
Introduction
Post-void residual volume (PVR) is the amount of urine retained in the bladder after a voluntary void and functions as a diagnostic tool. A PVR can be used to assess many disease processes, including but not limited to neurogenic bladder, cauda equina syndrome, urinary outlet obstruction, mechanical obstruction, medication-induced urinary retention, postoperative urinary retention, and urinary tract infections. The PVR may be determined through urinary catheterization, a portable dedicated bladder scanner, or a formal ultrasound examination. When used in conjunction with the American Urological Association (AUA) Symptom score and a 24-hour voiding diary, the PVR can provide clinicians a comprehensive understanding of the patient's bladder activity, functionality, and its association with symptoms, leading to an evidence-based diagnosis which guides directed therapy.
Specimen Collection
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Specimen Collection
A urine specimen is not always necessary or indicated but can aid in the diagnostic evaluation, especially if concern for infection is present as the etiology of the elevated residual volume. Performing urinary catheterization after voiding can provide both a post-void residual and a urine specimen. Catheterization is particularly useful when a urine specimen is needed and not otherwise obtainable, as well as in cases of apparent urinary retention. Urinary catheterization should be performed to prevent infection and to obtain an uncontaminated urine specimen.
Procedures
Measurement of the PVR immediately after voiding is crucial for an accurate result, with delays of as little as 10 minutes from bladder emptying to PVR determination causing clinically significant overestimation of the volume.[1]
Measurement of the PVR determines the quantity of urine remaining in the bladder shortly after a voluntary void; this measurement can be obtained using a portable dedicated bladder scanner, a formal bladder ultrasound examination, or by directly measuring the urine volume via urinary catheterization. Urinary catheterization is the gold standard for measuring the PVR but is invasive and has several other disadvantages compared to ultrasound.[2]
Portable Dedicated Bladder Ultrasound Device
A portable dedicated bladder ultrasound device, commonly known as a bladder scanner, uses ultrasound to measure the three-dimensional volume of urine in the bladder. The approach is simple and noninvasive to measure the PVR and is usually the preferred approach when available. In addition, the technique is simple to learn and takes only a few minutes to perform.
The device is easily portable on a movable stand, and a single instrument can serve an entire office or department. However, the device must be calibrated periodically, and the initial financial outlay may be significant. Nevertheless, while moderately expensive, the device has proven cost-effective over time and facilitates patient care in primary care facilities and specialist offices.
The technique of PVR measurement using a bladder scanner is straightforward. With the patient supine, ultrasound gel is placed on the suprapubic area. The probe is placed on the gel and directed toward the bladder. A simple button is depressed, which initiates the examination of the bladder volume. The result is displayed on a screen for the operator to see. The process can be repeated to align the bladder in the center of the display optimally. The largest bladder volume is recorded.[3]
Different bladder scanner machines may have slightly different procedures, but the basics of the technique are similar across devices. Bladder scanning is unsuitable for patients with severe abdominal scarring, prolapse of the uterus, significant ascites, or if currently pregnant.[4][5] Abdominal ascites may cause a falsely elevated measurement.[5]
Formal Bladder Ultrasound
Conventional ultrasound is used to visualize the bladder directly, using either a transabdominal or transvaginal approach. The PVR is measured using the ultrasound machine's internal volume calculations or the mathematical equation below. Transvaginal ultrasound appears especially accurate for measuring low bladder volumes.[6]
For transabdominal bladder volume evaluation, the probe is placed over the suprapubic area while the patient is prone. Bladder images are recorded in both the sagittal and transverse planes. The greatest transverse (width), anteroposterior (depth), and superior-inferior (height) distances are recorded (see Image. Bladder Dimensions Visualized on Ultrasound).[7]
