
 Anatomy, Head and Neck, Parathyroid, Ectopic Glands
Anatomy, Head and Neck, Parathyroid, Ectopic Glands
Introduction
Hyperparathyroidism is a condition mainly due to adenomas of the parathyroid that are overactive. Most cases of hyperparathyroidism go unnoticed because they are clinically silent. When symptomatic, the patient usually requires a referral to an otolaryngologist that will decide if surgery or medical intervention would better benefit the patient. If surgery is the option chosen, the patient will undergo imaging and a parathyroidectomy. Imaging is used to locate the parathyroid glands since these structures are notorious for being ectopically placed along a median line. If the clinical signs of hyperparathyroidism continue post-operatively, these serve as clues to the head and neck surgeon that there may be remaining tissue in the parathyroid, a parathyroid ectopically placed, or supernumerary parathyroids. Positive labs for continued primary hyperparathyroidism include hypercalcemia and high levels of PTH.[1] Symptoms of retained parathyroid tissue mirror symptoms of hypercalcemia: renal stones, osteoporosis, confusion, constipation, and weakness.[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The parathyroid glands are typically located posterior to the thyroid glands, but anterior relative to the rest of the neck. These glands primarily function as the regulators of calcium homeostasis. If there is normal anatomy, the inferior parathyroid glands are located at the lower poles of the thyroid gland, while the superior parathyroid glands are present near the upper poles.[3] Typically, a person has four parathyroid glands, but the number of glands can vary from one, up to as high as twelve glands in total. [1] The parathyroid glands are activated via G-protein coupled receptors (GPCRs) that are sensitive to surrounding parathyroid hormone. These GPCRs exist on bone and kidney cells.[4] The parathyroid hormone itself functions by increasing renal tubular calcium reabsorption, enhancing net bone resorption, as well as stimulation net intestinal calcium absorption by increasing Vitamin D because of activation of 1-alpha-hydroxylase in the proximal convoluted tubule.[5] Intermittent binding of PTH to its GPCR leads to bone formation, while constant binding leads to bone degradation.[4] Intermittent PTH activates osteoblast differentiation which enhances bone formation, resulting in net bone gain; continuous PTH leads to greater osteoclastogenesis.[6] PTH regulation is by ionized calcium, extracellular phosphate, and vitamin D. In contrast to other regulatory systems, the parathyroids are not under the direct influence of other glands and organs. Usually, in primary hyperparathyroidism, calcium levels remain elevated, while phosphate and Vitamin D levels are low (attempting to initiate negative feedback).[5]
Embryology
The upper parathyroid glands descend from the fourth pharyngeal pouch within the thyroid, while the lower parathyroid glands travel with the thymus in the third pharyngeal pouch.[3] Due to the line of migration from the mandibular angle to the mediastinum, the ectopic glands can be located anywhere along this median line.[7]
Blood Supply and Lymphatics
Inferior parathyroid adenomas are hypervascular and receive most of their blood supply from inferior thyroidal artery branches, while superior parathyroid adenomas receive their blood supply from the superior or inferior thyroidal artery branches. The ectopic parathyroid glands located in the mediastinum receive their vascular supply from the internal thoracic artery, specifically the thymic branch.[8]
Nerves
