
Introduction
Esophageal cysts are rare congenital malformations first described by Blasius in 1711.[1] In 1881, Roth also described these cysts, which divide into two categories: simple epithelial-lined cysts or foregut cysts, which include duplication cysts. Esophageal duplication cysts have a double layer of surrounding smooth muscle, which are lined by squamous or enteric epithelium, and are either attached to the esophagus or located within the wall.[2][3][4][5] They are usually diagnosed in childhood but can also present in adults. Patients can be asymptomatic or present with symptoms of respiratory distress, dysphagia, and/or chest pain. Esophageal cysts are usually incidental findings on endoscopy or imaging studies such as computed tomography (CT), magnetic resonance imaging (MRI), or barium esophagogram. The most common treatment is thoracotomy with cyst excision, but less invasive techniques, including endoscopic, laparoscopic, or thoracoscopic approaches, are gaining popularity.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of esophageal cysts is not clearly understood. The development of esophageal cysts is believed to result from a failure of vacuolization and budding of the primitive esophagus between weeks 4 to 8 of gestation, although no single unifying hypothesis has been able to elucidate why cysts occur at varying locations throughout the gastrointestinal tract.[6][7] They are most common on the right lateral aspect of the esophagus due to the embryologic pattern of rotation and lengthening of the intrathoracic viscera during development.[7]
Epidemiology
Esophageal cysts are rare entities, as their incidence is reported to be 1 in 8200 live births with a 2 to 1 male predominance.[8] They account for approximately 10 percent of all mediastinal tumors in children, and an estimated 10 to 15 percent of all duplications cysts that occur in the alimentary tract stem from the esophagus.[9][10][11] As many as 80 percent of these cysts are diagnosed in childhood.[12]
Pathophysiology
As a result of the aberrant development of the posterior division of the primitive foregut during embryogenesis, esophageal cysts can occur anywhere along the esophagus. Approximately 60 percent of the cysts occur in the lower third of the esophagus, which results in compressive dysphagia being the most common presenting symptom. Posterior cysts, located in the lower third of the esophagus, have also been seen to cause cardiac arrhythmias.[13] The remaining cysts occur in the upper/middle third of the esophagus, where retrosternal chest pain and upper respiratory symptoms such as cough, stridor and wheezing, predominate.[12][14]
Approximately 90 percent of esophageal cysts do not communicate with the esophageal lumen; the others tend to run parallel to and communicate with the esophageal lumen.[9]
Histopathology
Duplication cysts may be cystic, tubular, or present as a diverticulum with the cystic type being more common.[15] The lining of the cysts can vary and can encompass stratified squamous, simple columnar, cuboidal, pseudostratified, and ciliated histology. There are reports of heterotopic tissue, including gastric and pancreatic mucosae along with mucosae resembling Peyer’s patches.[16]
History and Physical
Most esophageal cysts are diagnosed in early childhood but can also present in adults. Some esophageal duplication cysts may have correlations with concurrent vertebral abnormalities.[17] Symptoms stem from extrinsic compression or displacement of surrounding mediastinal structures. Symptoms reported include respiratory distress, vomiting, dysphagia, chest pain, and failure to thrive.[18][19] Hematemesis may also occur if there is ectopic gastric epithelium present.[20] Reports exist of neurological deficits, such as nerve root compression along with cervical motion res.[21] Malignancy can develop, albeit rarely.[22]
The differentials for esophageal duplication cysts include mediastinal cysts like bronchogenic cysts, pericardial cysts or cystic degeneration of mediastinal tumors or other cysts including hydatid cyst, Mullerian cysts.[23]
Evaluation
The workup and evaluation of esophageal cysts include imaging/diagnostic procedures guided by history and physical examination findings and specific histopathologic characteristics. Imaging studies such as chest radiographs and barium swallow studies can reveal a mediastinal mass with esophageal compression along with tracheal displacement and narrowing.[11]
Computed tomography (CT) of an esophageal cyst can reveal a fluid-filled cystic structure arising from the esophagus that does not enhance after intravenous administration of contrast material. A benefit of CT includes the ability to rule out a lung and thoracic vertebral pathology along with providing anatomical landmarks if pursuing surgical intervention.[24] Magnetic resonance imaging (MRI) can also show further anatomic detail. Routine endoscopy typically shows extrinsic compression of the esophageal lumen by the cyst with normal-appearing esophageal mucosa.
