 22700839]
Level 3 (low-level) evidenceBonderman D, Turecek PL, Jakowitsch J, Weltermann A, Adlbrecht C, Schneider B, Kneussl M, Rubin LJ, Kyrle PA, Klepetko W, Maurer G, Lang IM. High prevalence of elevated clotting factor VIII in chronic thromboembolic pulmonary hypertension. Thrombosis and haemostasis. 2003 Sep:90(3):372-6 [PubMed PMID: 12958604]
Level 2 (mid-level) evidencePengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, Albanese P, Biasiolo A, Pegoraro C, Iliceto S, Prandoni P, Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. The New England journal of medicine. 2004 May 27:350(22):2257-64 [PubMed PMID: 15163775]
Kerr KM, Elliott CG, Chin K, Benza RL, Channick RN, Davis RD, He F, LaCroix A, Madani MM, McLaughlin VV, Park M, Robbins IM, Tapson VF, Terry JR, Test VJ, Jain S, Auger WR. Results From the United States Chronic Thromboembolic Pulmonary Hypertension Registry: Enrollment Characteristics and 1-Year Follow-up. Chest. 2021 Nov:160(5):1822-1831. doi: 10.1016/j.chest.2021.05.052. Epub 2021 Jun 4 [PubMed PMID: 34090871]
Klok FA, Dzikowska-Diduch O, Kostrubiec M, Vliegen HW, Pruszczyk P, Hasenfuß G, Huisman MV, Konstantinides S, Lankeit M. Derivation of a clinical prediction score for chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Journal of thrombosis and haemostasis : JTH. 2016 Jan:14(1):121-8. doi: 10.1111/jth.13175. Epub 2015 Dec 29 [PubMed PMID: 26509468]
Pepke-Zaba J, Delcroix M, Lang I, Mayer E, Jansa P, Ambroz D, Treacy C, D'Armini AM, Morsolini M, Snijder R, Bresser P, Torbicki A, Kristensen B, Lewczuk J, Simkova I, Barberà JA, de Perrot M, Hoeper MM, Gaine S, Speich R, Gomez-Sanchez MA, Kovacs G, Hamid AM, Jaïs X, Simonneau G. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation. 2011 Nov 1:124(18):1973-81. doi: 10.1161/CIRCULATIONAHA.110.015008. Epub 2011 Oct 3 [PubMed PMID: 21969018]
Guérin L, Couturaud F, Parent F, Revel MP, Gillaizeau F, Planquette B, Pontal D, Guégan M, Simonneau G, Meyer G, Sanchez O. Prevalence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Prevalence of CTEPH after pulmonary embolism. Thrombosis and haemostasis. 2014 Sep 2:112(3):598-605. doi: 10.1160/TH13-07-0538. Epub 2014 Jun 5 [PubMed PMID: 24898545]
Catella-Chatron J, Merah A, De Magalhaes E, Moulin N, Accassat S, Duvillard C, Mismetti P, Bertoletti L. Chronic thromboembolic pulmonary hypertension suspicion after pulmonary embolism in cancer patients. Respiratory medicine and research. 2019 Nov:76():34-37. doi: 10.1016/j.resmer.2019.08.002. Epub 2019 Aug 27 [PubMed PMID: 31527015]
Leber L, Beaudet A, Muller A. Epidemiology of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: identification of the most accurate estimates from a systematic literature review. Pulmonary circulation. 2021 Jan-Mar:11(1):2045894020977300. doi: 10.1177/2045894020977300. Epub 2021 Jan 7 [PubMed PMID: 33456755]
Level 1 (high-level) evidenceEnde-Verhaar YM, Cannegieter SC, Vonk Noordegraaf A, Delcroix M, Pruszczyk P, Mairuhu AT, Huisman MV, Klok FA. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a contemporary view of the published literature. The European respiratory journal. 2017 Feb:49(2):. pii: 1601792. doi: 10.1183/13993003.01792-2016. Epub 2017 Feb 23 [PubMed PMID: 28232411]
Gall H, Hoeper MM, Richter MJ, Cacheris W, Hinzmann B, Mayer E. An epidemiological analysis of the burden of chronic thromboembolic pulmonary hypertension in the USA, Europe and Japan. European respiratory review : an official journal of the European Respiratory Society. 2017 Mar 31:26(143):. doi: 10.1183/16000617.0121-2016. Epub 2017 Mar 29 [PubMed PMID: 28356407]
