
Indications
FDA Approved Uses
1. Angiotensin-converting enzyme (ACE) inhibitors are useful as adjunctive therapy in systolic heart failure (HF). HF guidelines recommend ACE inhibitors to help prevent HF in patients with a reduced ejection fraction (EF) who also have a history of myocardial infarction (MI), and to prevent HF in any patient with a reduced ejection fraction (EF), or to treat patients with heart failure and reduced EF.
2. ACE inhibitors can be used to treat hypertension (HTN) either alone or in conjunction with other antihypertensives in adults or children over six years old. Hypertension guidelines recommend initiating ACE inhibitors to manage HTN to lower blood pressure (BP). According to the American College of Cardiology, treatment recommendations exist based on various patient populations.[1] These are:
- Patients with daytime BP out of the office at greater than 135 mmHg systolic or greater than 85 mmHg diastolic; this is substitutable with office blood pressure readings of over 140/90 mmHg
- Patients with an in-office or out-of-office BP exceeding 130 mmHg systolic or over 80 mmHg diastolic and the addition of the following factors:
- History of cardiovascular disease
- Type 2 diabetes mellitus
- Chronic kidney disease
- Age 65 or older
3. Patients with chronic kidney disease (CKD) and HTN:
- Regardless of race or diabetes mellitus status, ACE inhibitors are recommended as initial therapy to improve kidney outcomes.
- In the non-Black population with diabetes mellitus and without CKD, initial antihypertensive therapy should include either thiazide diuretic, calcium channel blocker (CCB), ACE inhibitor, or angiotensin receptor blocker (ARB).
- In the Black population with diabetes mellitus and without CKD, initial antihypertensive therapy should include a thiazide diuretic or CCB instead of an ACE inhibitor or ARB.
4. Patients with coronary artery disease (CAD) and HTN:
- ACE inhibitors are recommended as part of a regimen in patients with HTN and chronic stable angina if there is a history of left ventricular dysfunction, diabetes mellitus, or CKD.
5. Patients with ST-elevated myocardial infarction (STEMI):
- ACE inhibitors should be initiated within 24 hours of all STEMI, specifically in patients with anterior MI, heart failure, or left ventricular (LV) ejection fraction (EF) of 40% or less.
- ACE inhibitors show efficacy in treatment due to the overall reduction of mortality in multiple disease states. There is evidence of mortality benefits in patients with hypertension, heart failure, Acute MI, and diabetes mellitus.[2][3][4]
Non-FDA Uses
ACE inhibitors may delay the progression of nephropathy and reduce the risks of cardiovascular events in hypertensive patients with diabetes mellitus type I and type II. The addition of an ACE inhibitor has shown a significant reduction in serum creatinine in hypertensive and normotensive patients with albuminuria. ACE inhibitor therapy has shown a significant decrease in the progression of diabetic nephropathy.[5][6]
Krecak I. et al. found evidence that ACE inhibitors might have renoprotective properties in patients with polycythemia vera.[7]
Yao J.et al. discovered that ACE inhibitors improve insulin sensitivity in hypertensive patients with diabetes mellitus compared to angiotensin II receptor blockers.[8]
Salmenkari H. et al. found evidence that ACE inhibitors and angiotensin II receptor blockers use in patients with inflammatory bowel disease have fewer hospitalizations, glucocorticoid use, and a milder disease course.[9]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
The angiotensin-converting-enzyme (ACE) is involved in the renin-angiotensin-aldosterone system (RAAS; media item 1) and stimulates the conversion of angiotensin I to angiotensin II. ACE inhibitors are competitive inhibitors of ACE, which prevent the conversion of angiotensin I to angiotensin II. Angiotensin II acts as a potent vasoconstrictor that, when inhibited, can reduce blood pressure by dilating vessels and decreasing aldosterone secretion.[10][2][3]
