
Introduction
The left atrium (LA) is a crucial component of the cardiac physiology that partakes in collecting blood into the heart and modulates left ventricular filling during systole and diastole, respectively.[1] Left atrial enlargement (LAE) is the hallmark of the structural remodeling process, which occurs in response to chronic pressure and volume overload. LAE occurs most commonly in association with diastolic dysfunction, left ventricular hypertrophy, mitral valvular disease, and systemic hypertension.[2][3] The size of LA has prognostic implications, and studies reveal that LAE can independently predict the development of clinically significant several cardiovascular diseases and heart failure.[4][5] In the absence of mitral valvular disease, atrial fibrillation, and high cardiac output states its an excellent indicator of Left ventricular diastolic dysfunction. Therefore, the assessment of LAE is important and is achievable by various imaging techniques.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Both congenital and acquired conditions can lead to LAE. Some of the causes and conditions are as follows[4][6]:
- Left ventricular diastolic dysfunction
- Left to right shunt as in ventricular septal defect (VSD) and patent ductus arteriosus (PDA)
- Hypertension
- Aortic stenosis
- Mitral stenosis
- Mitral regurgitation
- Left ventricular failure
- Left atrial mass or myxoma
- Arteriovenous fistulas
- Athlete's heart
Epidemiology
The exact prevalence of left atrial enlargement is not available. Nonetheless, a study conducted by Bombelli et al. revealed that 12% of the participant over 10 years developed LAE.[7] The average age of the participants at the beginning of the study was 47 years old. LA size is affected by anthropomorphic variants such as age, gender, and body size. LAE is not a result of the normal aging process rather a consequence of pathophysiological changes associated with normal aging. Further, men have larger LA than women, and the size of left atria increases with an increase in body size.[4]
Pathophysiology
LAE is most commonly due to conditions caused by pressure overload, volume overload, or both. Mitral valve stenosis or left ventricular dysfunction with or without any valvular disease can increase left atrial afterload, which over time, causes LAE as compensation.[8][9] The left atrium connects to the left ventricular through the mitral valve. In a non-compliant left ventricle, left atrial pressure increases, followed by LAE to maintain LV filling pressure. Similarly, right to left shunts and arteriovenous fistulas and mitral regurgitation cause volume overload in the left atria, subsequently leading to LAE.[4] LAE is an early finding in hypertensive heart disease.[10] LAE is a strong predictor of atrial fibrillation.[11][12]
History and Physical
There are no signs and symptoms of LAE in itself, and it is a pathophysiological response to other underlying cardiovascular conditions. Therefore, the focus should be on recognizing signs and symptoms related to the underlying pathological causes of LAE. Patients with LAE might present with a variety of symptoms, including palpitations, dyspnea, syncope, peripheral edema, fatigue, and weight gain.
Similarly, some patients in early phases of underlying cardiac disease such as left ventricular hypertrophy and a mild form of mitral valve diseases, stenosis or regurgitation, and undiagnosed systemic hypertension may present with absolutely no symptom, and the initial presentation could be an abnormal electrocardiogram or echocardiogram examined for any other reason. It is necessary for proper evaluation of the history of present illness in these patients, including the past medical history, social and family history that includes the risk factors for left ventricular hypertrophy, valvular abnormalities, congenital heart diseases, arrhythmias, and hypertension.
Evaluation
Atrial size and function are assessable using various modalities, including echocardiography, cardiac computed tomography (CCT), and cardiac magnetic resonance (CMR). However, an echocardiogram is a more common choice due to easy availability and safety.[13][14]. Echocardiographic assessment of left atrial volume correlates well with CT and MRI.[15]
Echocardiogram: LA size is measurable by multiple methods using two-dimensional and M-mode echocardiography.[16][17][13] Linear measurement of the left atria, however, might not truly represent the left atrial size, especially in asymmetrical enlargement of the LA. Hence, there has been a paradigm shift in the LA assessment. LA volume is the current standard of echocardiographic assessment of LA remodeling. LV volume is approximated using either the biplane area-length method or Simpson’s biplane method as per the recommendation of the American Society of Echocardiography and the European Association of Echocardiography. LA volume is affected by the body habitus, and hence it should be indexed to body surface area (LAVi).[18][19] A normal LAVi using an echocardiogram is 22 plus or minus 6 ml/m, and the American Society of Echocardiography considers the cut-off for LA enlargement as greater than 28 ml/m (mild greater than or equal to 28; moderate greater than or equal to 34; severe greater than or equal to 40). Newer three-dimensional echocardiography is increasingly an option to assess LA volume and enlargement.[20]
Electrocardiogram (EKG): The presence of any one of the following EKG findings would warrant a further investigation for LAE in the appropriate clinical context.[21][22][23][24]
- P wave in any lead greater than 0.11 s
- Notched P wave with an interpeak duration exceeding 0.04 s; P mitral
- P wave axis less than 30 degrees
Treatment / Management
There is no guidelines-based treatment available for LAE. Currently, no known medical therapy is available to reverse the left atrial remodeling. The focus of care and medical treatment in patients with LAE is the identification and treatment of underlying pathologies.