Level 2 (mid-level) evidenceStrange G, Gabbay E, Kermeen F, Williams T, Carrington M, Stewart S, Keogh A. Time from symptoms to definitive diagnosis of idiopathic pulmonary arterial hypertension: The delay study. Pulmonary circulation. 2013 Jan:3(1):89-94. doi: 10.4103/2045-8932.109919. Epub [PubMed PMID: 23662179]
Swietlik EM, Ruggiero A, Fletcher AJ, Taboada D, Knightbridge E, Harlow L, Harvey I, Screaton N, Cannon JE, Sheares KKK, Ng C, Jenkins DP, Pepke-Zaba J, Toshner MR. Limitations of resting haemodynamics in chronic thromboembolic disease without pulmonary hypertension. The European respiratory journal. 2019 Jan:53(1):. pii: 1801787. doi: 10.1183/13993003.01787-2018. Epub 2019 Jan 17 [PubMed PMID: 30409818]
Peacock A, Simonneau G, Rubin L. Controversies, uncertainties and future research on the treatment of chronic thromboembolic pulmonary hypertension. Proceedings of the American Thoracic Society. 2006 Sep:3(7):608-14 [PubMed PMID: 16963542]
Hoeper MM, Mayer E, Simonneau G, Rubin LJ. Chronic thromboembolic pulmonary hypertension. Circulation. 2006 Apr 25:113(16):2011-20 [PubMed PMID: 16636189]
Piazza G, Goldhaber SZ. Chronic thromboembolic pulmonary hypertension. The New England journal of medicine. 2011 Jan 27:364(4):351-60. doi: 10.1056/NEJMra0910203. Epub [PubMed PMID: 21268727]
Gopalan D, Blanchard D, Auger WR. Diagnostic Evaluation of Chronic Thromboembolic Pulmonary Hypertension. Annals of the American Thoracic Society. 2016 Jul:13 Suppl 3():S222-39. doi: 10.1513/AnnalsATS.201509-623AS. Epub [PubMed PMID: 27571004]
Auger WR, Kerr KM, Kim NH, Fedullo PF. Evaluation of patients with chronic thromboembolic pulmonary hypertension for pulmonary endarterectomy. Pulmonary circulation. 2012 Apr-Jun:2(2):155-62. doi: 10.4103/2045-8932.97594. Epub [PubMed PMID: 22837856]
Kapitan KS, Buchbinder M, Wagner PD, Moser KM. Mechanisms of hypoxemia in chronic thromboembolic pulmonary hypertension. The American review of respiratory disease. 1989 May:139(5):1149-54 [PubMed PMID: 2712441]
Tapson VF, Platt DM, Xia F, Teal SA, de la Orden M, Divers CH, Satler CA, Joish VN, Channick RN. Monitoring for Pulmonary Hypertension Following Pulmonary Embolism: The INFORM Study. The American journal of medicine. 2016 Sep:129(9):978-985.e2. doi: 10.1016/j.amjmed.2016.03.006. Epub 2016 Apr 1 [PubMed PMID: 27046247]
Woodruff WW 3rd, Hoeck BE, Chitwood WR Jr, Lyerly HK, Sabiston DC Jr, Chen JT. Radiographic findings in pulmonary hypertension from unresolved embolism. AJR. American journal of roentgenology. 1985 Apr:144(4):681-6 [PubMed PMID: 3872021]
Ghio S, Raineri C, Scelsi L, Recusani F, D'armini AM, Piovella F, Klersy C, Campana C, Viganò M, Tavazzi L. Usefulness and limits of transthoracic echocardiography in the evaluation of patients with primary and chronic thromboembolic pulmonary hypertension. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2002 Nov:15(11):1374-80 [PubMed PMID: 12415231]
Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Revista espanola de cardiologia (English ed.). 2016 Feb:69(2):177. doi: 10.1016/j.rec.2016.01.002. Epub [PubMed PMID: 26837729]
Expert Panel on Thoracic Imaging:, Sirajuddin A, Donnelly EF, Crabtree TP, Henry TS, Iannettoni MD, Johnson GB, Kazerooni EA, Maldonado F, Olsen KM, Wu CC, Mohammed TL, Kanne JP. ACR Appropriateness Criteria(®) Suspected Pulmonary Hypertension. Journal of the American College of Radiology : JACR. 2017 May:14(5S):S350-S361. doi: 10.1016/j.jacr.2017.01.040. Epub [PubMed PMID: 28473092]