Recurrent laryngeal nerve injuries are the most feared complication of parathyroid and thyroid operations due to the subsequent rise in postoperative morbidity. Some other symptoms of recurrent laryngeal nerve injury include vocal cord paresis or palsy, dyspnea, and deglutition.[9]
Muscles
In some rare cases, ectopic parathyroid adenomas are present in the sternohyoid muscles.[10]
Physiologic Variants
Another identified cause of primary hyperparathyroidism is an autosomal dominant condition known as multiple endocrine neoplasia type 1 (MEN1). The usual treatment of MEN1 in the context of primary hyperparathyroidism is surgical removal, but this is complicated when the parathyroid gland is ectopic. Ectopic parathyroid glands are more common in MEN1 patients than sporadically hyper-parathyroid patients.[11]
Surgical Considerations
The upper parathyroid glands are found above the inferior thyroid artery, at the cervical level of the cricoid cartilage, and posterolaterally to the recurrent laryngeal nerve.[1] The upper parathyroid glands have to travel a shorter distance when compared to the lower parathyroid glands, so the upper parathyroid glands are generally not ectopic.[3] Regardless of this, there are many ectopic locations for the superior parathyroid glands, and they consist of the tracheoesophageal groove, posteromedial to the thyroid in the paraesophageal area, within the carotid sheath, within the thyroid gland itself, and in the mediastinum (anywhere from superficial to deep).[1] Typically, the inferior parathyroid glands are located below the inferior thyroid artery and anteromedially to the recurrent laryngeal nerve. Some usual ectopic locations for the inferior parathyroid glands include: within the thymus, the perithymic fac, the thyrothymic ligament, as well as within the carotid sheath, the thyroid glands themselves, and the anterior mediastinal glands.[1] The most common ectopic locations for the parathyroid are within the mediastinum, the thymus, and the thyroid gland. The rarest locations for ectopic parathyroid glands include within the vagus nerve or pharynx, and behind the esophagus.[10]
Clinical Significance
Today, the majority of ectopic parathyroid glands are relatively silent without clinical manifestations. Because of this, surgery is not usually a recommendation unless the patient has symptoms. Guidelines for surgery include adjusted calcium over 0.25 mmol/L above the reference range, urine calcium greater than 10 mmol/ 24 hours, more than 30% reduction in creatinine clearance, less than -2.5 bone density T-score, and being less than 50 years old. Active ectopic parathyroid gland complications include namely hypercalcemia, which results in an increased fracture rate (more commonly in females), kidney stone disease, hypertension, cardiac valve calcification, and neurological symptoms (such as weakness, anxiety, and depression). For those patients that do not meet surgery guidelines, medications can be used and include hormone replacement therapy (specifically in post-menopausal women to decrease fracture rates) and calcimimetics that inhibit the release of PTH by binding to calcium receptors and dominating the negative feedback loop.[2]
Other Issues
Usual imaging for parathyroid glands includes ultrasound and CT. Ectopic parathyroid glands are not readily visible with ultrasound, so technetium-sestamibi CT scanning may be a diagnostic option which has high sensitivity and specificity for parathyroid adenomas. [2] After removal, parathyroid glands are taken to pathology to determine malignancy status. Because the regulation of calcium is vital, many times, surgeons will autoimplant a parathyroid gland within the forearm of a patient. By doing this, the gland's functionality remains the same with a lower incidence of malignancy and hyperparathyroidism because of close monitoring by the physician and patient.[10]