Endoscopic ultrasound (EUS) is the modality of choice to evaluate esophageal cysts. EUS can further characterize the echogenicity of the lesion.[12] It is a good tool to distinguish them from bronchogenic cysts by the absence of cartilage, proximity to the esophagus, and double muscle layer around them.[18][25] EUS also provides an opportunity to do an FNA of these lesions for confirming the nature of contents. Typically, EUS will reveal an anechoic homogenous lesion with smooth margins in the submucosal wall. The muscularis propria of the cyst is continuous with the muscularis of the esophagus. Some cysts may be hypoechoic or with heteroechoic lesions with an anechoic component due to the presence of pus, blood or thick contents may modify the EUS features and result in confusion with other soft-tissue lesions like stromal tumors.[26][27] EUS guided fine needle aspiration (FNA) has been used to confirm the diagnosis in patients with mediastinal cysts, but EUS FNA of duplication cysts may lead to infection despite using prophylactic antibiotics.[26] Hence, caution is needed when planning for EUS with FNA of an esophageal cyst.
The criteria for classifying an esophageal cyst include the following [4][10]:
- The cyst is within or attached to the esophageal wall.
- Two muscle layers cover the cyst.
- The lining is squamous, columnar, cuboidal, pseudostratified, or ciliated epithelium.
The combination of imaging and histopathology contributes to the diagnosis of esophageal cysts.
Treatment / Management
Medical therapy serves no role in the management of esophageal cysts. Surgical removal is the treatment of choice in most symptomatic cases. Simple cysts show enucleation, whereas duplications get excised. Traditionally, a posterolateral thoracotomy was performed to remove the cyst. However, more recently, video-assisted thoracoscopic surgery (VATS) and robotic-assisted thoracoscopic surgery (RATS) are available to perform enucleation and resection with better cosmetic outcomes.[11][28] Also, endoscopic submucosal tunnel dissection (ESTD) is an option to excise an esophageal cyst less invasively, but long-term outcomes and complications after this procedure require further evaluation.[29][30] Laparoscopic resection has been described as well, with this method being more common with esophageal cysts that are continuous with the mediastinum and abdominal cavity.[31](B3)
In asymptomatic cases, there are currently no clear guidelines on whether or not treatment is warranted. Surgery can be an option to prevent cases of ulceration, perforation, and rare instances of malignancy.[12][18][22](B3)
Differential Diagnosis
- Bronchogenic cyst
- Cervical duplication cyst
- Thyroglossal duct cyst
- Neuroenteric cyst
- Lipoma
- Lymphangioma
- Hemangioma
- Anterior meningocele
- Pericardial cyst
Prognosis
After treatment with full surgical enucleation and/or excision, patients overall do well both in the short term and long term. Recurrence is rare, but has been reported.[32]
Complications
The complications associated with esophageal cysts include heartburn, reflux esophagitis, rupture, obstruction, hemorrhage, infection, and malignancy.[28] Other complications related to esophageal cyst intervention include tracheal and esophageal injuries, pseudodiverticulum development, and nerve injury/paralysis.
Deterrence and Patient Education
Patients and family members should receive education about recognizing symptoms associated with esophageal cysts. If undergoing surgical intervention, patients should be informed and educated on any potential complications and have a follow-up visit scheduled with their physician.
