
Introduction
Abdominal aortic aneurysm (AAA) repair is performed because the mortality rates are as high as 78% following rupture. Open and endovascular surgery are the two approaches utilized for AAA repair. Open repair is accomplished by either accessing the aorta through a transabdominal or retroperitoneal approach. The aorta is then cross-clamped, the aneurysm sac is next opened and graft in, then sewn within the aorta to exclude the aneurysmal portion. Finally, the aneurysm sac is closed over the graft. In contrast, an endovascular aortic repair is typically performed by accessing the femoral artery through either cut-down or percutaneous means. The endograft is then delivered over a wire in a retrograde fashion to the affected aortic segment and deployed with the use of fluoroscopic imaging. Main repair indications include a large aneurysm diameter (5 cm in females, 5.5 cm in males), rapid expansion, symptomatic aneurysm, and frank rupture.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Smoking duration is the strongest risk factor in AAA development. Elevated risk of development also is seen with increasing age (males older than 50, females older than 60), male sex, white race and a positive family history. Additional associations are found with vasculitides, infectious aortitis, a low-density lipoprotein receptor-related protein 1 (LRP1) variant, and rarely, Marfan syndrome. Factors specifically linked with high rupture risk include AAA greater than 6 cm, female gender, current smoking, uncontrolled hypertension, severe chronic obstructive pulmonary disease, AAA growth greater than 0.5 cm per year, and multiple family members with AAA.[4][5]
Epidemiology
Since the early 2000s, AAA prevalence, rupture rates, and mortality have declined when compared to data from the 1990s. Prevalence was previously reported to be between 4% to 9% in men whereas more recent studies report prevalence below 2%. Large reductions in smoking, which is associated with 75% of AAA; established screening guidelines, leading to approximately 40% mortality reduction; and an increased number of elective endovascular aneurysm repairs have contributed to this trend.[6][7]
Pathophysiology
AAA by definition is a concurrent dilatation of all three vessel wall layers: tunica intima, media, and adventitia, which result in a transaortic cross-sectional diameter of at least 3 cm. Although cigarette smoking provides the strongest link to AAA development, the exact mechanism by which it does so is not explicitly defined. The response of endothelial cells, vascular smooth muscle cells, and macrophages to cigarette smoke as well as genomic studies demonstrating a genetic predisposition to AAA development are active areas of investigation.
Histopathology
Resected segments of the aneurysmal aorta usually reveal varying degrees of neovascularity and a chronic inflammatory infiltrate. There is evidence of degeneration of the aortic walls.
History and Physical
Abdominal palpation and examination of the femoral and popliteal pulses are recommended for AAA evaluation although up to 25% of AAAs larger than 5 cm are missed with focused physicals. Patients may report an exaggerated pulse or pulsating mass in the abdomen. Additional presentations include signs of embolic phenomena, originating from the aneurysm wall thrombus such as in blue toe syndrome, as well as signs of deep venous thrombosis from iliocaval compression by an aneurysm. Rare symptoms include chronic back pain from vertebral involvement, early satiety and nausea from gastric outlet obstruction, and urinary retention from ureter obstruction. Frank rupture elicits the classic triad of severe back or abdominal pain, hypotension and pulsatile abdominal mass in 50% of cases.
Evaluation
For screening, a one-time abdominal ultrasound is recommended for anyone 65 or older who have smoked or have a family history of AAAs. Screening for males with a positive family history can begin as early as 55 years old. Yearly ultrasound surveillance is recommended for AAAs between 3.5 cm to 4.4 cm and repeat ultrasound is recommended every 6 months for AAAs between 4.5 cm to 5.4 cm. A high-quality CT angiography with computerized reconstruction is recommended for patients requiring aneurysm repair.[8][9][10]
Treatment / Management
Endovascular and open surgery are currently the only two evidence-based treatment options for AAA repair. Endovascular aneurysm repair (EVAR) is the preferred approach for elective or emergent repair but requires favorable patient anatomy including a 1.0 cm to 1.5 cm aneurysm neck, a neck diameter less than 3.2 cm, aortic angulation less than 60 degrees, and access vessels amenable to endograft delivery. Open surgical repair (OSR) is typically reserved for the emergent repair of ruptured AAAs, aneurysms within 1 cm of or involving the renal arteries, and for patients with anatomy unfavorable to endovascular repair. Fenestrated and branched grafts are alternative endovascular approaches for aneurysms with renal artery involvement.[11][12][8](A1)
Differential Diagnosis
- Acute gastritis
- Acute myocardial infarction
- Acute urinary tract infection
- Appendicitis
- Cholelithiasis
- Cystitis
- Diverticulitis
- Gastrointestinal bleed
- Ischemic bowel
- Large bowel obstruction
- Nephrolithiasis
- Musculoskeletal pain
- Pancreatitis
- Peptic ulcer disease
- Perforated gastrointestinal ulcer
- Pyelonephritis
- Small bowel obstruction
Prognosis
For elective AAA repair, the mortality is very low. However, for those who present with a rupture, the mortality can exceed 50%. Even those who survive surgery develop wound problems, bowel ischemia, heart failure, leg necrosis and multiorgan failure.