Ectopic parathyroid management requires close collaboration with an interdisciplinary team that includes the family physician, specialists, nursing staff, and pharmacists; this interprofessional team approach best leads to optimal patient management and clinical results. [Level V]
Media
(Click Image to Enlarge)
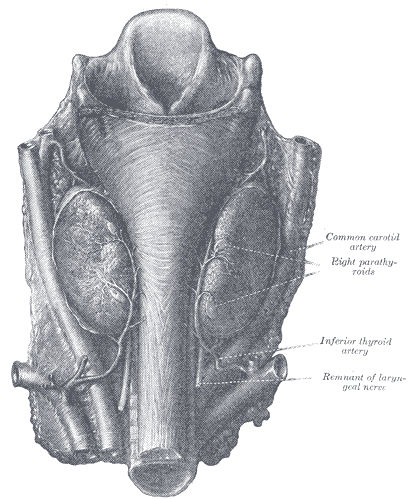
The Parathyroid Glands
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
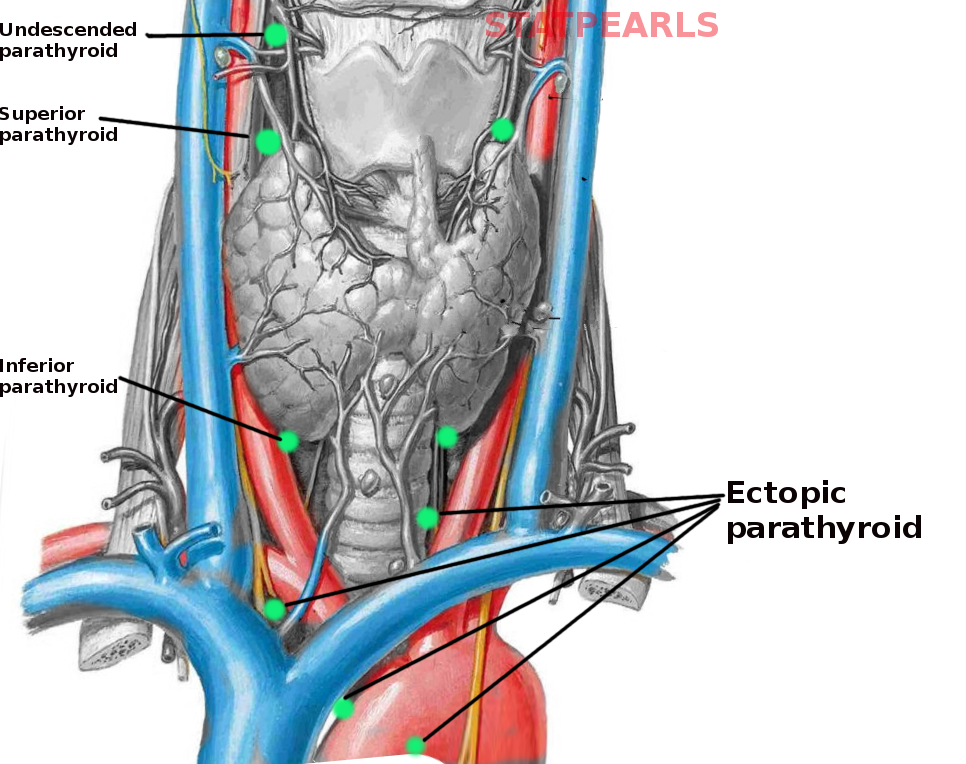
Ectopic parathyroid glands
Image courtesy S Bhimji MD
References
Caron NR, Sturgeon C, Clark OH. Persistent and recurrent hyperparathyroidism. Current treatment options in oncology. 2004 Aug:5(4):335-45 [PubMed PMID: 15233910]
Fraser WD. Hyperparathyroidism. Lancet (London, England). 2009 Jul 11:374(9684):145-58. doi: 10.1016/S0140-6736(09)60507-9. Epub [PubMed PMID: 19595349]
Taterra D, Wong LM, Vikse J, Sanna B, Pękala P, Walocha J, Cirocchi R, Tomaszewski K, Henry BM. The prevalence and anatomy of parathyroid glands: a meta-analysis with implications for parathyroid surgery. Langenbeck's archives of surgery. 2019 Feb:404(1):63-70. doi: 10.1007/s00423-019-01751-8. Epub 2019 Feb 14 [PubMed PMID: 30762091]
Level 1 (high-level) evidenceCulhane KJ, Belina ME, Sims JN, Cai Y, Liu Y, Wang PSP, Yan ECY. Parathyroid Hormone Senses Extracellular Calcium To Modulate Endocrine Signaling upon Binding to the Family B GPCR Parathyroid Hormone 1 Receptor. ACS chemical biology. 2018 Aug 17:13(8):2347-2358. doi: 10.1021/acschembio.8b00568. Epub 2018 Jul 11 [PubMed PMID: 29952553]
Schappacher-Tilp G, Cherif A, Fuertinger DH, Bushinsky D, Kotanko P. A mathematical model of parathyroid gland biology. Physiological reports. 2019 Apr:7(7):e14045. doi: 10.14814/phy2.14045. Epub [PubMed PMID: 30927339]
Choi H, Magyar CE, Nervina JM, Tetradis S. Different duration of parathyroid hormone exposure distinctively regulates primary response genes Nurr1 and RANKL in osteoblasts. PloS one. 2018:13(12):e0208514. doi: 10.1371/journal.pone.0208514. Epub 2018 Dec 21 [PubMed PMID: 30576321]
Patrinos A, Zarokosta M, Piperos T, Chrysikos D, Kakaviatos D, Theodoropoulos P, Kalles V, Tsiaoussis J, Noussios G, Mariolis-Sapsako T. WITHDRAWN: An anatomic aberration and a surgical challenge: Mediastinal parathyroid adenoma anterior the pericardium. A case report. International journal of surgery case reports. 2019:57():106-109. doi: 10.1016/j.ijscr.2019.03.014. Epub 2019 Mar 21 [PubMed PMID: 30943449]
Level 3 (low-level) evidenceLane MJ, Desser TS, Weigel RJ, Jeffrey RB Jr. Use of color and power Doppler sonography to identify feeding arteries associated with parathyroid adenomas. AJR. American journal of roentgenology. 1998 Sep:171(3):819-23 [PubMed PMID: 9725323]
Joliat GR, Guarnero V, Demartines N, Schweizer V, Matter M. Recurrent laryngeal nerve injury after thyroid and parathyroid surgery: Incidence and postoperative evolution assessment. Medicine. 2017 Apr:96(17):e6674. doi: 10.1097/MD.0000000000006674. Epub [PubMed PMID: 28445266]
Miura D. Ectopic parathyroid tumor in the sternohyoid muscles: supernumerary gland in a patient with MEN type 1. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2005 Aug:20(8):1478-9 [PubMed PMID: 16007345]
Level 3 (low-level) evidencePark HL, Yoo IR, Kim SH, Lee S. Multiple endocrine neoplasia type 1 with anterior mediastinal parathyroid adenoma: successful localization using Tc-99m sestamibi SPECT/CT. Annals of surgical treatment and research. 2016 Dec:91(6):323-326 [PubMed PMID: 27904855]