It is essential to understand the role of the RAAS hormonal system in depth to appreciate the therapeutic effects of ACE inhibitors and understand why this is a target for hypertensive therapy. Initially, afferent arteriole juxtaglomerular cells synthesize prorenin, which is actively cleaved to renin. Angiotensinogen produced from the liver is then cleaved by renin to form angiotensin I. The angiotensin I molecule is converted to angiotensin II by ACE. Angiotensin II is a molecule that has significant actions on various systems. Initially, angiotensin II induces vasoconstriction, which ultimately increases systemic blood pressure.[11] Angiotensin II stimulates the adrenal cortex to produce aldosterone and the pituitary to produce antidiuretic hormone. Aldosterone induces sodium reabsorption and, in turn, water reabsorption through internal mineralocorticoid receptor activity.[12]
Antidiuretic hormone increases the synthesis of aquaporin-2 channels in the collecting duct inducing selective reabsorption of water. Actions of angiotensin-II and aldosterone lead to adverse cardiac remodeling. ACE inhibitors prevent adverse cardiac remodeling by reducing the concentrations of angiotensin-II and aldosterone.[13]
Administration
ACE inhibitors are most commonly administered as oral agents, but intravenous forms are available. These medications most commonly end with the suffix '-pril.' Examples include lisinopril, ramipril, and captopril.
ACE Inhibitors are Classified into Three Groups According to Chemical Structure
- Sulfhydryl-containing ACE inhibitor. Captopril – Hypertension therapy is 25 mg, either BID or TID, with a maximum of 450 mg. Heart failure therapy is 6.25 mg TID, with a maximum of 450 mg.
- Phosphorus-containing ACE inhibitor. Fosinopril – Hypertension therapy dosing is 10 mg, increasing to a maximum dose of 80 mg. May split into two equal doses during the day to control blood pressure. Heart failure therapy is 5 to 10 mg daily to a maximum dose of 40 mg.
- Dicarboxylic-containing ACE inhibitors: see table
| ACE inhibitor | Initial dose per day for hypertension | The maximum dose per day for hypertension | Initial dose per day for Heart Failure | The maximum dose per day for heart failure |
| Benazepril | 10 mg | 80 mg | - | - |
| Enalapril | 5 mg | 40 mg | 2.5 mg | 40 mg |
| Lisinopril | 10 mg | 80 mg | 2.5-5 mg | 40 mg |
| Moexipril | 7.5 mg | 30 mg | - | - |
| Perindopril | 4 mg | 16 mg | 2 mg | 16 mg |
| Quinapril | 10-2 0mg | 80 mg | 5 mg BID | 40 mg |
| Ramipril | 2.5 mg | 20 mg | 1.25-2.5 mg | 10 mg |
| Trandolapril | 1-2 mg | 8 mg | 1 mg | 4 mg |
General Dosing Information
All ACE inhibitors are prescribed orally, except for enalapril, which can be given intravenously. Enalapril's IV dosage is initially 0.625 to 1.25 mg every 6 hours. Dosage titration up can be to 5 mg IV every 6 hours. Geriatric dosing should be initiated at the lower end of the adult dosing regimen.
There should be a dosage decrease in patients with heart failure, salt-depleted patients, and/or renal impairment.
Lisinopril and captopril are the only ACE inhibitors that do not have to be activated in the body to be effective. All the other ACE inhibitors are prodrugs and require activation. Most reach peak serum levels within 1 hour after ingestion. Since most of the activation occurs in the liver, a non-prodrug form is preferable in patients with underlying liver issues.[14]
Adverse Effects
Most Common
- Dry Cough (10% to 20%)
- Dizziness (12% to 19%)
- Hypotension (7% to 11%)
- Increased BUN and creatinine (2% to 11%)
- Syncope (5% to 7%)
- Hyperkalemia (2% to 6%)
Dry Cough: Commonly, patients on ACE inhibitors have reported dry cough between the one week of initiation and up to six months. Some sources cite up to one year after initiation. Discontinuing therapy usually resolves the cough 1 to 4 days after, but it can be prolonged for up to a month.[15] The concern for dry cough with therapy initiation is a decrease in the patient's medication adherence. Additionally, there is an increased propensity to develop bronchospasm in these patients.[16]
ACE metabolizes bradykinin and other local molecules. Inhibiting ACE in the lung increases the concentration of kinins, causing bronchial irritation.[17] After discontinuation of ACE inhibitor therapy, an angiotensin receptor blocker (ARB) can be initiated as an alternate therapy. ARBs have a lower incidence of cough recurrence than reinitiating ACE inhibitor therapy.[18] If cough recurs on ARB therapy, switch to a different drug class entirely.