An intracavitary transvaginal probe with frequencies between 7 to 9 MHz is used for transvaginal bladder volume evaluation. Ensure the probe is clean, has a probe cover, and has gel placed onto the end of the probe. The patient should be supine with the legs in stirrups or a pad under the pelvis. The probe is inserted into the vagina, and bladder identification is in the sagittal plane. Measurements are from the longest anteroposterior dimension and the craniocaudal dimension. The probe is then rotated 90° to measure the width or axial dimension.[8]
Most ultrasound machines have a function to automatically calculate volumes from the measurements used with the ultrasound calipers. The volumes can be calculated using the prolate ellipsoid formula if this function is unavailable. Multiple mathematical methods are used to calculate volume, and the prolate ellipsoid formula below is one commonly accepted method.[9][10]
Volume = length x width x height x 0.52
The prolate ellipsoid formula has more than one acceptable correction factor. The bladder is measured at its maximal transverse (width), longitudinal (length), and anterior-posterior (height) diameters. This method is recommended as the standard calculation because it is fast and easy.[10]
Data on the accuracy of transabdominal ultrasound for determining the PVR is mixed. Although most studies demonstrate high accuracy using transabdominal point-of-care ultrasound or bladder scanners with automated measurement of bladder volume, other recent studies have questioned the accuracy of these methods.[3][11][12][13][14] Some evidence indicates that dedicated bladder scanners are more accurate than two-dimensional ultrasound imaging.[7] For most practical purposes, an accurate measurement is not necessary for clinical decision-making, and a rough estimate is generally sufficient.
Urethral Catheterization
Urethral catheterization directly measures the PVR and is considered the gold measurement standard. Varying the size and type of catheter used may result in variable results.[5]
While accurate, the technique has some significant disadvantages. First, time and supplies are required. Second, the technique is invasive and requires a trained professional to perform. Third, the patient could be uncomfortable and risk a urinary tract infection or possible injury to the urethra. Fourth, unexpected difficulty in placing the catheter may be encountered, causing bleeding or other complications.
Finally, catheterization may not be possible in uncooperative individuals, babies, or children. However, it may be the optimal method when urinary retention is suspected or when noninvasive ultrasound equipment is unavailable or cannot be reliably used, as in patients with ascites or during the later stages of pregnancy.
While male and female anatomy each requires a different technique for inserting a urethral catheter, the overall procedure and sterile technique are similar. The steps in the technique are: [15][16]
- Perform hand hygiene and place the patient in an accessible position; a female patient should be placed in the frog-leg position while males can remain supine.
- Sterile drapes should cover the genitals with the urethral meatus exposed, and sterile gloves should be worn.
- The non-dominant hand should hold the penis at a 90-degree angle toward the ceiling, and for females, the labia should be separated and held to expose the urethral meatus.
- The urethral meatus and glans penis for males or perineum for females should undergo prepping with an antiseptic solution using a sterile technique.
- Injection of 20 mL of a local anesthetic gel, such as lidocaine, into the urethra can help diminish patient discomfort during the procedure.[17]
- Insert a well-lubricated catheter (usually 14 or 16 French in size) into the urethral meatus with the dominant, sterile-gloved hand.
- For male patients, pulling the penis downwards towards the feet while advancing the catheter will tend to straighten the natural anterior curve of the bulbous urethra and facilitate passage into the bladder.
- For female patients, if the urethral meatus is not visible, it can be found at the 12 o'clock position inside the vagina. If not visible, it may be located by palpation.
- Observe for a spontaneous urine return to confirm catheter tip placement within the bladder.
- To obtain a urine sample or PVR, allow the bladder to drain completely into a graduated container, measure the volume, and remove the catheter.
If permanent drainage is desired or the need appears likely, use a Foley catheter and inflate the balloon with sterile water after satisfactory placement.[18] Ensure the balloon portion of the Foley is entirely inside the bladder before inflation. This usually means a full catheter insertion up to the hub in male patients before balloon inflation.