Treating valvular abnormalities: Mitral valve stenosis/regurgitation involves medical therapy geared towards relieving symptoms, percutaneous mitral valvuloplasty, and surgical treatment. Patients might also need anticoagulation therapy should they develop arrhythmias to lower thromboembolic risks.
Treating hypertension: It is the most common modifiable risk factor for cardiovascular diseases. Many blood pressures lowering agents are available to aid patients in lowering blood pressure. Similarly, lifestyle modification, including consuming low salt diet, exercising regularly, limiting alcohol intake, quitting smoking are some of the measures that assist in lowering blood pressure.
Treating left ventricular dysfunction and heart failure: Medical therapy remains the cornerstone of these pathologies. The mainstay of medical treatment includes beta-blockers (BB) including carvedilol, metoprolol succinate, and bisoprolol, angiotensin-converting enzyme inhibitors (ACEi)/angiotensin receptor blockers (ARB), and mineralocorticoid receptor antagonists (MRA). A new class of medication angiotensin receptor neprilysin inhibitor sacubitril/valsartan is also being recognized recently for offering mortality benefits in patients with heart failure with reduced ejection fraction.[25][26] (B3)
Differential Diagnosis
Mitral stenosis
Prognosis
LAE is not a benign condition. LA diameter, in the absence of LVH, acts as a prognosticator of fatal and nonfatal cardiovascular events independently of other contributors to cardiovascular risk such as hypertension.[27] Left atrial size is independently associated with all-cause mortality in both sexes and with ischemic stroke in women.[28] Underlying pathology leading to LAE should be explored and managed accordingly to avoid any catastrophic outcome and prevent poor quality of life.
Complications
Most commonly encountered complications include[27][4]:
- Atrial fibrillation
- Stroke
- Heart failure with preserved ejection fraction (HFpEF)
Deterrence and Patient Education
It is likely that patients with left atrial enlargement may not experience any symptoms throughout their lifetime. Nonetheless, the presence of LAE might be a sign of underlying cardiac pathology and requires further exploration. Since treatment of the disease itself is not available, patients with left atrial enlargement must be made aware of the other underlying cardiac pathologies and guided accordingly in terms of management, which ranges from simple lifestyle modifications to surgical evaluation and treatment.
Pearls and Other Issues
One of the major pitfalls in LA assessment is inaccurate echocardiographic measurements. More than one echocardiographic plane (especially two orthogonal planes) are necessary for assessing LAVi. The foreshortening of the long axis of LA should be avoided.
Enhancing Healthcare Team Outcomes
There are guidelines available for the diagnosis of LAE, but no therapeutic management geared towards its management. Hence, the most critical feature in terms of management of the condition is the treatment of any underlying cardiac pathology and patient education to avoid fatal consequences. Since LAE is a prognosticator of cardiovascular events, both fatal and non-fatal, management of the condition is best with an interprofessional health care team approach, including doctors, nurses, pharmacists, physiotherapists, dietitians, physical trainers, and psychologists.