Enhancing Healthcare Team Outcomes
The evaluation of esophageal cysts includes a thorough history, examination, diagnostic, and pathological testing. An interprofessional team, including primary care physicians, pharmacists, radiologists, gastroenterologists, surgeons, and specialty-trained nurses, can facilitate better recognition and management of esophageal cysts to prevent harmful outcomes and complications. The role of the nurse in the postoperative period is vital. Patients need both DVT and bedsore prophylaxis; nursing staff will be crucial in this regard, and must report any concerns to the treating clinician and interprofessional team. To prevent atelectasis, incentive spirometry should be encouraged. If the patient has a chest drain, the amount of air and fluid leak requires monitoring. [Level 5] Patient education is paramount. Length of follow-up after enucleation or excision varies, and there are no clear guidelines on whether or not surveillance imaging is necessary at this time.
Media
(Click Image to Enlarge)
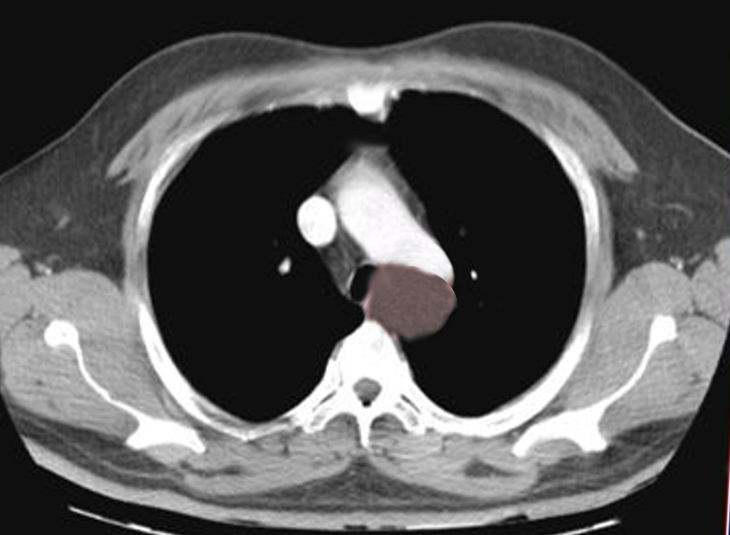
Esophageal cyst
Image courtesy S Bhimji MD
(Click Image to Enlarge)

Esophageal cyst
Image courtesy S Bhimji MD
References
Singhal V, Shenoy RD, Kamath N, Rao S. Mediastinal enteric cyst in a neonate. Journal of clinical neonatology. 2012 Jul:1(3):149-51. doi: 10.4103/2249-4847.101701. Epub [PubMed PMID: 24027713]
Level 3 (low-level) evidenceWhitaker JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. The American journal of gastroenterology. 1980 Apr:73(4):329-32 [PubMed PMID: 7416128]
Level 3 (low-level) evidenceWang B, Hunter WJ, Bin-Sagheer S, Bewtra C. Rare potential pitfall in endoscopic ultrasound-guided fine needle aspiration biopsy in gastric duplication cyst: a case report. Acta cytologica. 2009 Mar-Apr:53(2):219-22 [PubMed PMID: 19365980]
Level 3 (low-level) evidenceArbona JL, Fazzi JG, Mayoral J. Congenital esophageal cysts: case report and review of literature. The American journal of gastroenterology. 1984 Mar:79(3):177-82 [PubMed PMID: 6702802]
Level 3 (low-level) evidenceGeller A, Wang KK, DiMagno EP. Diagnosis of foregut duplication cysts by endoscopic ultrasonography. Gastroenterology. 1995 Sep:109(3):838-42 [PubMed PMID: 7657112]
Wang D, Du LC, Wang QX, Wang Z. Esophagectomy for a rapidly progressing esophageal duplication cyst. The Annals of thoracic surgery. 2015 Apr:99(4):e79-81. doi: 10.1016/j.athoracsur.2015.01.047. Epub [PubMed PMID: 25841854]
Berrocal T, Torres I, Gutiérrez J, Prieto C, del Hoyo ML, Lamas M. Congenital anomalies of the upper gastrointestinal tract. Radiographics : a review publication of the Radiological Society of North America, Inc. 1999 Jul-Aug:19(4):855-72 [PubMed PMID: 10464795]
Cuch B, Nachulewicz P, Wieczorek AP, Wozniak M, Pac-Kozuchowska E. Esophageal Duplication Cyst Treated Thoracoscopically During the Neonatal Period: Clinical Case Report. Medicine. 2015 Dec:94(49):e2270. doi: 10.1097/MD.0000000000002270. Epub [PubMed PMID: 26656375]