Special techniques and procedures exist for complicated urethral catheterizations.[15]
Urethral catheterization has known complications. Common traumatic complications include urethral trauma, the creation of a false urethral passage, stricture formation, and inadvertent balloon inflation in the urethra. The precursor of catheter-associated urinary tract infection is bacteria, which develops at an average rate of 3% to 10% per day of catheterization. The commonly studied incidence of infection relates to indwelling catheterization and not in-and-out catheterization, which would identify a PVR or obtain a sterile urine sample.[19][20]
Comparison of Methods
While no statistically significant difference in PVR was found when measured using the bladder scanner or urinary catheterization, the average time to perform the bladder scan was 45 seconds. In contrast, the average urinary catheterization time was 293 seconds.[4] Portable bladder scanning for PVR measurement is convenient, noninvasive, accurate, cost-effective, and carries no risk of urethral trauma or urinary tract infection.[21] This is beneficial in various populations, including individuals with neurologic disease, children, babies, uncooperative patients, and the elderly, as well as other situations where catheterization is difficult or traumatic.[21]
Of note, some bladder scan machines include modifications to allow for the identification of abdominal aortic aneurysms. This makes the machines cost-effective for small primary care offices, not to mention finding potentially life-threatening aortic aneurysms that were missed.
Indications
A PVR is a valuable diagnostic tool for evaluating patients with urological symptoms such as urgency, frequency, incomplete emptying, weak urinary stream, suprapubic pain or pressure, bladder overactivity, incontinence, hesitancy, or stranguria. PVR can also be used for an underlying neurological disease or injury, bladder dysfunction, mechanical voiding obstruction, infection, or possible urinary retention.
The PVR is often best used with a 24-hour voiding diary and an AUA symptom score. Together, these non-invasive tools can provide the clinician with a clear understanding of urinary symptoms, bladder function, and emptying. Formal urodynamic testing can provide additional information, but this is costly, time-consuming, and often unnecessary with the optimal use of non-invasive diagnostic tools.
Symptoms of urinary retention and PVR can be indirect. Common symptoms of acute urinary retention are lower abdominal pain and inability to pass urine; in young children or elderly patients with dementia, who can provide only a limited history, agitation may be the only sign of bladder overdistension.[22] Determination of the PVR can identify patients with incontinence who have overflow due to urinary retention. It can also track the progress and treatment effectiveness of therapy for benign prostatic hyperplasia and other urinary disorders.
Additionally, patients with cauda equina syndrome may present with low back pain, saddle anesthesia, bilateral sciatica, motor weakness of the lower extremities, paraplegia, or incontinence; determination of the PVR may be of use.[23] Young children may have urinary retention due to a refusal to urinate because of the dysuria caused by a urinary tract infection or other causes.
Potential Diagnosis
Underlying causes of an elevated post-void residual volume include but are not limited to:
Neurogenic Causes
- Alcoholism
- Atonic detrusor
- Bladder denervation from pelvic surgery or other injuries
- Cauda equina syndrome
- Cerebrovascular accident
- Diabetic bladder neuropathy
- Detrusor-sphincter dyssynergia
- Fowler syndrome (inability to relax bladder sphincters)
- Heavy metal poisoning
- Multiple sclerosis
- Neurogenic bladder
- Parkinson disease
- Post-surgical urinary retention
- Spinal anesthesia
- Spinal cord injury
- Spinal nerve impingements (due to trauma, neoplasm, disc herniation, infection, or hematoma)
- Traumatic brain injury
- Vitamin B12 deficiency
Mechanical Causes
- Benign prostatic hyperplasia
- Bladder calculi
- Bladder neoplasm
- Blood clots
- Cystocele
- Detrusor underactivity
- Fecal impaction
- Phimosis and paraphimosis
- Prostate cancer
- Tumors
- Ureteral calculi
- Urethral strictures
- Uterine prolapse
Medication-related Causes
- Amphetamines
- Anticholinergics
- Antihistamines
- Antimuscarinics
- Botox injections of the bladder
- Cyclobenzaprine
- Decongestants
- Diazepam
- NSAIDs
- Opioids
- Tricyclic antidepressants
Infectious or Inflammatory Causes
- Cystitis
- Herpes simplex virus
- Local abscess
- Prostatitis
- Varicella zoster virus
- Vulvovaginitis
Congenital Causes
- Phimosis
- Posterior urethral valves
Anatomical Causes
- Foreign bodies in the urethra
- Large bladder diverticula
- Vesicoureteral reflux (causing rapid bladder refilling after voiding)
Normal and Critical Findings
A lack of consensus exists for both sexes about what constitutes a significantly elevated post-void residual volume, and conflicting data is present. Widely agreed-upon normal PVR values are provided.[24][25]
Adults and Older Adults
- Less than 100 mL PVR is considered normal.