Complications
- Renal Failure
- Stroke
- Heart attack
- Leg ischemia
- Bleeding
- Prosthetic graft infection
- Injury to the ureters
- Erectile dysfunction
- Bowel ischemia
- Deep vein thrombosis
Consultations
Once a diagnosis of an abdominal aneurysm is made, the vascular surgeon should be consulted.
Deterrence and Patient Education
- Avoid smoking
- Eat healthy
- Exercise
Pearls and Other Issues
Endoleaks are a complication in approximately 25% of EVARs that must be monitored with either postoperative triple-phase CTA scans or color duplex ultrasound. This surveillance is required as endoleaks allow blood to fill the aneurysm sac around the endograft and may contribute to the continued risk of sac rupture. Type II endoleaks are the most common and occur when aortic side branches such as lumbar, inferior mesenteric, or middle sacral arteries provide retrograde filling to the lower pressure aneurysm sac. These are often thought to be benign but are treated most commonly with translumbar or transarterial embolization when intervention is deemed necessary. Other endoleaks include Type I, sac filling around graft ends; Type III, sac filling at misaligned graft components; Type IV, sac filling through porous graft material; and Type V, sac filling through endotension).[1][13][14]
Another devastating but rare complication following EVAR is graft infection. Its incidence has been reported to be between 0.2% to 5% of endovascular aortic repairs with an increased occurrence after emergent repairs and in patients with infection complicating the index operation. Patients often present with nonspecific symptoms which can delay diagnoses such as back pain, abdominal pain, fever or chills. Additional findings include aortic fistula, endoleak, or aneurysm rupture. Endograft infections are often polymicrobial or caused by gram-positive organisms. Surgical management is the mainstay of endograft infection with graft excision, tissue debridement, and aortic conduit reconstruction being the overarching approach. This was traditionally accomplished with graft excision, over-sewing the aorta and performing an extraanatomical bypass to ensure distal perfusion. In-line reconstructions with venous conduits, cryo allografts, or antibiotic-impregnated prosthetic grafts are more widely utilized approaches. As persistent sepsis or recurrent infection remains a possibility following these procedures, patients should be placed on long-term antibiotic therapy.
Enhancing Healthcare Team Outcomes
Abdominal aortic aneurysms that have not ruptured are often identified incidentally on imaging studies or a physical exam. It is important for all healthcare workers to refer these patients to a vascular surgeon because not all may require treatment. Healthcare workers in the emergency room including nurse practitioners should be aware that endovascular options are now being offered to patients with an AAA. However, even after the endovascular procedure is completed, the patient needs long-term follow up since leaks are not uncommon. Overall, endovascular repair has much lower morbidity than open surgery and should be the initial recommendation for all elective AAA.[15][16]
Media
(Click Image to Enlarge)
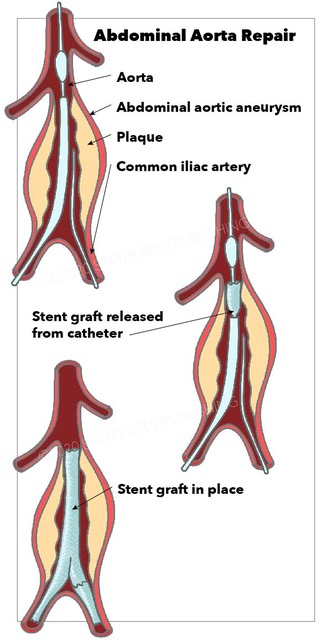
Abdominal Aorta Repair, aneurysm, common iliac artery, stent graft released from catheter
StatPearls Publishing Illustration
References
Qazi AA, Jaberi A, Mironov O, Addas J, Qazi E, Tarulli E, Simons M, Tan KT. Conservative management of type 1A endoleaks at completion angiogram in endovascular repair of infra-renal abdominal aortic aneurysms with current generation stent grafts. Vascular. 2019 Apr:27(2):168-174. doi: 10.1177/1708538118811206. Epub 2018 Nov 5 [PubMed PMID: 30396328]
Oikonomou K, Kasprzak P, Schierling W, Kopp R, Pfister K. [Indications for the Use of Endoanchors: State of the Art]. Zentralblatt fur Chirurgie. 2018 Oct:143(5):503-509. doi: 10.1055/a-0746-3679. Epub 2018 Oct 24 [PubMed PMID: 30357794]