Level 3 (low-level) evidenceWootton-Gorges SL, Eckel GM, Poulos ND, Kappler S, Milstein JM. Duplication of the cervical esophagus: a case report and review of the literature. Pediatric radiology. 2002 Jul:32(7):533-5 [PubMed PMID: 12107589]
Level 3 (low-level) evidenceKawashima S, Segawa O, Kimura S, Tsuchiya M, Henmi N, Hasegawa H, Fujibayashi M, Naritaka Y. A case of cervical esophageal duplication cyst in a newborn infant. Surgical case reports. 2016 Dec:2(1):30. doi: 10.1186/s40792-016-0157-2. Epub 2016 Apr 1 [PubMed PMID: 27037803]
Level 3 (low-level) evidenceStringel G, Mercer S, Briggs V. Esophageal duplication cyst containing a foreign body. Canadian Medical Association journal. 1985 Mar 1:132(5):529-31 [PubMed PMID: 3971270]
Level 3 (low-level) evidenceLiu R, Adler DG. Duplication cysts: Diagnosis, management, and the role of endoscopic ultrasound. Endoscopic ultrasound. 2014 Jul:3(3):152-60. doi: 10.4103/2303-9027.138783. Epub [PubMed PMID: 25184121]
Birmole BJ, Kulkarni BK, Vaidya AS, Borwankar SS. Intrathoracic enteric foregut duplication cyst. Journal of postgraduate medicine. 1994 Oct-Dec:40(4):228-30 [PubMed PMID: 9136248]
Level 3 (low-level) evidenceBhatia V, Tajika M, Rastogi A. Upper gastrointestinal submucosal lesions--clinical and endosonographic evaluation and management. Tropical gastroenterology : official journal of the Digestive Diseases Foundation. 2010 Jan-Mar:31(1):5-29 [PubMed PMID: 20860221]
Sonthalia N, Jain SS, Surude RG, Mohite AR, Rathi PM. Congenital Esophageal Duplication Cyst: A Rare Cause of Dysphagia in an Adult. Gastroenterology research. 2016 Oct:9(4-5):79-82 [PubMed PMID: 27785331]
Ildstad ST, Tollerud DJ, Weiss RG, Ryan DP, McGowan MA, Martin LW. Duplications of the alimentary tract. Clinical characteristics, preferred treatment, and associated malformations. Annals of surgery. 1988 Aug:208(2):184-9 [PubMed PMID: 3401062]
Estefan Ventura D, Reibscheid S, Colleoni R, Tomaz Schettini S. Surgical images: soft tissue. Tubular duplication of the esophagus. Canadian journal of surgery. Journal canadien de chirurgie. 2008 Jun:51(3):205-6 [PubMed PMID: 18682751]
Level 3 (low-level) evidenceWiechowska-Kozłowska A, Wunsch E, Majewski M, Milkiewicz P. Esophageal duplication cysts: endosonographic findings in asymptomatic patients. World journal of gastroenterology. 2012 Mar 21:18(11):1270-2. doi: 10.3748/wjg.v18.i11.1270. Epub [PubMed PMID: 22468092]
Level 3 (low-level) evidenceHuff WD, Adams G, Schoepfle WJ. Back pain with a congenital cyst of the esophagus. The Journal of the American Board of Family Practice. 1989 Oct-Dec:2(4):275-8 [PubMed PMID: 2801195]
Level 3 (low-level) evidenceSun CF, Chen CH, Ke PZ, Ho TL, Lin CH. Esophageal duplication cyst presenting with stridor in a child with congenital pulmonary airway malformation: A case report and literature review. Medicine. 2019 Jul:98(28):e16364. doi: 10.1097/MD.0000000000016364. Epub [PubMed PMID: 31305433]
Level 3 (low-level) evidenceSethi GK, Marsden J, Johnson D. Duplication cysts of the esophagus. Southern medical journal. 1974 May:67(5):616-8 [PubMed PMID: 4823366]