- Up to 200 mL PVR may be acceptable.
- Over 200 mL PVR indicates inadequate emptying.
- Over 300 mL is suggestive of urinary retention.
- Over 400 mL is considered urinary retention.[26][27][28][29]
Children
Urinary Retention
- A PVR over 400 mL is considered abnormal and generally diagnostic of urinary retention. In addition, it may be highly predictive of cauda equina syndrome if associated with other neurological findings.
- A Foley catheter or intermittent self-catheterization is recommended.[33][34][35]
- Concern for possible post-obstructive diuresis exists if greater than 1,500 mL of urine is drained immediately.[36]
- Clamping the catheter during drainage of large bladder volumes is unneeded. The bladder drains typically at once, and interrupting the flow can cause spasms and inaccurate measurements of the actual post-void residual volume.
Interfering Factors
Limitations of Testing and Interfering Factors
When evaluating PVR volumes with ultrasonography, a false positive rate of 9% for urinary retention is present. This may be due to many factors, including pelvic masses such as ovarian cysts or uterine leiomyoma with cystic degeneration, ascites, scarring, device miscalibration, improper measuring technique, etc. No standard perfect calculation for measuring bladder volume exists; different measurement modalities and devices may produce different bladder volumes.
PVR measurements are recommended shortly after a voluntary void. Less than 10 minutes is optimal, but logistical problems often delay measurements for 20 minutes or longer. It is optimal if the patient indicates they must urinate rather than being forced to void on command to take a measurement.[2][7][10][11]
Complications
Urinary catheterization is the gold standard to measure PVR but has significant limitations such as patient discomfort, low compliance, invasiveness, and risk of urinary tract infection (UTI) or injury.[2] One study of females in the post-operative period found the overall prevalence of UTI after catheterization was 2.3%. Still, the risk of UTI rose the longer the catheter was in place.[37] In cases of urinary obstruction relieved by catheterization, post-obstructive diuresis (typically in cases of over 1,500 mL of retained urine) can cause hypovolemia and electrolyte abnormalities that may require admission for management.[36]
Patient Safety and Education
A PVR is a diagnostic tool to evaluate bladder function and detect underlying pathology. Bladder scanning and real-time transabdominal ultrasound are non-invasive and have no risk of ionizing radiation. Urethral catheterization carries some risks, including hematuria, urethral injury, discomfort, and infection, but may be preferred in certain situations, such as apparent urinary retention.
Clinical Significance
Although no definitive consensus definition of an elevated PVR exists, the procedure can help identify and diagnose urinary retention and verify good bladder emptying. This helps determine the proper management of various bladder disorders and prevents further discomfort, disability, or death. PVR measurement is often best used with a 24-hour voiding diary to help clarify multiple voiding dysfunctions and differentiate polyuria, overactive bladder, and overflow incontinence.
The appropriate and optimal use of post-void residual determinations is the early and correct diagnosis of urinary retention and other bladder disorders. Since this is often done non-invasively with dedicated ultrasonic scanners, it provides valuable evidence of bladder emptying ability and can be used to track therapy. It has proven useful in almost every type of urinary disorder.
Measurement of the post-void residual urine volume is one of a handful of evidence-based, non-invasive diagnostic tools available to the clinician to treat various urinary symptoms that could be caused by many, sometimes contradictory, disorders.
