
Introduction
Lupus erythematosus is an autoimmune disease that has an array of clinical manifestations ranging from cutaneous to multi-organ systemic involvement. Bullous systemic lupus erythematosus (BSLE) is a rare blistering eruption seen in patients with systemic lupus erythematosus (SLE) described mainly in case reports, series, and a few multicenter retrospective studies. These cutaneous lesions appear as tense, vesiculobullous eruptions with a predilection for the extremities, trunk, face, and neck, usually healing without scar or milia.[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of bullous systemic lupus erythematosus is unknown. It is an uncommon complication of SLE with autoantibodies to the dermo-epidermal junction of type VII collagen. Most patients with BSLE have an existing diagnosis of SLE, although there are several reports of BSLE as an initial presentation of SLE.[2][3]
Epidemiology
Bullous systemic lupus erythematosus, in line with the epidemiology of SLE, affects more females than males, usually of African descent in the second to the fourth decade of life. Nevertheless, it can be seen in all races, ages, or males. The reported incidence is limited but estimated at ~2% of all subepidermal autoimmune bullous cutaneous conditions.[4][5]
Pathophysiology
Autoantibodies to type VII collagen are involved in the pathophysiology of bullous systemic lupus erythematosus. This results in a weakened basement membrane-dermal adhesion, which appears as subepidermal blistering. Type VII collagen plays a vital role as an anchoring fibril attaching the epidermis to the dermis. The circulating autoantibodies are directed against the non-collagenous domain type 1 and 2 (NC1 and NC2) of type VII collagen seen in the basement membrane zone.[2][6] Other autoantibodies have been identified, such as BPAg1, laminin 5, laminin 6, and BPAg2.[7]
Histopathology
The histopathology of bullous systemic lupus erythematosus demonstrates subepidermal blistering with a dense neutrophilic infiltration in the upper dermis concentrated on the papillary tip with the association of nuclear dust and fibrin. These findings have a similarity to the histology of dermatitis herpetiformis. However, a good distinguishing feature is the presence of large deposits of mucin in the reticular dermis.[8][9]
Direct immunofluorescence (DIF) staining of perilesional and uninvolved skin shows the deposition of immune-reactants along the dermato-epidermal junction (DEJ). IgG constitutes the majority of immunoglobulins, but other classes such as IgA and IgM are seen. Complements are frequently seen in the involved skin. Granular, linear, or a mixed pattern of immune reactant deposition are seen in the basement membrane zone (BMZ). Indirect immunofluorescence staining performed with basement membrane zone-split skin may also be positive for antibodies to type VII collagen on the dermal side.[9] IgG subtyping can help differentiate the two.[10]
History and Physical
Bullous systemic lupus erythematosus is often an acute onset presentation with tense vesicles and bullae over erythematous or normal skin. These blisters appear more in sun-exposed areas but can be seen in non-sun-exposed skin and mucosa with a predilection for the trunk, face, neck, vermillion border, upper extremities-extensor surfaces, supraclavicular region, and oral mucosa.[4][11]
A rare pattern, erythema gyratum repens described as a centrifugally migrating erythematous plaque, has been described.[12][13]
BSLE may be associated with urticarial lesions, and pruritus is not always present. Healing with milia and/or scarring occurs infrequently. However, hypo/hyperpigmentation of the affected skin is usually seen.[8]
Several reports have shown an association with BSLE and active lupus nephritis. A multicenter retrospective study and literature review with a total of 128 cases described lupus nephritis in 50% of the cases, mainly class III or IV. 7% of cases had neuropsychiatric SLE and 45% with hematologic involvement at the time of BSLE.[8]
Evaluation
A careful review of the clinical presentation, serologies, histology, and immunofluorescence is required in the process of diagnosis.
