
 Anatomy, Head and Neck, Costocervical Trunk Arteries
Anatomy, Head and Neck, Costocervical Trunk Arteries
Introduction
The costocervical trunk is a branch of the subclavian artery which supplies the upper extremities and contributes partly to the blood supply of the head and neck. The subclavian artery has a different origin on each side. On the right side, it originates from the brachiocephalic trunk while stemming directly from the arch of the aorta on the left side.[1][2] It is critical to know the course of the subclavian artery, its branches, and its parts to get a comprehensive understanding of the costocervical trunk. The subclavian artery divides into three segments depending on their position relative to the scalenus anterior muscle. The first part of the subclavian artery extends from its root to the medial part of the scalenus muscle. The first segment of the subclavian artery gives rise to the internal thoracic artery(internal mammary artery)[3], vertebral artery, and thyrocervical trunk that supply the circle of Willis, breast tissue and thyroid tissue. The second part of the subclavian artery starts from the medial part of the scalenus muscle and extends to the lateral aspect of the scalenus muscle; This part gives rise to the costocervical trunk. The third part starts at the lateral aspect of the scalenus muscle and ends at the tip of the first rib, where it becomes the axillary artery.[4][5] Since we now know the exact origin of the costocervical trunk, we can go in-depth about delineating its details and importance.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The costocervical trunk arises directly from the posterior surface of the second part of the subclavian artery that lies posterior or medial to the scalenus anterior muscle.[6] The trunk passes in a posterosuperior direction and divides into two branches; superior intercostal artery(AKA: the highest intercostal or the supreme intercostal artery)[7] and deep cervical artery.[8][6] The superior intercostal artery, which is the first branch of the costocervical trunk travels posteriorly and inferiorly from where it originates along the posterior and medial aspect of the thorax. It lies between the necks of the first two ribs and the pleura, where it typically divides into two posterior intercostal arteries as it passes along the neck of the first rib. The two posterior intercostal arteries supply blood to the upper two intercostal spaces in a similar fashion to that of the lower posterior intercostal arteries.[9][10] The deep cervical artery along with the uppermost intercostal artery, the ascending pharyngeal artery, and the vertebral artery supply the joint capsules of the zygapophyseal joints and the synovial membranes with their villi of the cervical region. Some branches of the occipital artery and the vertebral artery may anastomose with the deep cervical artery anterior to the semispinalis capitis muscle.[11][6][12]
Embryology
The embryological development of the costocervical trunk follows the development of the subclavian artery on both sides. The development of the costocervical trunk is unique to each side since the development of the right and left subclavian arteries are different. The left subclavian artery arises only from the seventh intersegmental artery, while the right subclavian artery develops from three different embryological vessels. The fourth aortic arch gives rise to the first part of the subclavian artery. The right dorsal aorta gives rise to the second part of the right subclavian artery. The right seventh intersegmental artery gives rise to the last part of the subclavian artery.[13][5][14][15]
Nerves
The costocervical trunk is in the upper thorax and the lower part of the neck, which is closely related to some critical structures like the vagus nerve, recurrent laryngeal nerve, phrenic nerve, sympathetic ganglia, and brachial plexus. On the right side, the vagus nerve runs anterior to the subclavian artery and medial to the costocervical trunk. The recurrent laryngeal nerve, which is a vagus nerve branch, runs medial to the costocervical trunk and posterior to the root of the subclavian artery. The right phrenic nerve runs lateral to the costocervical trunk. On the left side, the vagus nerve, recurrent laryngeal nerve, and phrenic nerve run medial to the costocervical trunk. The left phrenic and vagus nerve pass anterior to the root of the subclavian artery. The left recurrent laryngeal nerve is longer than its right-side counterpart because it loops around the aortic arch instead of the subclavian artery. The brachial plexus runs posterior to the costocervical trunk and the anterior scalenus muscle. The superior intercostal artery, one of the costocervical trunk’s branches, runs medial to the anterior division of the first thoracic nerve. It also runs lateral to the first thoracic ganglion of the sympathetic trunk on both sides.