Singh S, Lal P, Sikora SS, Datta NR. Squamous cell carcinoma arising from a congenital duplication cyst of the esophagus in a young adult. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus. 2001:14(3-4):258-61 [PubMed PMID: 11869334]
Level 3 (low-level) evidenceGümüş M, Önder A, Firat U, Kapan M, Önder H, Gırgın S. Hydatid cyst-like intra-abdominal esophageal duplication cyst in an endemic region. The Turkish journal of gastroenterology : the official journal of Turkish Society of Gastroenterology. 2011 Oct:22(5):557-8 [PubMed PMID: 22234770]
Level 3 (low-level) evidenceWeiss LM, Fagelman D, Warhit JM. CT demonstration of an esophageal duplication cyst. Journal of computer assisted tomography. 1983 Aug:7(4):716-8 [PubMed PMID: 6863677]
Level 3 (low-level) evidenceKuhlman JE, Fishman EK, Wang KP, Siegelman SS. Esophageal duplication cyst: CT and transesophageal needle aspiration. AJR. American journal of roentgenology. 1985 Sep:145(3):531-2 [PubMed PMID: 3875256]
Level 3 (low-level) evidenceDiehl DL, Cheruvattath R, Facktor MA, Go BD. Infection after endoscopic ultrasound-guided aspiration of mediastinal cysts. Interactive cardiovascular and thoracic surgery. 2010 Feb:10(2):338-40. doi: 10.1510/icvts.2009.217067. Epub 2009 Nov 16 [PubMed PMID: 19917550]
Level 3 (low-level) evidenceMansard MJ, Rao U, Rebala P, Rao GV, Reddy DN. Esophageal duplication cyst masquerading as a stromal tumor in an adult. The Indian journal of surgery. 2011 Dec:73(6):441-3. doi: 10.1007/s12262-011-0250-5. Epub 2011 Apr 8 [PubMed PMID: 23204704]
Obasi PC, Hebra A, Varela JC. Excision of esophageal duplication cysts with robotic-assisted thoracoscopic surgery. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2011 Apr-Jun:15(2):244-7. doi: 10.4293/108680811X13071180406961. Epub [PubMed PMID: 21902985]
Level 3 (low-level) evidenceTang X, Jiang B, Gong W. Endoscopic submucosal tunnel dissection of a bronchogenic esophageal cyst. Endoscopy. 2014:46 Suppl 1 UCTN():E626-7. doi: 10.1055/s-0034-1390780. Epub 2014 Dec 11 [PubMed PMID: 25502273]
Level 3 (low-level) evidenceYang X, Zong Y, Zhao HY, Wu YD, Ji M. Complete excision of esophageal bronchogenic cyst by endoscopic submucosal tunnel dissection: a case presentation. BMC gastroenterology. 2019 Aug 28:19(1):155. doi: 10.1186/s12876-019-1072-3. Epub 2019 Aug 28 [PubMed PMID: 31462259]
Level 3 (low-level) evidenceWatanobe I, Ito Y, Akimoto E, Sekine Y, Haruyama Y, Amemiya K, Kawano F, Fujita S, Omori S, Miyano S, Kosaka T, Machida M, Kitabatake T, Kojima K, Sakaguchi A, Ogura K, Matsumoto T. Laparoscopic resection of an intra-abdominal esophageal duplication cyst: a case report and literature review. Case reports in surgery. 2015:2015():940768. doi: 10.1155/2015/940768. Epub 2015 Mar 26 [PubMed PMID: 25883826]
Level 3 (low-level) evidenceDuan X, Cui Y, He Y, Xu S. Acute attack of recurrent esophageal duplication cyst in an adult: case report and literature review. Journal of thoracic disease. 2018 May:10(5):E335-E339. doi: 10.21037/jtd.2018.04.89. Epub [PubMed PMID: 29997988]
Level 3 (low-level) evidence