Neurological Injury
Cauda equina syndrome is a serious condition that, if not managed expeditiously, leaves many patients with long-term neurological deficits. Urinary retention is considered a late sign predictive of paralysis, insensate bladder and bowel, and loss of sexual function.[38] One researcher found patients diagnosed with cauda equina with the sole findings of urinary retention and absent ankle reflexes with no other obvious neurological abnormalities.[26]
Long-standing neurogenic bladder can lead to loss of bladder compliance and refractory urinary incontinence, pyelonephritis, and possible renal function deterioration over time.[39] Non-neurologic causes of a sizeable post-void residual can cause bladder muscle damage.
Infection
Conflicting data exist, but one study of stroke patients found a higher rate of UTIs developed in patients with a PVR over 100 ml.[40]
Obstruction
One researcher found that 9.5% of admitted patients to a geriatric unit with acute kidney injury had a pre-existing renal disease caused by obstructive uropathy.[41] Bladder outlet obstruction, namely benign prostatic hyperplasia, leads to profound changes and permanent damage to bladder structure and function, which may be irreversible.[42]
Media
(Click Image to Enlarge)
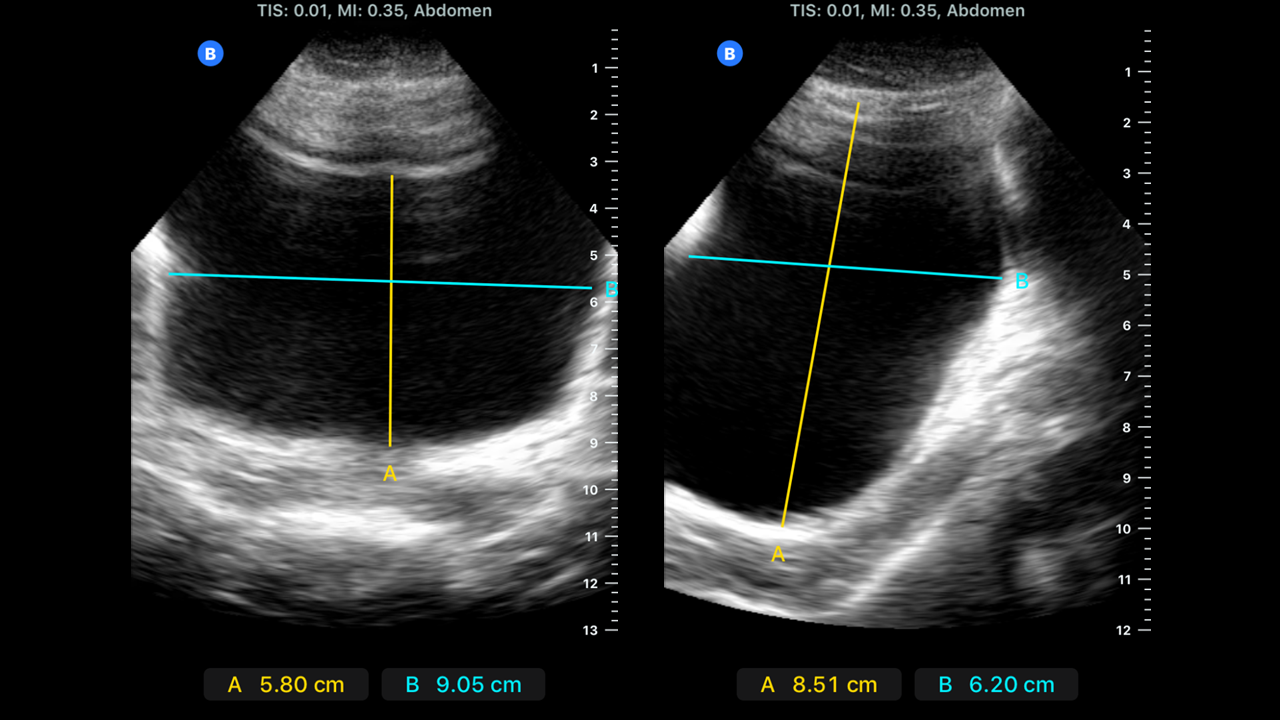
Bladder Dimensions Visualized on Ultrasound. Bladder dimensions in sagittal and transverse views to determine PVR using ultrasound.