Kim NH, Delcroix M, Jais X, Madani MM, Matsubara H, Mayer E, Ogo T, Tapson VF, Ghofrani HA, Jenkins DP. Chronic thromboembolic pulmonary hypertension. The European respiratory journal. 2019 Jan:53(1):. doi: 10.1183/13993003.01915-2018. Epub 2019 Jan 24 [PubMed PMID: 30545969]
Jenkins D, Madani M, Fadel E, D'Armini AM, Mayer E. Pulmonary endarterectomy in the management of chronic thromboembolic pulmonary hypertension. European respiratory review : an official journal of the European Respiratory Society. 2017 Jan:26(143):. doi: 10.1183/16000617.0111-2016. Epub 2017 Mar 15 [PubMed PMID: 28298388]
Fedullo P, Kerr KM, Kim NH, Auger WR. Chronic thromboembolic pulmonary hypertension. American journal of respiratory and critical care medicine. 2011 Jun 15:183(12):1605-13. doi: 10.1164/rccm.201011-1854CI. Epub 2011 Feb 17 [PubMed PMID: 21330453]
Madani MM. Surgical Treatment of Chronic Thromboembolic Pulmonary Hypertension: Pulmonary Thromboendarterectomy. Methodist DeBakey cardiovascular journal. 2016 Oct-Dec:12(4):213-218. doi: 10.14797/mdcj-12-4-213. Epub [PubMed PMID: 28289496]
Corsico AG, D'Armini AM, Cerveri I, Klersy C, Ansaldo E, Niniano R, Gatto E, Monterosso C, Morsolini M, Nicolardi S, Tramontin C, Pozzi E, Viganò M. Long-term outcome after pulmonary endarterectomy. American journal of respiratory and critical care medicine. 2008 Aug 15:178(4):419-24. doi: 10.1164/rccm.200801-101OC. Epub 2008 Jun 12 [PubMed PMID: 18556630]
Reesink HJ, Marcus JT, Tulevski II, Jamieson S, Kloek JJ, Vonk Noordegraaf A, Bresser P. Reverse right ventricular remodeling after pulmonary endarterectomy in patients with chronic thromboembolic pulmonary hypertension: utility of magnetic resonance imaging to demonstrate restoration of the right ventricle. The Journal of thoracic and cardiovascular surgery. 2007 Jan:133(1):58-64 [PubMed PMID: 17198781]
Freed DH, Thomson BM, Berman M, Tsui SS, Dunning J, Sheares KK, Pepke-Zaba J, Jenkins DP. Survival after pulmonary thromboendarterectomy: effect of residual pulmonary hypertension. The Journal of thoracic and cardiovascular surgery. 2011 Feb:141(2):383-7. doi: 10.1016/j.jtcvs.2009.12.056. Epub 2010 May 13 [PubMed PMID: 20471039]
Bunclark K, Newnham M, Chiu YD, Ruggiero A, Villar SS, Cannon JE, Coghlan G, Corris PA, Howard L, Jenkins D, Johnson M, Kiely DG, Ng C, Screaton N, Sheares K, Taboada D, Tsui S, Wort SJ, Pepke-Zaba J, Toshner M. A multicenter study of anticoagulation in operable chronic thromboembolic pulmonary hypertension. Journal of thrombosis and haemostasis : JTH. 2020 Jan:18(1):114-122. doi: 10.1111/jth.14649. Epub 2019 Oct 18 [PubMed PMID: 31557382]
Level 2 (mid-level) evidenceMizoguchi H, Ogawa A, Munemasa M, Mikouchi H, Ito H, Matsubara H. Refined balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic pulmonary hypertension. Circulation. Cardiovascular interventions. 2012 Dec:5(6):748-55. doi: 10.1161/CIRCINTERVENTIONS.112.971077. Epub 2012 Nov 27 [PubMed PMID: 23192917]
Fukui S, Ogo T, Goto Y, Ueda J, Tsuji A, Sanda Y, Kumasaka R, Arakawa T, Nakanishi M, Fukuda T, Takaki H, Yasuda S, Ogawa H, Nakanishi N. Exercise intolerance and ventilatory inefficiency improve early after balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension. International journal of cardiology. 2015 Feb 1:180():66-8. doi: 10.1016/j.ijcard.2014.11.187. Epub 2014 Nov 26 [PubMed PMID: 25438215]