Angioedema: Angioedema is a rare but potentially life-threatening side effect of ACE inhibitor use. Angioedema is an adverse drug reaction characterized by swelling of the face, lips, and upper airway in an episodic nature. The inflammation creates difficulty in the patient's ability to maintain an airway; therefore, endotracheal intubation is necessary to secure the airway. The mechanism of angioedema is thought to be through an extensive accumulation of bradykinins in select individuals. Bradykinin induces prominent vasodilation and plasma extravasation into the local tissue. Therefore, the primary treatment of ACE inhibitor-induced angioedema is the discontinuation of ACE inhibitor therapy. It is also suggested to avoid ACE inhibitor therapy in individuals with hereditary angioedema or a history of angioedema episodes. Ghouse J. et al. conducted a genome-wide association study on patients who developed ACE inhibitor-related angioedema.[19] The investigators found variants located near the bradykinin receptor B2 gene.
Hyperkalemia: Hyperkalemia from ACE inhibitors directly results from its mechanism of action. The blockade of angiotensin II prevents the downstream secretion of aldosterone. Aldosterone causes reabsorption of sodium and, subsequently, water. Consequently, protons and potassium get secreted into the urine. Without potassium secretion through aldosterone, potassium can easily increase in patients on ACE inhibitors.[20] Co-morbidities that decrease kidney function or medications that cause potassium retention can increase the risk of hyperkalemia.
Increased BUN and creatinine: A slight reduction of glomerular filtration rate (GFR) is common when initiating therapy. Patients with heart failure, chronic kidney disease, and bilateral renal artery stenosis with poor renal perfusion can further reduce GFR, which mandates discontinuation of ACE-Inhibitor therapy.[21]
Hypotension: Hypotension can cause intolerance to therapy leading to discontinuation in a small population of patients, which is more common in patients with increased renin baseline concentrations. Allowing the repletion of fluids and discontinuing diuretic medication before therapy can minimize hypotensive episodes.[22]
Dizziness: Dizziness is a common adverse drug reaction of ACE inhibitor therapy that can be mitigated by adequate volume status and avoiding concomitant diuretic therapy.[4][23]
Post-marketing surveillance: Significant adverse events are reported in less than one percent population in post-marketing surveillance. These adverse drug reactions include anaphylactoid reactions, cardiac arrest, cutaneous pseudolymphoma, eosinophilic pneumonitis, hepatic necrosis, hyponatremia, intestinal angioedema, malignant neoplasm of the lung, pulmonary embolism, systemic lupus erythematosus, Steven-Johnson Syndrome, toxic epidermal necrolysis, and transient ischemic attack.
Khera R. et al. found no association between ACE inhibitors and angiotensin II receptor blockers in COVID-19 hospitalization and mortality.[24]
Contraindications
Absolute Contraindications
- Hypersensitivity reactions- ACE inhibitors are contraindicated in a patient with a history of hypersensitivity to any ACE inhibitor or component of the formulation, angioedema related to previous treatment with ACE inhibitor, idiopathic or hereditary angioedema, or current use of aliskiren in a patient with diabetes mellitus. Also, consider drugs with cross-reactivity with ACE inhibitors.[25][26]
- Pregnancy -The use of drugs that inhibit the renin-angiotensin system correlates with teratogenic effects such as oligohydramnios, decreased fetal renal function, anuria, renal failure, skull hypoplasia, and death. The proposed mechanism behind oligohydramnios is evident at the level of the fetal kidney. The low-pressure hemodynamics of the fetus becomes easily disrupted with a decreased amount of angiotensin II. Fetal renal pressure becomes lower, reducing the ability to maintain GFR, leading to oligohydramnios and anuria.[27]
Relative Contraindications
Use with great caution in the following situations:
- Patients with abnormal renal function: ACE inhibitors can cause elevation of potassium and worsen renal function in patients already on ACE inhibitors. If the patient has an abnormal but stable renal function, close monitoring is required on an ACE inhibitor. If the renal function starts to decline, the clinician should discontinue the ACE inhibitor immediately.