Contributed by MK Herbst, MD
References
Haylen BT, Lee J. The accuracy of post-void residual measurement in women. International urogynecology journal and pelvic floor dysfunction. 2008 May:19(5):603-6. doi: 10.1007/s00192-008-0568-0. Epub 2008 Feb 27 [PubMed PMID: 18301853]
Kim TH, Kim HS, Park JW, Lim OK, Park KD, Lee JK. Falsely Elevated Postvoid Residual Urine Volume in Uterine Myoma. Annals of rehabilitation medicine. 2017 Apr:41(2):332-336. doi: 10.5535/arm.2017.41.2.332. Epub 2017 Apr 27 [PubMed PMID: 28503470]
Bent AE, Nahhas DE, McLennan MT. Portable ultrasound determination of urinary residual volume. International urogynecology journal and pelvic floor dysfunction. 1997:8(4):200-2 [PubMed PMID: 9449296]
Teng CH, Huang YH, Kuo BJ, Bih LI. Application of portable ultrasound scanners in the measurement of post-void residual urine. The journal of nursing research : JNR. 2005 Sep:13(3):216-24 [PubMed PMID: 16237633]
Level 2 (mid-level) evidenceHaylen BT, Frazer MI, MacDonald JH. Assessing the effectiveness of different urinary catheters in emptying the bladder: an application of transvaginal ultrasound. British journal of urology. 1989 Oct:64(4):353-6 [PubMed PMID: 2684335]
Haylen BT. Verification of the accuracy and range of transvaginal ultrasound in measuring bladder volumes in women. British journal of urology. 1989 Oct:64(4):350-2 [PubMed PMID: 2684334]
Byun SS, Kim HH, Lee E, Paick JS, Kamg W, Oh SJ. Accuracy of bladder volume determinations by ultrasonography: are they accurate over entire bladder volume range? Urology. 2003 Oct:62(4):656-60 [PubMed PMID: 14550437]
Rachaneni S, McCooty S, Middleton LJ, Parker VL, Daniels JP, Coomarasamy A, Verghese TS, Balogun M, Goranitis I, Barton P, Roberts TE, Deeks JJ, Latthe P, Bladder Ultrasound Study (BUS) Collaborative Group. Bladder ultrasonography for diagnosing detrusor overactivity: test accuracy study and economic evaluation. Health technology assessment (Winchester, England). 2016 Jan:20(7):1-150. doi: 10.3310/hta20070. Epub [PubMed PMID: 26806032]
Dicuio M, Pomara G, Menchini Fabris F, Ales V, Dahlstrand C, Morelli G. Measurements of urinary bladder volume: comparison of five ultrasound calculation methods in volunteers. Archivio italiano di urologia, andrologia : organo ufficiale [di] Societa italiana di ecografia urologica e nefrologica. 2005 Mar:77(1):60-2 [PubMed PMID: 15906795]
Hvarness H, Skjoldbye B, Jakobsen H. Urinary bladder volume measurements: comparison of three ultrasound calculation methods. Scandinavian journal of urology and nephrology. 2002:36(3):177-81 [PubMed PMID: 12201931]
Ouslander JG, Simmons S, Tuico E, Nigam JG, Fingold S, Bates-Jensen B, Schnelle JF. Use of a portable ultrasound device to measure post-void residual volume among incontinent nursing home residents. Journal of the American Geriatrics Society. 1994 Nov:42(11):1189-92 [PubMed PMID: 7963206]
Park YH, Ku JH, Oh SJ. Accuracy of post-void residual urine volume measurement using a portable ultrasound bladder scanner with real-time pre-scan imaging. Neurourology and urodynamics. 2011 Mar:30(3):335-8. doi: 10.1002/nau.20977. Epub [PubMed PMID: 20658544]