Sakalihasan N, Michel JB, Katsargyris A, Kuivaniemi H, Defraigne JO, Nchimi A, Powell JT, Yoshimura K, Hultgren R. Abdominal aortic aneurysms. Nature reviews. Disease primers. 2018 Oct 18:4(1):34. doi: 10.1038/s41572-018-0030-7. Epub 2018 Oct 18 [PubMed PMID: 30337540]
Desole A, Ferrari A, Tosato F, Milite D. Open Repair for Juxtarenal Aortic Aneurysm: Short and Long-term Results. Annals of vascular surgery. 2019 Jan:54():161-165. doi: 10.1016/j.avsg.2018.05.071. Epub 2018 Aug 6 [PubMed PMID: 30092431]
Carino D, Sarac TP, Ziganshin BA, Elefteriades JA. Abdominal Aortic Aneurysm: Evolving Controversies and Uncertainties. The International journal of angiology : official publication of the International College of Angiology, Inc. 2018 Jun:27(2):58-80. doi: 10.1055/s-0038-1657771. Epub 2018 May 29 [PubMed PMID: 29896039]
Wallinder J, Georgiou A, Wanhainen A, Björck M. Prevalence of Synchronous and Metachronous Aneurysms in Women With Abdominal Aortic Aneurysm. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2018 Sep:56(3):435-440. doi: 10.1016/j.ejvs.2018.05.015. Epub 2018 Jun 20 [PubMed PMID: 29935861]
Niclot J, Stansal A, Saint-Lary O, Lazareth I, Priollet P. [Identifying barriers to screening for abdominal aortic aneurysm in general practice: Qualitative study of 14 general practitioners in Paris]. Journal de medecine vasculaire. 2018 May:43(3):174-181. doi: 10.1016/j.jdmv.2018.03.002. Epub 2018 Apr 25 [PubMed PMID: 29754727]
Level 2 (mid-level) evidenceParaskevas KI, Gloviczki P. Some asymptomatic abdominal aortic aneurysms smaller than 5.5 cm can be considered for elective repair. Journal of vascular surgery. 2018 Jun:67(6):1645-1648. doi: 10.1016/j.jvs.2018.01.042. Epub [PubMed PMID: 29685510]
Huang Y, Gloviczki P, Duncan AA, Kalra M, Oderich GS, Fleming MD, Harmsen WS, Bower TC. Maximal aortic diameter affects outcome after endovascular repair of abdominal aortic aneurysms. Journal of vascular surgery. 2017 May:65(5):1313-1322.e4. doi: 10.1016/j.jvs.2016.10.093. Epub 2016 Dec 27 [PubMed PMID: 28034585]
Laroche JP, Becker F, Baud JM, Miserey G, Jaussent A, Picot MC, Bura-Rivière A, Quéré I. [Ultrasound screening of abdominal aortic aneurysm: Lessons from Vesale 2013]. Journal des maladies vasculaires. 2015 Dec:40(6):340-9. doi: 10.1016/j.jmv.2015.07.104. Epub 2015 Sep 12 [PubMed PMID: 26371387]
Sidloff DA, Stather PW, Choke E, Bown MJ, Sayers RD. A systematic review and meta-analysis of the association between markers of hemostasis and abdominal aortic aneurysm presence and size. Journal of vascular surgery. 2014 Feb:59(2):528-535.e4. doi: 10.1016/j.jvs.2013.10.088. Epub [PubMed PMID: 24461868]
Level 1 (high-level) evidenceDesjardins B, Dill KE, Flamm SD, Francois CJ, Gerhard-Herman MD, Kalva SP, Mansour MA, Mohler ER 3rd, Oliva IB, Schenker MP, Weiss C, Rybicki FJ, American College of Radiology. ACR Appropriateness Criteria® pulsatile abdominal mass, suspected abdominal aortic aneurysm. The international journal of cardiovascular imaging. 2013 Jan:29(1):177-83. doi: 10.1007/s10554-012-0044-2. Epub 2012 May 27 [PubMed PMID: 22644671]
Kuziez MS, Picus D, Sanchez LA, Zayed MA. Trans-luminal repair of a ruptured AAA with Type Ia and Type II endoleaks. Journal of surgical case reports. 2018 Oct:2018(10):rjy254. doi: 10.1093/jscr/rjy254. Epub 2018 Oct 8 [PubMed PMID: 30310643]
Level 3 (low-level) evidenceRibner AS, Tassiopoulos AK. Postoperative Aortic Neck Dilation: Myth or Fact? The International journal of angiology : official publication of the International College of Angiology, Inc. 2018 Jun:27(2):110-113. doi: 10.1055/s-0038-1649516. Epub 2018 May 23 [PubMed PMID: 29896043]
Wang T, Zhao J, Yuan D, Ma Y, Huang B, Yang Y, Zeng G. Comparative effectiveness of open surgery versus endovascular repair for hemodynamically stable and unstable ruptured abdominal aortic aneurysm. Medicine. 2018 Jul:97(27):e11313. doi: 10.1097/MD.0000000000011313. Epub [PubMed PMID: 29979402]
Level 2 (mid-level) evidenceHallett RL, Ullery BW, Fleischmann D. Abdominal aortic aneurysms: pre- and post-procedural imaging. Abdominal radiology (New York). 2018 May:43(5):1044-1066. doi: 10.1007/s00261-018-1520-5. Epub [PubMed PMID: 29460048]