- Patients with aortic valve stenosis: ACE inhibitors reduce afterload and lead to severe hypotension, so these patients should not receive ACE inhibitors.
- Patient with hypovolemia: ACE inhibitors can worsen dehydration and hypovolemia, so these patients should not receive treatment with ACE inhibitors.
Monitoring
- Typical parameters to monitor are renal function, i.e., Blood Urea Nitrogen (BUN), serum creatinine, and electrolytes such as potassium.[28]
- If a patient has collagen vascular disease and/or renal impairment, periodically monitor complete blood count with differential to evaluate kidney erythropoietin production.
- In patients with hypotensive effects within 1 to 3 hours of initial dose or increased dosages or preexisting hepatic impairment, consider baseline hepatic function tests.
- White and red blood cell counts are necessary to evaluate for rare side effects of anemia, neutropenia, agranulocytosis, and thrombocytopenia.[29]
Toxicity
When used at therapeutic doses, the risk of toxicity is rare. Toxicity is more likely when the drug is used in combination with other antihypertensive drugs or at supratherapeutic doses. Captopril is the only ACE inhibitor to penetrate the blood-brain barrier and potentially cause confusion and lethargy.[30] Combining ACE inhibitors with other antihypertensive drugs can increase side effects like hyperkalemia, hypotension, and renal failure. Precaution is required when the patient is given an ACE inhibitor and already receives a potassium-sparing diuretic, NSAIDs, cyclosporine, and anticoagulants.
For the majority of patients, the effects of poisoning are mild, and close observation is required. Hospital admission is indicated when symptoms and signs are more severe. Derranged hemodynamic parameters may require supportive therapy with intravenous fluids and inotropic support.[30]
Enhancing Healthcare Team Outcomes
Clinicians widely use ACE inhibitors in medicine to treat hypertension, heart failure, and patients with chronic kidney disease. While effective, healthcare workers (nurse practitioners, physicians, and pharmacists) who prescribe these agents should be aware of their adverse drug reactions and contraindications. Patients must also be regularly monitored for their renal function and electrolyte concentrations. Healthcare providers should be aware that these agents can produce a chronic dry cough. The clinician should try another class of antihypertensive medication if the patient experiences a dry cough.[10][31][32][33]
Even though ACE inhibitors are among the oldest drug classes available, there is a threat that familiarity can lead to carelessness. That is why, like any other drug, these agents require the oversight and coordination of an interprofessional team. Pharmacists need to verify that dosing is appropriate and check for potential drug interactions.[34] Nurses should take blood pressure at every visit and chart it accurately, so the clinician can determine if dosing or other changes are required. Nurses can monitor for potential signs of pregnancy and promptly inform the clinician if the patient is pregnant, as ACE inhibitors are absolutely contraindicated in pregnancy.[35]