In 1983 Camisa and Sharma proposed the following diagnostic criteria for bullous systemic lupus erythematosus, which was later revised in 1986:[14][15]
- A diagnosis of SLE based on the American College of Rheumatology (ACR) criteria
- Vesicles and bullae arising upon but not limited to sun-exposed skin
- Histopathology compatible with dermatitis herpetiformis (DH)
- Negative or positive indirect immunofluorescence (IIF) for circulating BMZ autoantibodies
- Direct immunofluorescence (DIF) revealing IgG and/or IgM and often IgA at the BMZ
In 1995, Yell et al. l described BSLE as "an acquired subepidermal blistering disease in a patient with SLE with immune reactants at the BMZ on either DIF or IIF."[11]
Detection of an autoantibody directed against collagen VII was shown to play a role in BSLE. The criteria by Camisa and Sharma were made before the availability of ELISA or immunoblot technology. The use of ELISA for detecting antibodies against NC1 and NC2 of type VII collagen is utilized.[16]
However, it is important to note that a diagnosis of SLE is usually present; however, this may be the first presentation of SLE in a few cases. A thorough exclusion of other blistering diseases should also be completed.
Treatment / Management
Dapsone is considered the first line of treatment with a good response.[17]
The use of dapsone, however, may have a few side effects, including but not limited to anemia, hepatitis, or hypersensitivity syndrome. In the event of intolerance, systemic manifestation, or extensive skin involvement, the use of steroids may be considered.
Several steroid-sparing agents have been used in the literature with variable efficacy. These immunosuppressive medications include cyclophosphamide, azathioprine, mycophenolate mofetil, methotrexate, with modest results. Rituximab has shown some promise with refractory cases.
Less infrequently, anakinra and intravenous immunoglobulins have been reported.[8](B3)
Differential Diagnosis
Bullous systemic lupus erythematosus may be confused with several other blistering diseases, especially two autoimmune blistering conditions: dermatitis herpetiformis (DH) or epidermolysis bullosa acquisita (EBA).
Epidermolysis bullosa acquisita (EBA) exhibits similar antibodies against type VII collagen. It is more likely to heal with scarring and milia formation compared to BSLE. A prominent distinguishing feature includes the absence of SLE and a lack of histologic finding of large deposits of mucin in the dermis. The poor or slow response to dapsone in EBA compared to BSLE may help in separating the two entities.
Dermatitis herpetiformis (DH) has a skin distribution different from BSLE. The pruritic lesions have a predilection to the extensor surfaces, elbows, knees, and buttocks. DH is histologically identical to BSLE except for the presence of IgA deposition within the dermal papilla.[18]
Other differential diagnoses include:
- Linear IgA bullous dermatosis: immunofluorescence shows IgA deposition on the epidermal side of split skin
- Systemic lupus erythematosus with blisters
- Bullous pemphigoid: With the aid of immunofluorescence, antibody deposition is found on the epidermal side of salt-split skin
Prognosis
In a 12-year retrospective review, the majority of the patients healed without scarring or milia, although post-inflammatory hypo- or hyper-pigmentation may be seen. It was also pointed out that BSLE rarely recurred.[19]
Complications
Complications include:
- Infection of exposed and affected skin
- Sloughing esophagitis
- Complications from concomitant multiorgan SLE flare
- Medication side effects
Deterrence and Patient Education
Patient education is very vital in the management of bullous systemic lupus erythematosus. For a few, this may present as the first manifestation of SLE, which is a chronic, autoimmune condition with several multiorgan involvements. Educate these patients on the early signs and symptoms of organ involvement, photoprotection with sunscreen, and the need for medication adherence.
BSLE poses significant stress related to discomfort, aesthetics, and concern of skin complications. Support groups and behavioral therapy may be needed in such cases.
Enhancing Healthcare Team Outcomes
An interprofessional approach in evaluation, treatment, and care of patients with bullous systemic lupus erythematosus cannot be over-emphasized.
Primary care physicians, rheumatologists, and dermatologists play a key role in early diagnosis. The histopathology mimics of BSLE can be a source of a wrong diagnosis and delay of treatment, thus the need for an experienced pathologist.
