
Introduction
Electrical alternans is defined as alternating QRS amplitude that is seen in any or all leads on an electrocardiogram (ECG) with no additional changes to the conduction pathways of the heart. This rhythm is typically associated with pericardial effusion via the “swinging heart” from the fluid surrounding the heart. However, electrical alternans is also associated with other pathologies including but not limited to ventricular tachycardia, Wolff-Parkinson-White (WPW), accelerated idioventricular rhythm, and supraventricular tachycardia.[1] Understanding the varied pathologies causing this ECG finding is key to evaluation and if necessary, treatment success.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Electrical alternans is most commonly attributed to pericardial effusion and tamponade pathology. In this scenario, the classic ECG rhythm is due to the pendulum-like motion and rotation of the heart from beat to beat manifesting as varied amplitudes when detected by the ECG electrodes. Electrical alternans is also seen in conduction and refractory changes in various rhythms including those mentioned above resulting in varied QRS amplitudes as detected by the electrodes. The mechanism that leads to these ECG changes will be further discussed in pathophysiology.[2][3]
Epidemiology
Electrical alternans is usually associated with pericardial effusion which is associated with many disease states including infection, inflammatory syndromes, trauma, malignancy, and idiopathic to name a few. Although the majority of effusions have an underlying cause, as much as 20% are from unknown causes, making approach and eventual treatment challenging. Incidence of pericardial effusion overall is low in symptomatic patients presenting with ECG findings of alternans. Despite this, effusion should remain on the differential as this is a potentially fatal complication if it remains unrecognized.[4] As mentioned above, there are additional pathologies that can lead to alternans on ECG also includes various arrhythmias and conduction pathway abnormalities. Each of these pathologies have various and unique pathologies and further discussion of these will not be included in this paper.
Pathophysiology
Electrical alternans is the alternating voltage noted in the QRS complexes seen on an ECG; refer to the image below. Electrical alternans can be diagnosed by the varying changes in the amplitude of the QRS complex. Of note, T-wave alternans can be present as well. This review focuses on the QRS complex alternans. These changes are thought to be caused by the anterior-posterior swinging of the heart with each contraction in the fluid-filled pericardial sac. As the heart swings, the electrical signals detected by the electrodes travel over a greater distance through the fluid resulting in reduced voltage at the electrodes. Alternans may also be seen in other physiology including myocardial disease, pneumothorax or emphysema wherein the electrical conductivity of the tissues between the heart and the electrodes are affected causing variations in the QRS amplitudes. Other causes of electrical alternans can include AV nodal reentrant tachycardia, bundle branch block, Wolff-Parkinson-White syndrome (WOW), late premature ventricular complexes where the underlying change in conduction pathway is responsible for the change in the QRS amplitude observed on the ECG. In some ventricular tachycardias, changes in ion concentrations around the myocardium can result in regional changes in potassium causing varied action potential instability creating an alternans type pattern as different regions of the heart depolarize at varied levels of excitation.[5] It has been shown that deep breathing may be a cause of alternans in the precordial leads caused by the additional distance the electrical signal travels at full inhalation where electrical signals are reduced at the electrodes.
History and Physical
When electrical alternans is found on an ECG, further evaluation is needed because treatment will vary based on the underlying pathophysiology. Therefore, a thorough history and examination of the patient are necessary to focus on the cardiovascular and pulmonary exam. In the case of pericardial effusion, patients are usually asymptomatic unless tamponade physiology is present. Signs of tamponade include Becks triad: hypotension, muffled heart sounds, and distended neck veins. Additional signs of tamponade may also include tachypnea and dyspnea in the form of Kussmaul breathing and Pulsus Paradoxus.[6] In the case of arrhythmias, as mentioned above, patients may present with tachycardia and associated symptoms of light-headedness, fatigue, chest pain, shortness of breath, syncope, among others along with a potential history of cardiac conduction abnormalities. Based on this, a further cardiac history, including family history, may need to be obtained.
Evaluation
When electrical alternans is present on an ECG, further evaluation is needed to find the underlying cause as mentioned above. When considering a pericardial effusion, a transthoracic echocardiogram (TTE) is the first-line imaging modality. In the unstable patient, bedside echocardiogram is even more important as TTE provides very high sensitivity (near 100%) in diagnosing pericardial effusion.[7]
Treatment / Management
Once diagnosed, to treat serious tamponade pathology; you must first address resuscitative measures including intravenous (IV) access, oxygen as needed and cardiac monitoring. Intravenous fluid boluses may be needed to promote right heart filling and function to temporize poor hemodynamics. For definitive treatment of tamponade, however, a pericardiocentesis is necessary. This is typically performed in a cardiac catheterization lab in a non-life-threatening situation. However, in urgent conditions, for example, in patients at risk of arrest or who may have arrested, percutaneous pericardiocentesis may be performed in the emergency department. Once a pericardiocentesis and removal of fluid have been performed, and the patient is stabilized, further investigation is required to determine what pathophysiological process lead to the effusion.
For other causes of alternans including WPW, ventricular arrhythmias, and bundle branch block, therapy must be directed toward the underlying cause, with the early emphasis on hemodynamic stability of the patient as the first step in treatment.