Muscles
The superior intercostal artery, which branches off the costocervical trunk, supplies the upper intercostal spaces. It passes inferiorly between the pleura and the necks of the first and second ribs, where it divides into two posterior intercostal arteries. The upper two intercostal muscles receive vascular supply from the superior intercostal artery and its branches. The deep cervical artery, which is another branch of the costocervical trunk, passes inferiorly above the eight cervical spinal nerve between the transverse process of the seventh cranial vertebra. From there, it ascends to the deep muscles of the neck and the back. It gives off muscular branches to supply the deep muscles in the neck and upper back.[16][17][18][12][19][20]
Physiologic Variants
Although the costocervical trunk commonly originates from the second part of the subclavian artery, it can originate from its third part or be absent en bloc. The two usual branches of the costocervical trunk include the deep cervical artery and the superior intercostal artery, which can arise independently from the subclavian artery if the trunk is absent. The superior intercostal artery can originate from the thyrocervical trunk or some of its branches like the inferior thyroid artery and the scapular artery. There are also reports that the superior intercostal artery can originate from the axillary artery, aortic arch, vertebral artery, or the second intercostal artery[21][22][23][24][25][26][27]
Clinical Significance
Costocervical trunk Pseudoaneurysms
Costocervical trunk pseudoaneurysms are extremely rare. They can be the result of bullectomy with pleural abrasion, blind cannulation of the jugular vein, secondary to infection like in the case of pulmonary tuberculosis, atherosclerosis of the costocervical trunk, trauma to the neck, or certain vasculitides (e.g., Takayasu arteritis).[28] Chest pain is a prevalent complaint in patients with costocervical trunk pseudoaneurysm. In rare cases, it can present with hemoptysis.[29] In the case of pseudoaneurysm rupturing, it can present as an expanding mass in the neck. The mass can affect the airways leading to labored breathing.[30][31] The gold standard method for diagnosing costocervical trunk aneurysms is CT angiography. Transcatheter embolization can be used for the management of ruptured costocervical trunk pseudoaneurysms.[30][32]
Takayasu arteritis
Takayasu arteritis, which can go by many other names like occlusive thromboaortopathy, pulseless disease, and Martorell syndrome, is inflammatory arteritis of the large blood vessels that involves the aorta and its major branches including the subclavian artery and the costocervical trunk. The condition can be detected clinically by the presence of bruits in the upper lateral anterior thorax or lower neck and the absence of a radial pulse. It can be accompanied by ischemic changes that involve the upper extremities and head and neck. The arteries supplying blood to the brain can undergo degenerative changes or form aneurysms that could eventually result in strokes. The reported presence of hypertension was in 33 to 83% of patients, Diminished or absent pulses in 84 to 96%, Takayasu retinopathy 37%.[33][34][35][36]
Perforation of the costocervical trunk
A transradial arterial approach to coronary angiography is associated with decreased vascular complications compared to a transfemoral arterial approach. It also allows for the early mobilization of patients. However, in rare cases, perforation of the costocervical trunk can take place shortly after a percutaneous transradial coronary intervention, which can result in a rapidly expanding cervical hematoma that presses on the airway and cause several breathing problems. This condition requires emergency intubation to preserve the patency of the airways.[37]