Mainprize TC, Drutz HP. Accuracy of total bladder volume and residual urine measurements: comparison between real-time ultrasonography and catheterization. American journal of obstetrics and gynecology. 1989 Apr:160(4):1013-6 [PubMed PMID: 2653036]
Alnaif B, Drutz HP. The accuracy of portable abdominal ultrasound equipment in measuring postvoid residual volume. International urogynecology journal and pelvic floor dysfunction. 1999:10(4):215-8 [PubMed PMID: 10450819]
Bianchi A, Leslie SW, Chesnut GT. Difficult Foley Catheterization. StatPearls. 2024 Jan:(): [PubMed PMID: 33232074]
Haider MZ, Annamaraju P. Bladder Catheterization. StatPearls. 2024 Jan:(): [PubMed PMID: 32809583]
Meconi A, Butcher R. Local Anesthetic for Urinary Catheter Insertion: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. 2020 Feb 27:(): [PubMed PMID: 33074606]
Clayton JL. Indwelling Urinary Catheters: A Pathway to Health Care-Associated Infections. AORN journal. 2017 May:105(5):446-452. doi: 10.1016/j.aorn.2017.02.013. Epub [PubMed PMID: 28454610]
Bhatt NR, Davis NF, Addie D, Flynn R, McDermott TED, Manecksha RP, Thornhill JA. Evaluating the cost of iatrogenic urethral catheterisation injuries. Irish journal of medical science. 2017 Nov:186(4):1051-1055. doi: 10.1007/s11845-016-1451-5. Epub 2016 Apr 6 [PubMed PMID: 27052967]
Chenoweth C, Saint S. Preventing catheter-associated urinary tract infections in the intensive care unit. Critical care clinics. 2013 Jan:29(1):19-32. doi: 10.1016/j.ccc.2012.10.005. Epub [PubMed PMID: 23182525]
Kelly CE. Evaluation of voiding dysfunction and measurement of bladder volume. Reviews in urology. 2004:6 Suppl 1(Suppl 1):S32-7 [PubMed PMID: 16985853]
Thomas K, Chow K, Kirby RS. Acute urinary retention: a review of the aetiology and management. Prostate cancer and prostatic diseases. 2004:7(1):32-7 [PubMed PMID: 14999235]
Orendácová J, Cízková D, Kafka J, Lukácová N, Marsala M, Sulla I, Marsala J, Katsube N. Cauda equina syndrome. Progress in neurobiology. 2001 Aug:64(6):613-37 [PubMed PMID: 11311464]
Level 3 (low-level) evidenceKaplan SA, Wein AJ, Staskin DR, Roehrborn CG, Steers WD. Urinary retention and post-void residual urine in men: separating truth from tradition. The Journal of urology. 2008 Jul:180(1):47-54. doi: 10.1016/j.juro.2008.03.027. Epub 2008 May 15 [PubMed PMID: 18485378]
Asimakopoulos AD, De Nunzio C, Kocjancic E, Tubaro A, Rosier PF, Finazzi-Agrò E. Measurement of post-void residual urine. Neurourology and urodynamics. 2016 Jan:35(1):55-7. doi: 10.1002/nau.22671. Epub 2014 Sep 22 [PubMed PMID: 25251215]
Sakakibara R, Yamamoto T, Uchiyama T, Liu Z, Ito T, Yamazaki M, Awa Y, Yamanishi T, Hattori T. Is lumbar spondylosis a cause of urinary retention in elderly women? Journal of neurology. 2005 Aug:252(8):953-7 [PubMed PMID: 15778810]
Level 2 (mid-level) evidenceAlagiakrishnan K, Valpreda M. Ultrasound bladder scanner presents falsely elevated postvoid residual volumes. Canadian family physician Medecin de famille canadien. 2009 Feb:55(2):163-4 [PubMed PMID: 19221075]
Level 3 (low-level) evidenceKolman C, Girman CJ, Jacobsen SJ, Lieber MM. Distribution of post-void residual urine volume in randomly selected men. The Journal of urology. 1999 Jan:161(1):122-7 [PubMed PMID: 10037383]