Differential Diagnosis
- Alternans bundle branch block
- Aortic stenosis
- Air embolism
- Bigeminy
- Cardiac rupture
- Digoxin toxicity- bidirectional ventricular tachycardia
- Myocardial contusion
- Massive pulmonary embolus
- Wide varying tidal volumes in severe tachypnea
- Ventricular septal defect
Pearls and Other Issues
Electrical alternans, although considered pathognomonic for pericardial effusion, is not a diagnostic factor for effusion and cardiac tamponade as other pathologies can result in this ECG finding. When present on an ECG, early evaluation of the patient’s vitals and overall presentation are imperative. If and when the patient is stable following resuscitation, further evaluation of the heart, including echocardiogram, is necessary to identify the underlying pathology and rule out tamponade. If tamponade physiology is present on imaging or hemodynamic instability from tachycardic rhythms is present further action needs to be taken with a focus on hemodynamic stability, then correction of the underlying pathophysiology.
Enhancing Healthcare Team Outcomes
Healthcare workers should be aware that Electrical alternans, although considered pathognomonic for pericardial effusion, is not a diagnostic factor for effusion and cardiac tamponade as other pathologies can result in this ECG finding. If the rhythm is noted on the ECG, the next step is to order an echocardiogram and consult with a cardiologist. If the patient is hemodynamically unstable, immediate drainage of the pericardial fluid is required. The most compelling fact is that electrical alternans is not a benign event and one should always rule out cardiac tamponade first.
Media
(Click Image to Enlarge)
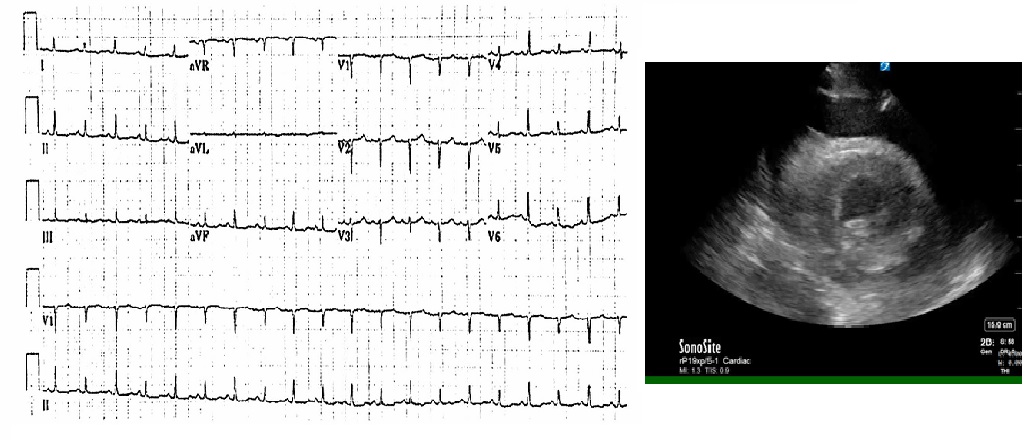
ECG of electrical alternans
Contributed by Brandon Barth, MD and Magaret Strecker-Mcgraw, MD
References
Goyal M, Woods KM, Atwood JE. Electrical alternans: a sign, not a diagnosis. Southern medical journal. 2013 Aug:106(8):485-9. doi: 10.1097/SMJ.0b013e3182a1456c. Epub [PubMed PMID: 23912146]
Hazim A, Belhamadia Y, Dubljevic S. Mechanical perturbation control of cardiac alternans. Physical review. E. 2018 May:97(5-1):052407. doi: 10.1103/PhysRevE.97.052407. Epub [PubMed PMID: 29906969]
Wilson LD, Jeyaraj D, Wan X, Hoeker GS, Said TH, Gittinger M, Laurita KR, Rosenbaum DS. Heart failure enhances susceptibility to arrhythmogenic cardiac alternans. Heart rhythm. 2009 Feb:6(2):251-9. doi: 10.1016/j.hrthm.2008.11.008. Epub 2008 Nov 8 [PubMed PMID: 19187920]
Level 3 (low-level) evidenceBlaivas M, Incidence of pericardial effusion in patients presenting to the emergency department with unexplained dyspnea. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2001 Dec [PubMed PMID: 11733291]
Kandel SM, Roth BJ. ELECTRICAL INSTABILITY DUE TO REGIONAL INCREASE IN EXTRACELLULAR POTASSIUM ION CONCENTRATION. Journal of nature and science. 2015 Aug:1(8):. pii: e160. Epub [PubMed PMID: 28795153]
Honasoge AP, Dubbs SB. Rapid Fire: Pericardial Effusion and Tamponade. Emergency medicine clinics of North America. 2018 Aug:36(3):557-565. doi: 10.1016/j.emc.2018.04.004. Epub 2018 Jun 11 [PubMed PMID: 30037442]
Xu B, Kwon DH, Klein AL. Imaging of the Pericardium: A Multimodality Cardiovascular Imaging Update. Cardiology clinics. 2017 Nov:35(4):491-503. doi: 10.1016/j.ccl.2017.07.003. Epub [PubMed PMID: 29025541]