Skincare by trained and dedicated nurses of the skin lesions, especially when ruptured leaving behind crusts and erosions, is also important.
Clinicians, nurses, and pharmacists also need to educate their patients on the disease condition, medications, and their potential side effects.
In cases with concomitant lupus nephritis, neuropsychiatric lupus, and hematologic complications, other subspecialties such as nephrology, neurology, and hematology may be needed.
Most importantly, the patient and family need to be involved in the treatment strategies, especially on decisions to escalate treatment to immunosuppressants. [Level 5]
Media
(Click Image to Enlarge)

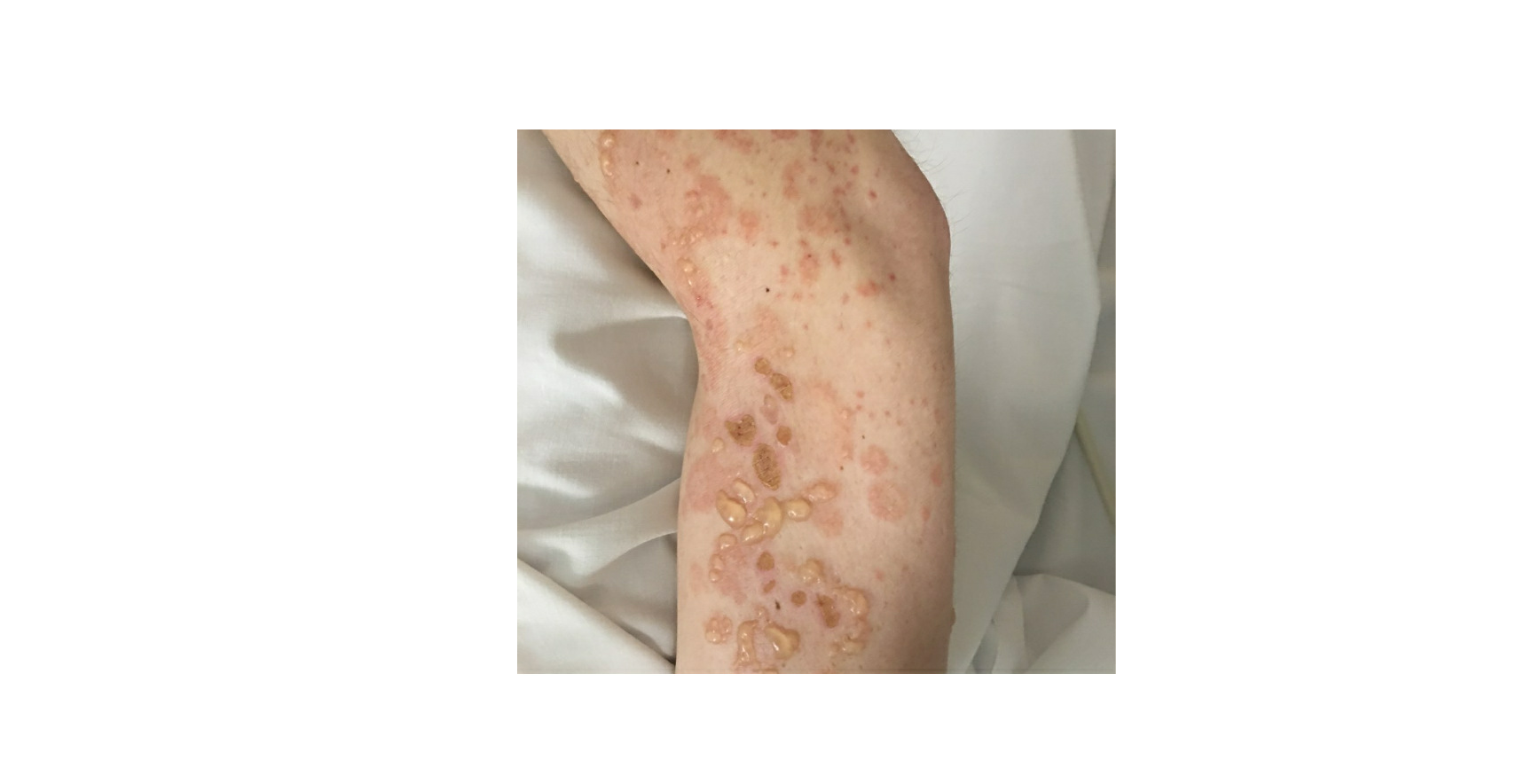
Bullous SLE
Contributed by Priyanka Vashisht MD
(Click Image to Enlarge)

Bullous SLE
Contributed by Priyanka Vashisht MD
(Click Image to Enlarge)
Bullous SLE
Contributed by Priyanka Vashisht MD
References
Rutnin S, Chanprapaph K. Vesiculobullous diseases in relation to lupus erythematosus. Clinical, cosmetic and investigational dermatology. 2019:12():653-667. doi: 10.2147/CCID.S220906. Epub 2019 Sep 4 [PubMed PMID: 31564947]
Contestable JJ, Edhegard KD, Meyerle JH. Bullous systemic lupus erythematosus: a review and update to diagnosis and treatment. American journal of clinical dermatology. 2014 Dec:15(6):517-24. doi: 10.1007/s40257-014-0098-0. Epub [PubMed PMID: 25358414]
Tincopa M, Puttgen KB, Sule S, Cohen BA, Gerstenblith MR. Bullous lupus: an unusual initial presentation of systemic lupus erythematosus in an adolescent girl. Pediatric dermatology. 2010 Jul-Aug:27(4):373-6. doi: 10.1111/j.1525-1470.2010.01179.x. Epub [PubMed PMID: 20653856]
Anyanwu CO, Ang CC, Werth VP. Oral mucosal involvement in bullous lupus. Arthritis and rheumatism. 2013 Oct:65(10):2622. doi: 10.1002/art.38051. Epub [PubMed PMID: 23780804]
Level 3 (low-level) evidenceBernard P, Vaillant L, Labeille B, Bedane C, Arbeille B, Denoeux JP, Lorette G, Bonnetblanc JM, Prost C. Incidence and distribution of subepidermal autoimmune bullous skin diseases in three French regions. Bullous Diseases French Study Group. Archives of dermatology. 1995 Jan:131(1):48-52 [PubMed PMID: 7826096]