Collateral circulation
The first and second intercostal spaces are typically supplied with blood by the superior intercostal artery, which is of great clinical importance if the anterior intercostal or internal thoracic arteries become compromised. Moreover, the superior intercostal artery may supply blood to the descending aorta in the case of coarctation of the aorta through mediastinal collateral branches that bypass the coarctation.[10][7] It is a clinical observation that the mediastinal collateral arteries become hypertrophied in patients with obstruction of the subclavian artery or coarctation of the aorta. The mediastinal arteries play an important role in such instances as they connect the costocervical trunk, superior intercostal artery, or subclavian artery to the descending thoracic aorta bypassing the narrowed portion of the aorta.[10] In the case of occlusion of the internal carotid artery, blood can divert through several collateral arteries, including the occipital artery, vertebral artery, costocervical trunk, deep cervical artery, and thyrocervical trunk.[38] Aneurysm of the superior intercostal artery can be the result of the coarctation of the aorta or neurofibromatosis type 1. Selective endovascular embolization combing glue and micro-coils is the treatment of choice for superior intercostal artery aneurysms. Embolization of the superior intercostal artery is well-tolerated because the intercostal spaces supplied by it receive collateral arterial circulation from the anterior intercostal arteries.[39][40][7]
Media
(Click Image to Enlarge)
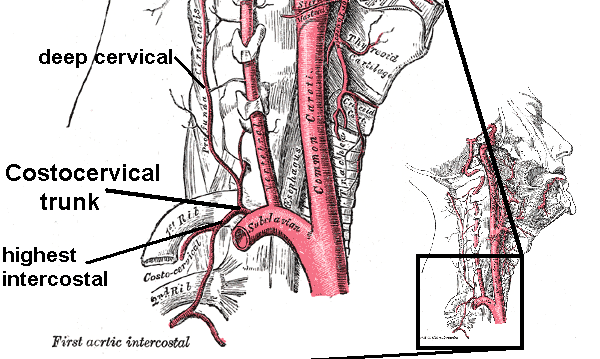
Costocervical trunk with branches. Right side. Deep Cervical Artery
Contributed by Wikimedia Commons,"Medical gallery of Mikael Häggström 2014" (Public Domain)
References
Azakie A, McElhinney DB, Messina LM, Stoney RJ. Common brachiocephalic trunk: strategies for revascularization. The Annals of thoracic surgery. 1999 Mar:67(3):657-60 [PubMed PMID: 10215206]
Level 2 (mid-level) evidenceMubarik A, Iqbal AM. Subclavian Artery Thrombosis. StatPearls. 2023 Jan:(): [PubMed PMID: 30725960]
Shahoud JS, Kerndt CC, Burns B. Anatomy, Thorax, Internal Mammary (Internal Thoracic) Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 30726022]
Rahimi O, Geiger Z. Anatomy, Thorax, Subclavian Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 30969558]
Aboulhoda BE, Ahmed RK, Awad AS. Clinically-relevant morphometric parameters and anatomical variations of the aortic arch branching pattern. Surgical and radiologic anatomy : SRA. 2019 Jul:41(7):731-744. doi: 10.1007/s00276-019-02215-w. Epub 2019 Mar 21 [PubMed PMID: 30900002]
Koizumi M, Sekiya S, Horiguchi M, Harada M. A study of the deep ascending cervical artery (new definition) and its relation to some other arteries in the human cervical region. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 1994 Jun:176(3):233-42 [PubMed PMID: 8059967]
Granger CJ, Martin AR. Anatomy, Thorax, Superior Intercostal Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 31751037]
Arslan M, Acar HI, Comert A, Tubbs RS. The Cervical Arteries: An Anatomical Study with Application to Avoid the Nerve Root and Spinal Cord Blood Supply. Turkish neurosurgery. 2018:28(2):234-240. doi: 10.5137/1019-5149.JTN.19469-16.1. Epub [PubMed PMID: 28266004]
Helm EJ, Rahman NM, Talakoub O, Fox DL, Gleeson FV. Course and variation of the intercostal artery by CT scan. Chest. 2013 Mar:143(3):634-639. doi: 10.1378/chest.12-1285. Epub [PubMed PMID: 23079732]