Following an established diagnosis of LAE is established, the patient should receive education about the disease and the need for further evaluation of other coexisting cardiac pathologies. Asymptomatic patients should continue to get annual exams, including echocardiograms. Patients with underlying hypertension need strict blood pressure control. Patients with underlying heart failure require medical management and lifestyle modification, as well. A dietary consult can help patients to adjust to low salt diet and healthy eating habits. A patient with LAE and palpitation must undergo an EKG and a Holter monitor to evaluate any underlying arrhythmia that can develop as a consequence of LAE. Many patients might require anticoagulation therapy to avoid any thromboembolic event. Pharmacists can help ensure patients get all their medications in a timely fashion. They can also recommend medication selection, dosing, and reconciliation to avoid any drug interactions. Pharmacists can also help report any adverse drug reaction to the health care team and assist in subsequent medication changes as well as patient counseling. Nurses, especially cardiovascular trained, are a vital part of the patient team care. Nurses are an extension of the treating physician in an appropriate clinical setting. They can help administer medications while the patient remains in the hospital. Their role is also vital in monitoring patient compliance, providing counseling, and answering questions from the patient and the family members. A fully collaborative, interprofessional team approach can help achieve optimal results in patients with LAE. [Level 5]
Media
(Click Image to Enlarge)
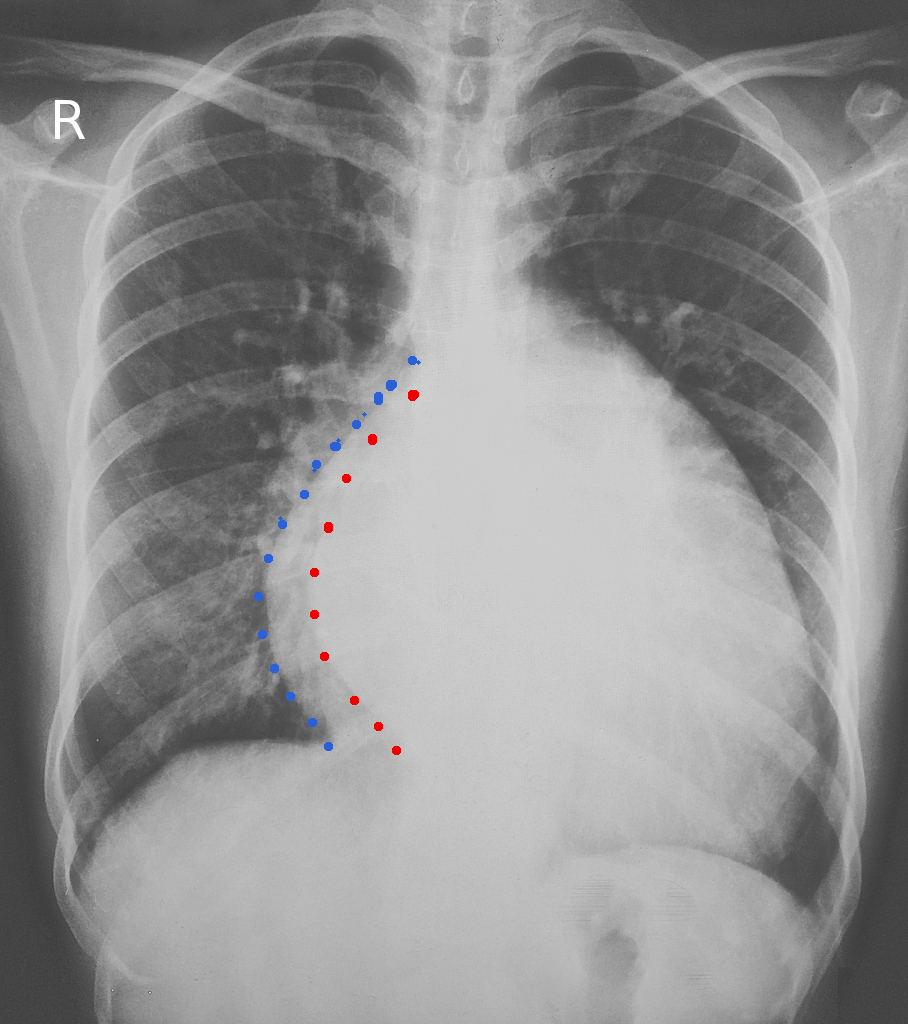
left atrial enlargement
Image courtesy S Bhimji MD
(Click Image to Enlarge)
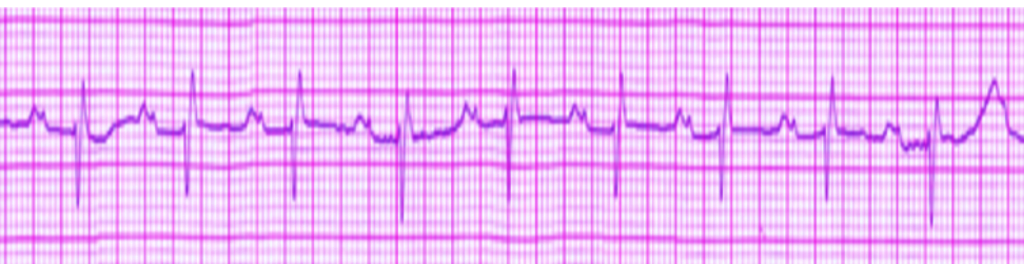
ECG left atrial enlargement
Image courtesy S Bhimji MD
References
Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, Tajik AJ, Tsang TS. Left atrial size: physiologic determinants and clinical applications. Journal of the American College of Cardiology. 2006 Jun 20:47(12):2357-63 [PubMed PMID: 16781359]
Cuspidi C, Negri F, Sala C, Valerio C, Mancia G. Association of left atrial enlargement with left ventricular hypertrophy and diastolic dysfunction: a tissue Doppler study in echocardiographic practice. Blood pressure. 2012 Feb:21(1):24-30. doi: 10.3109/08037051.2011.618262. Epub 2011 Oct 13 [PubMed PMID: 21992028]
Cuspidi C, Rescaldani M, Sala C. Prevalence of echocardiographic left-atrial enlargement in hypertension: a systematic review of recent clinical studies. American journal of hypertension. 2013 Apr:26(4):456-64. doi: 10.1093/ajh/hpt001. Epub 2013 Feb 6 [PubMed PMID: 23388831]
Level 1 (high-level) evidencePatel DA, Lavie CJ, Milani RV, Shah S, Gilliland Y. Clinical implications of left atrial enlargement: a review. The Ochsner journal. 2009 Winter:9(4):191-6 [PubMed PMID: 21603443]
Kizer JR, Bella JN, Palmieri V, Liu JE, Best LG, Lee ET, Roman MJ, Devereux RB. Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: the Strong Heart Study (SHS). American heart journal. 2006 Feb:151(2):412-8 [PubMed PMID: 16442908]