Bain EE, Grover RK, Plunkett RW, Beutner EH. Detection of collagen VII autoantibodies to NC1 and NC2 domains of collagen VII by ELISA in suspected epidermolysis bullosa acquisita and bullous lupus erythematosus patients. Journal of dermatological science. 2012 Feb:65(2):155-6. doi: 10.1016/j.jdermsci.2011.12.004. Epub 2011 Dec 13 [PubMed PMID: 22225828]
Level 3 (low-level) evidenceChan LS, Lapiere JC, Chen M, Traczyk T, Mancini AJ, Paller AS, Woodley DT, Marinkovich MP. Bullous systemic lupus erythematosus with autoantibodies recognizing multiple skin basement membrane components, bullous pemphigoid antigen 1, laminin-5, laminin-6, and type VII collagen. Archives of dermatology. 1999 May:135(5):569-73 [PubMed PMID: 10328198]
Level 3 (low-level) evidencede Risi-Pugliese T, Cohen Aubart F, Haroche J, Moguelet P, Grootenboer-Mignot S, Mathian A, Ingen-Housz-Oro S, Hie M, Wendremaire N, Aucouturier F, Lepelletier F, Miyara M, Bader-Meunier B, Rémy P, Fabien N, Francès C, Barete S, Amoura Z. Clinical, histological, immunological presentations and outcomes of bullous systemic lupus erythematosus: 10 New cases and a literature review of 118 cases. Seminars in arthritis and rheumatism. 2018 Aug:48(1):83-89. doi: 10.1016/j.semarthrit.2017.11.003. Epub 2017 Nov 4 [PubMed PMID: 29191376]
Level 3 (low-level) evidenceVassileva S. Bullous systemic lupus erythematosus. Clinics in dermatology. 2004 Mar-Apr:22(2):129-38 [PubMed PMID: 15234014]
Gual A, Guilabert A, Iranzo P, Flores G, Diaz LA, Mascaró JM Jr. IgG autoantibody subclass analysis as a tool to differentiate epidermolysis bullosa acquisita with overlapping features of bullous systemic lupus erythematosus. Journal of the American Academy of Dermatology. 2013 Jul:69(1):e34-6. doi: 10.1016/j.jaad.2013.01.025. Epub [PubMed PMID: 23768307]
Level 3 (low-level) evidenceYell JA, Allen J, Wojnarowska F, Kirtschig G, Burge SM. Bullous systemic lupus erythematosus: revised criteria for diagnosis. The British journal of dermatology. 1995 Jun:132(6):921-8 [PubMed PMID: 7662571]