Kirks DR, Currarino G, Chen JT. Mediastinal collateral arteries: important vessels in coarctation of the aorta. AJR. American journal of roentgenology. 1986 Apr:146(4):757-62 [PubMed PMID: 3485349]
Level 3 (low-level) evidenceSu WD, Ohtsuka A, Taguchi T, Murakami T. Typology of the arteries in the human scalenus region, with special reference to the accessory ascending cervical artery. Acta medica Okayama. 2000 Dec:54(6):243-52 [PubMed PMID: 11132917]
Koga M, Hattori G, Maeda M, Nakamura Y, Miyagi T, Okura A, Morioka M, Uchikado H. Deep Cervical Artery as a Source of Bleeding in Postoperative Spinal Epidural Hematoma: A Case Report. NMC case report journal. 2019 Aug:6(3):87-90. doi: 10.2176/nmccrj.cr.2018-0214. Epub 2019 May 25 [PubMed PMID: 31417838]
Level 3 (low-level) evidenceKau T, Sinzig M, Gasser J, Lesnik G, Rabitsch E, Celedin S, Eicher W, Illiasch H, Hausegger KA. Aortic development and anomalies. Seminars in interventional radiology. 2007 Jun:24(2):141-52. doi: 10.1055/s-2007-980040. Epub [PubMed PMID: 21326792]
Gailloud P. The supreme intercostal artery includes the last cervical intersegmental artery (C7) - angiographic validation of the intersegmental nomenclature proposed by Dorcas Padget in 1954. Anatomical record (Hoboken, N.J. : 2007). 2014 May:297(5):810-8. doi: 10.1002/ar.22893. Epub 2014 Mar 7 [PubMed PMID: 24610867]
Level 1 (high-level) evidencePanakkal BJ, Rajesh GN, Parakkal HB, Subramaniam G, Vellani H, Sajeev CG. Bilateral variant origin of subclavian artery branches. BJR case reports. 2016:2(3):20150429. doi: 10.1259/bjrcr.20150429. Epub 2016 Jul 28 [PubMed PMID: 30459983]
Level 3 (low-level) evidenceHenson B, Kadiyala B, Edens MA. Anatomy, Back, Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30725759]
Sutcliffe P, Lasrado S. Anatomy, Head and Neck, Deep Cervical Neck Fascia. StatPearls. 2023 Jan:(): [PubMed PMID: 31082135]
Casale J, Geiger Z. Anatomy, Head and Neck, Posterior Neck Triangle. StatPearls. 2023 Jan:(): [PubMed PMID: 30725974]
Di Santo D, Giordano L, Bertazzoni G, Galli A, Tulli M, Bussi M. Rupture of the extracranial carotid artery caused by misdiagnosed infected pseudoaneurysm during deep cervical abscess drainage: A case report. Auris, nasus, larynx. 2017 Jun:44(3):355-358. doi: 10.1016/j.anl.2016.06.004. Epub 2016 Jun 23 [PubMed PMID: 27346681]
Level 3 (low-level) evidenceGofur EM, Bordoni B. Anatomy, Head and Neck: Cerebral Blood Flow. StatPearls. 2023 Jan:(): [PubMed PMID: 30844161]
Gailloud P. The supreme intercostal artery in its most rudimentary form does not branch off any intercostal arteries. Anatomical record (Hoboken, N.J. : 2007). 2015 May:298(5):781-2. doi: 10.1002/ar.23092. Epub 2014 Nov 20 [PubMed PMID: 25388017]
Level 3 (low-level) evidenceTubbs RS, Salter G, Wellons JC 3rd, Oakes WJ. Blood supply of the human cervical sympathetic chain and ganglia. European journal of morphology. 2002 Dec:40(5):283-8 [PubMed PMID: 15101443]
Brasileiro Filho G, Pena SD. Molecular biological techniques for the diagnosis of infectious diseases. Revista da Sociedade Brasileira de Medicina Tropical. 1992 Jan-Mar:25(1):59-71 [PubMed PMID: 1308067]
Yücel AH, Kizilkanat E, Ozdemir CO. The variations of the subclavian artery and its branches. Okajimas folia anatomica Japonica. 1999 Dec:76(5):255-61 [PubMed PMID: 10693329]
Takemura A, Okuda H, Oda K, Fang YR, Hsieh HM, Ohta Y. [A case of the right subclavian artery as the last branch of the aortic arch in the human fetus and a new classification on these variations]. Kaibogaku zasshi. Journal of anatomy. 1990 Oct:65(5):374-80 [PubMed PMID: 2077810]