Level 3 (low-level) evidenceWang W, Wen L, Song Z, Shi W, Wang K, Huang W. Balloon pulmonary angioplasty vs riociguat in patients with inoperable chronic thromboembolic pulmonary hypertension: A systematic review and meta-analysis. Clinical cardiology. 2019 Aug:42(8):741-752. doi: 10.1002/clc.23212. Epub 2019 Jun 12 [PubMed PMID: 31188483]
Level 1 (high-level) evidenceKearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, Huisman M, King CS, Morris TA, Sood N, Stevens SM, Vintch JRE, Wells P, Woller SC, Moores L. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb:149(2):315-352. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7 [PubMed PMID: 26867832]
Zhang Y, Yu X, Jin Q, Luo Q, Zhao Z, Zhao Q, Yan L, Liu Z. Advances in targeted therapy for chronic thromboembolic pulmonary hypertension. Heart failure reviews. 2019 Nov:24(6):949-965. doi: 10.1007/s10741-019-09798-x. Epub [PubMed PMID: 31044326]
Level 3 (low-level) evidenceScheidl SJ, Englisch C, Kovacs G, Reichenberger F, Schulz R, Breithecker A, Ghofrani HA, Seeger W, Olschewski H. Diagnosis of CTEPH versus IPAH using capillary to end-tidal carbon dioxide gradients. The European respiratory journal. 2012 Jan:39(1):119-24. doi: 10.1183/09031936.00109710. Epub 2011 Jul 7 [PubMed PMID: 21737552]
Level 2 (mid-level) evidenceGrosse C, Grosse A. CT findings in diseases associated with pulmonary hypertension: a current review. Radiographics : a review publication of the Radiological Society of North America, Inc. 2010 Nov:30(7):1753-77. doi: 10.1148/rg.307105710. Epub [PubMed PMID: 21057119]
Bendel EC, Maleszewski JJ, Araoz PA. Imaging sarcomas of the great vessels and heart. Seminars in ultrasound, CT, and MR. 2011 Oct:32(5):377-404. doi: 10.1053/j.sult.2011.06.001. Epub [PubMed PMID: 21963161]
Wijesuriya S, Chandratreya L, Medford AR. Chronic pulmonary emboli and radiologic mimics on CT pulmonary angiography: a diagnostic challenge. Chest. 2013 May:143(5):1460-1471. doi: 10.1378/chest.12-1384. Epub [PubMed PMID: 23648910]
Nishiyama KH, Saboo SS, Tanabe Y, Jasinowodolinski D, Landay MJ, Kay FU. Chronic pulmonary embolism: diagnosis. Cardiovascular diagnosis and therapy. 2018 Jun:8(3):253-271. doi: 10.21037/cdt.2018.01.09. Epub [PubMed PMID: 30057874]
Njei B, Sanchez H. Neurofibromatosis type 1, recurrent pulmonary embolism, and a periampullary carcinoid tumor: is there a link? Connecticut medicine. 2013 Feb:77(2):77-80 [PubMed PMID: 23513634]
Level 3 (low-level) evidenceGuzman S, Khan MS, Chodakiewitz Y, Khan M, Chodakiewitz MS, Julien P, Luthringer DJ. Pulmonary capillary hemangiomatosis: a lesson learned. Autopsy & case reports. 2019 Jul-Sep:9(3):e2019111. doi: 10.4322/acr.2019.111. Epub 2019 Aug 22 [PubMed PMID: 31528628]
Hartopo AB, Dinarti LK, Wahab AS. The Challenge in Diagnosis and Current Treatment of Chronic Thromboembolic Pulmonary Hypertension. Acta medica Indonesiana. 2017 Apr:49(2):183-191 [PubMed PMID: 28790235]
Korsholm K, Andersen A, Mellemkjær S, Nielsen DV, Klaaborg KE, Ilkjær LB, Nielsen-Kudsk JE. Results from more than 20 years of surgical pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension in Denmark. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2017 Oct 1:52(4):704-709. doi: 10.1093/ejcts/ezx182. Epub [PubMed PMID: 28591785]
Segel MJ, Kogan A, Preissman S, Agmon-Levin N, Lubetsky A, Fefer P, Schaefers HJ, Raanani E. Pulmonary Endarterectomy Surgery for Chronic Thromboembolic Pulmonary Hypertension: A Small-Volume National Referral Center Experience. The Israel Medical Association journal : IMAJ. 2019 Aug:21(8):528-531 [PubMed PMID: 31474014]