Fruchter R, Shaikh G, Myers KL, Eungdamrong NJ, Lee HS, Franks AG Jr. An erythema gyratum repens variant of bullous lupus erythematosus. JAAD case reports. 2016 Mar:2(2):111-3. doi: 10.1016/j.jdcr.2016.01.009. Epub 2016 Mar 3 [PubMed PMID: 27051846]
Level 3 (low-level) evidenceDa Silva Sousa AC, Campos M, Oliveira A, Menezes N, Tente D, Baptista A. Bullous lupus erythematosus with an erythema gyratum repens-like pattern. Dermatology online journal. 2019 Jan 15:25(1):. pii: 13030/qt0nt6h49v. Epub 2019 Jan 15 [PubMed PMID: 30710900]
Camisa C, Sharma HM. Vesiculobullous systemic lupus erythematosus. Report of two cases and a review of the literature. Journal of the American Academy of Dermatology. 1983 Dec:9(6):924-33 [PubMed PMID: 6358284]
Level 3 (low-level) evidenceCamisa C, Grimwood RE. Indirect immunofluorescence in vesiculobullous eruption of systemic lupus erythematosus. The Journal of investigative dermatology. 1986 May:86(5):606 [PubMed PMID: 3528314]
Level 3 (low-level) evidenceKomorowski L, Müller R, Vorobyev A, Probst C, Recke A, Jonkman MF, Hashimoto T, Kim SC, Groves R, Ludwig RJ, Zillikens D, Stöcker W, Schmidt E. Sensitive and specific assays for routine serological diagnosis of epidermolysis bullosa acquisita. Journal of the American Academy of Dermatology. 2013 Mar:68(3):e89-95. doi: 10.1016/j.jaad.2011.12.032. Epub 2012 Feb 16 [PubMed PMID: 22341608]
Duan L, Chen L, Zhong S, Wang Y, Huang Y, He Y, Chen J, Shi G. Treatment of Bullous Systemic Lupus Erythematosus. Journal of immunology research. 2015:2015():167064. doi: 10.1155/2015/167064. Epub 2015 May 18 [PubMed PMID: 26090480]
Ko CJ, Colegio OR, Moss JE, McNiff JM. Fibrillar IgA deposition in dermatitis herpetiformis--an underreported pattern with potential clinical significance. Journal of cutaneous pathology. 2010 Apr:37(4):475-7. doi: 10.1111/j.1600-0560.2009.01472.x. Epub 2009 Nov 16 [PubMed PMID: 19919655]
Level 3 (low-level) evidenceChanprapaph K, Sawatwarakul S, Vachiramon V. A 12-year retrospective review of bullous systemic lupus erythematosus in cutaneous and systemic lupus erythematosus patients. Lupus. 2017 Oct:26(12):1278-1284. doi: 10.1177/0961203317699714. Epub 2017 Mar 30 [PubMed PMID: 28358242]
Level 2 (mid-level) evidence