Level 3 (low-level) evidenceYuan SM. Isolated costal cartilage fractures: the radiographically overlooked injuries. Folia morphologica. 2017:76(1):139-142. doi: 10.5603/FM.a2016.0030. Epub 2016 Nov 10 [PubMed PMID: 27830867]
Hara M, Kitase M, Satake M, Miyagawa H, Ogino H, Itoh M, Ohba S. A case of right-sided aortic arch with isolation of the left subclavian artery: CT findings. Radiation medicine. 2001 Jan-Feb:19(1):33-6 [PubMed PMID: 11305616]
Level 3 (low-level) evidenceYu D, Sun XW, Chen C, Jie B, Jiang S. Endovascular coil embolization of a costocervical trunk pseudoaneurysm after bullectomy with pleural abrasion. Vascular and endovascular surgery. 2014 Jan:48(1):74-6. doi: 10.1177/1538574413502550. Epub 2013 Sep 16 [PubMed PMID: 24043488]
Level 3 (low-level) evidenceSinghal M, Giragani S, Lal A, Sharma A, Khandelwal N. An unusual cause of hemoptysis: costocervical trunk pseudoaneurysm. Emergency radiology. 2011 Jan:18(1):53-5. doi: 10.1007/s10140-010-0911-x. Epub 2010 Oct 7 [PubMed PMID: 20927565]
Level 3 (low-level) evidenceLang EV, Picus D. Delayed rupture of a pseudoaneurysm of the costocervical trunk: treatment with therapeutic embolization. Radiology. 1991 Feb:178(2):352 [PubMed PMID: 1987591]
Level 3 (low-level) evidenceHoonjan B, Thayur N, Abu-Own A. Aneurysmal rupture of the costo-cervical trunk in a patient with neurofibromatosis type 1: A case report. International journal of surgery case reports. 2014:5(2):100-3. doi: 10.1016/j.ijscr.2013.12.023. Epub 2013 Dec 30 [PubMed PMID: 24463561]
Level 3 (low-level) evidenceKauppila LI, Penttilä A. Postmortem angiographic study of degenerative vascular changes in arteries supplying the cervicobrachial region. Annals of the rheumatic diseases. 1994 Feb:53(2):94-9 [PubMed PMID: 8129468]
Johnston SL, Lock RJ, Gompels MM. Takayasu arteritis: a review. Journal of clinical pathology. 2002 Jul:55(7):481-6 [PubMed PMID: 12101189]
Vaideeswar P, Deshpande JR. Pathology of Takayasu arteritis: A brief review. Annals of pediatric cardiology. 2013 Jan:6(1):52-8. doi: 10.4103/0974-2069.107235. Epub [PubMed PMID: 23626437]
Espinoza JL, Ai S, Matsumura I. New Insights on the Pathogenesis of Takayasu Arteritis: Revisiting the Microbial Theory. Pathogens (Basel, Switzerland). 2018 Sep 6:7(3):. doi: 10.3390/pathogens7030073. Epub 2018 Sep 6 [PubMed PMID: 30200570]
Ezhilnilavan S, Priyamvada PS, Swamiappan E, Haridasan S, Parameswaran S. Pseudoaneurysm of Thyrocervical Trunk Following Left Internal Jugular Vein Cannulation. Indian journal of nephrology. 2018 Mar-Apr:28(2):173-174. doi: 10.4103/ijn.IJN_170_17. Epub [PubMed PMID: 29861572]
Farooqi F, Alexander J, Sarma A. Rare vascular perforation complicating radial approach to percutaneous coronary angioplasty. BMJ case reports. 2013 Jan 28:2013():. doi: 10.1136/bcr-2012-007732. Epub 2013 Jan 28 [PubMed PMID: 23362057]
Level 3 (low-level) evidenceWang J, Zheng C, Hou B, Huang A, Zhang X, Du B. Four collateral circulation pathways were observed after common carotid artery occlusion. BMC neurology. 2019 Aug 20:19(1):201. doi: 10.1186/s12883-019-1425-0. Epub 2019 Aug 20 [PubMed PMID: 31429719]
Fenwick A, Omotoso P, Ferguson D. Endovascular management of unruptured intercostal artery aneurysms. CVIR endovascular. 2019:2(1):2. doi: 10.1186/s42155-018-0048-7. Epub 2019 Jan 4 [PubMed PMID: 30652168]
Aizawa K, Iwashita C, Saito T, Misawa Y. Spontaneous rupture of an intercostal artery in a patient with neurofibromatosis type 1. Interactive cardiovascular and thoracic surgery. 2010 Jan:10(1):128-30. doi: 10.1510/icvts.2009.222125. Epub 2009 Oct 15 [PubMed PMID: 19833637]
Level 3 (low-level) evidence