Level 2 (mid-level) evidenceRusinaru D, Bohbot Y, Kowalski C, Ringle A, Maréchaux S, Tribouilloy C. Left Atrial Volume and Mortality in Patients With Aortic Stenosis. Journal of the American Heart Association. 2017 Oct 31:6(11):. doi: 10.1161/JAHA.117.006615. Epub 2017 Oct 31 [PubMed PMID: 29089338]
Bombelli M, Cuspidi C, Facchetti R, Sala C, Tadic M, Brambilla G, Re A, Villa P, Grassi G, Mancia G. New-onset left atrial enlargement in a general population. Journal of hypertension. 2016 Sep:34(9):1838-45. doi: 10.1097/HJH.0000000000001022. Epub [PubMed PMID: 27379539]
Pape LA, Price JM, Alpert JS, Ockene IS, Weiner BH. Relation of left atrial size to pulmonary capillary wedge pressure in severe mitral regurgitation. Cardiology. 1991:78(4):297-303 [PubMed PMID: 1889048]
Appleton CP, Galloway JM, Gonzalez MS, Gaballa M, Basnight MA. Estimation of left ventricular filling pressures using two-dimensional and Doppler echocardiography in adult patients with cardiac disease. Additional value of analyzing left atrial size, left atrial ejection fraction and the difference in duration of pulmonary venous and mitral flow velocity at atrial contraction. Journal of the American College of Cardiology. 1993 Dec:22(7):1972-82 [PubMed PMID: 8245357]
Aljizeeri A, Gin K, Barnes ME, Lee PK, Nair P, Jue J, Tsang TS. Atrial remodeling in newly diagnosed drug-naive hypertensive subjects. Echocardiography (Mount Kisco, N.Y.). 2013 Jul:30(6):627-33. doi: 10.1111/echo.12119. Epub 2013 Jan 30 [PubMed PMID: 23360480]
Level 2 (mid-level) evidenceVaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation. 1994 Feb:89(2):724-30 [PubMed PMID: 8313561]
Tsang TS, Barnes ME, Bailey KR, Leibson CL, Montgomery SC, Takemoto Y, Diamond PM, Marra MA, Gersh BJ, Wiebers DO, Petty GW, Seward JB. Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women. Mayo Clinic proceedings. 2001 May:76(5):467-75 [PubMed PMID: 11357793]
Level 2 (mid-level) evidenceHoit BD. Left atrial size and function: role in prognosis. Journal of the American College of Cardiology. 2014 Feb 18:63(6):493-505. doi: 10.1016/j.jacc.2013.10.055. Epub 2013 Nov 27 [PubMed PMID: 24291276]
To AC, Flamm SD, Marwick TH, Klein AL. Clinical utility of multimodality LA imaging: assessment of size, function, and structure. JACC. Cardiovascular imaging. 2011 Jul:4(7):788-98. doi: 10.1016/j.jcmg.2011.02.018. Epub [PubMed PMID: 21757171]
Kircher B, Abbott JA, Pau S, Gould RG, Himelman RB, Higgins CB, Lipton MJ, Schiller NB. Left atrial volume determination by biplane two-dimensional echocardiography: validation by cine computed tomography. American heart journal. 1991 Mar:121(3 Pt 1):864-71 [PubMed PMID: 2000754]
Level 1 (high-level) evidenceHirata T, Wolfe SB, Popp RL, Helmen CH, Feigenbaum H. Estimation of left atrial size using ultrasound. American heart journal. 1969 Jul:78(1):43-52 [PubMed PMID: 5794795]
Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978 Dec:58(6):1072-83 [PubMed PMID: 709763]