Shimoni Z, Fruger E, Froom P. Measurement of post-void residual bladder volumes in hospitalized older adults. The American journal of medicine. 2015 Jan:128(1):77-81. doi: 10.1016/j.amjmed.2014.08.018. Epub 2014 Sep 3 [PubMed PMID: 25193275]
Level 2 (mid-level) evidenceChung KL, Chao NS, Liu CS, Tang PM, Liu KK, Leung MW. Abnormal voiding parameters in children with severe idiopathic constipation. Pediatric surgery international. 2014 Jul:30(7):747-9. doi: 10.1007/s00383-014-3511-0. Epub 2014 May 15 [PubMed PMID: 24828888]
Chang SJ, Yang SS. Variability, related factors and normal reference value of post-void residual urine in healthy kindergarteners. The Journal of urology. 2009 Oct:182(4 Suppl):1933-8. doi: 10.1016/j.juro.2009.02.086. Epub 2009 Aug 20 [PubMed PMID: 19695621]
Chang SJ, Chiang IN, Hsieh CH, Lin CD, Yang SS. Age- and gender-specific nomograms for single and dual post-void residual urine in healthy children. Neurourology and urodynamics. 2013 Sep:32(7):1014-8. doi: 10.1002/nau.22342. Epub 2013 Apr 17 [PubMed PMID: 23595887]
Level 2 (mid-level) evidenceDomen PM, Hofman PA, van Santbrink H, Weber WE. Predictive value of clinical characteristics in patients with suspected cauda equina syndrome. European journal of neurology. 2009 Mar:16(3):416-9. doi: 10.1111/j.1468-1331.2008.02510.x. Epub [PubMed PMID: 19490073]
Level 2 (mid-level) evidenceLeslie SW, Rawla P, Dougherty JM. Female Urinary Retention. StatPearls. 2024 Jan:(): [PubMed PMID: 30860732]
Dougherty JM, Aeddula NR. Male Urinary Retention. StatPearls. 2024 Jan:(): [PubMed PMID: 30860734]
Leslie SW, Sajjad H, Sharma S. Postobstructive Diuresis. StatPearls. 2024 Jan:(): [PubMed PMID: 29083564]
Karp NE, Kobernik EK, Kamdar NS, Fore AM, Morgan DM. Length of Catheter Use After Hysterectomy as a Risk Factor for Urinary Tract Infection. Female pelvic medicine & reconstructive surgery. 2018 Nov/Dec:24(6):430-434. doi: 10.1097/SPV.0000000000000486. Epub [PubMed PMID: 28914703]
Todd NV. Guidelines for cauda equina syndrome. Red flags and white flags. Systematic review and implications for triage. British journal of neurosurgery. 2017 Jun:31(3):336-339. doi: 10.1080/02688697.2017.1297364. Epub 2017 Mar 2 [PubMed PMID: 28637110]
Level 1 (high-level) evidenceNseyo U, Santiago-Lastra Y. Long-Term Complications of the Neurogenic Bladder. The Urologic clinics of North America. 2017 Aug:44(3):355-366. doi: 10.1016/j.ucl.2017.04.003. Epub [PubMed PMID: 28716317]
Kim BR, Lim JH, Lee SA, Kim JH, Koh SE, Lee IS, Jung H, Lee J. The Relation between Postvoid Residual and Occurrence of Urinary Tract Infection after Stroke in Rehabilitation Unit. Annals of rehabilitation medicine. 2012 Apr:36(2):248-53. doi: 10.5535/arm.2012.36.2.248. Epub 2012 Apr 30 [PubMed PMID: 22639750]
Tseng TY, Stoller ML. Obstructive uropathy. Clinics in geriatric medicine. 2009 Aug:25(3):437-43. doi: 10.1016/j.cger.2009.06.003. Epub [PubMed PMID: 19765491]
Mirone V, Imbimbo C, Longo N, Fusco F. The detrusor muscle: an innocent victim of bladder outlet obstruction. European urology. 2007 Jan:51(1):57-66 [PubMed PMID: 16979287]