Level 3 (low-level) evidenceVasan RS, Larson MG, Levy D, Evans JC, Benjamin EJ. Distribution and categorization of echocardiographic measurements in relation to reference limits: the Framingham Heart Study: formulation of a height- and sex-specific classification and its prospective validation. Circulation. 1997 Sep 16:96(6):1863-73 [PubMed PMID: 9323074]
Level 1 (high-level) evidenceTsang TS, Abhayaratna WP, Barnes ME, Miyasaka Y, Gersh BJ, Bailey KR, Cha SS, Seward JB. Prediction of cardiovascular outcomes with left atrial size: is volume superior to area or diameter? Journal of the American College of Cardiology. 2006 Mar 7:47(5):1018-23 [PubMed PMID: 16516087]
Takeuchi M, Kitano T, Nabeshima Y, Otsuji Y, Otani K. Left ventricular and left atrial volume ratio assessed by three-dimensional echocardiography: Novel indices for evaluating age-related change in left heart chamber size. Physiological reports. 2019 Dec:7(23):e14300. doi: 10.14814/phy2.14300. Epub [PubMed PMID: 31814325]
Hazen MS, Marwick TH, Underwood DA. Diagnostic accuracy of the resting electrocardiogram in detection and estimation of left atrial enlargement: an echocardiographic correlation in 551 patients. American heart journal. 1991 Sep:122(3 Pt 1):823-8 [PubMed PMID: 1831587]
Munuswamy K, Alpert MA, Martin RH, Whiting RB, Mechlin NJ. Sensitivity and specificity of commonly used electrocardiographic criteria for left atrial enlargement determined by M-mode echocardiography. The American journal of cardiology. 1984 Mar 1:53(6):829-32 [PubMed PMID: 6230922]
Waggoner AD, Adyanthaya AV, Quinones MA, Alexander JK. Left atrial enlargement. Echocardiographic assessment of electrocardiographic criteria. Circulation. 1976 Oct:54(4):553-7 [PubMed PMID: 134852]
Ikram H, Drysdale P, Bones PJ, Chan W. The non-invasive recognition of left atrial enlargement: comparison of electro- and echocardiographic measurements. Postgraduate medical journal. 1977 Jul:53(621):356-9 [PubMed PMID: 142246]
Almufleh A, Marbach J, Chih S, Stadnick E, Davies R, Liu P, Mielniczuk L. Ejection fraction improvement and reverse remodeling achieved with Sacubitril/Valsartan in heart failure with reduced ejection fraction patients. American journal of cardiovascular disease. 2017:7(6):108-113 [PubMed PMID: 29348971]
Oparil S, Schmieder RE. New approaches in the treatment of hypertension. Circulation research. 2015 Mar 13:116(6):1074-95. doi: 10.1161/CIRCRESAHA.116.303603. Epub [PubMed PMID: 25767291]
Level 3 (low-level) evidenceBombelli M, Facchetti R, Cuspidi C, Villa P, Dozio D, Brambilla G, Grassi G, Mancia G. Prognostic significance of left atrial enlargement in a general population: results of the PAMELA study. Hypertension (Dallas, Tex. : 1979). 2014 Dec:64(6):1205-11. doi: 10.1161/HYPERTENSIONAHA.114.03975. Epub 2014 Sep 8 [PubMed PMID: 25201892]
Level 2 (mid-level) evidenceBouzas-Mosquera A, Broullón FJ, Álvarez-García N, Méndez E, Peteiro J, Gándara-Sambade T, Prada O, Mosquera VX, Castro-Beiras A. Left atrial size and risk for all-cause mortality and ischemic stroke. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2011 Jul 12:183(10):E657-64. doi: 10.1503/cmaj.091688. Epub 2011 May 24 [PubMed PMID: 21609990]