The clinician must remain informed of these findings from the other interprofessional healthcare team members to take corrective action if necessary. All team members must keep meticulous records of their observations and interventions in the patient's medical record. In summary, the interprofessional team approach using evidence-based medicine and patient-centered care correlates with reduced morbidity and mortality in patients receiving ACE inhibitor therapy.[36] [Level 5]
Media
(Click Image to Enlarge)
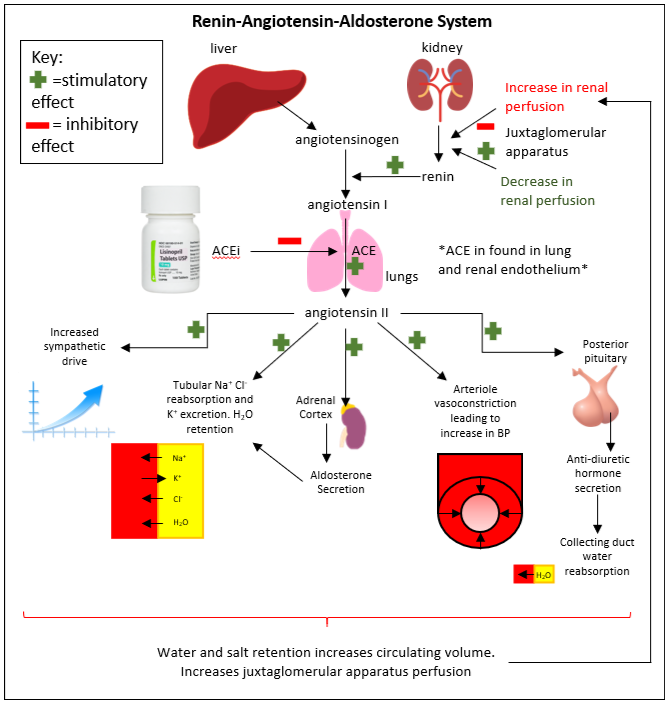
Illustration of Renin-Angiotensin Aldosterone system (RAAS) pathway
Contribute Austin Cusick and Amandeep Goyal, MD
References
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension (Dallas, Tex. : 1979). 2018 Jun:71(6):e13-e115. doi: 10.1161/HYP.0000000000000065. Epub 2017 Nov 13 [PubMed PMID: 29133356]
Level 3 (low-level) evidenceKnežević T, Gellineo L, Jelaković A, Premužić V, Dika Ž, Laganović M, Jelaković B. Treatment of Hypertension Induced Albuminuria. Current pharmaceutical design. 2018:24(37):4404-4412. doi: 10.2174/1381612825666181126170354. Epub [PubMed PMID: 30479206]
Hradec J, Pharmacological therapy for chronic heart failure. Vnitrni lekarstvi. 2018 Fall [PubMed PMID: 30441998]
Leru PM,Anton VF,Bumbea H, Nine year follow-up of a rare case of angioedema due to acquired C1-inhibitor deficiency with late onset and good response to attenuated androgen. Allergy, asthma, and clinical immunology : official journal of the Canadian Society of Allergy and Clinical Immunology. 2018 [PubMed PMID: 30386386]
Level 3 (low-level) evidenceViberti G, Mogensen CE, Groop LC, Pauls JF. Effect of captopril on progression to clinical proteinuria in patients with insulin-dependent diabetes mellitus and microalbuminuria. European Microalbuminuria Captopril Study Group. JAMA. 1994 Jan 26:271(4):275-9 [PubMed PMID: 8295285]
Level 1 (high-level) evidenceLewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. The New England journal of medicine. 1993 Nov 11:329(20):1456-62 [PubMed PMID: 8413456]
Level 1 (high-level) evidenceKrečak I,Morić Perić M,Zekanović I,Holik H,Coha B,Gverić-Krečak V,Lucijanić M, Beneficial effect of ACE inhibitors on kidney function in polycythemia vera. Wiener klinische Wochenschrift. 2021 Aug [PubMed PMID: 33555393]
Yao J, Fan S, Shi X, Gong X, Zhao J, Fan G. Angiotensin-converting enzyme inhibitors versus angiotensin II receptor blockers on insulin sensitivity in hypertensive patients: A meta-analysis of randomized controlled trials. PloS one. 2021:16(7):e0253492. doi: 10.1371/journal.pone.0253492. Epub 2021 Jul 7 [PubMed PMID: 34234365]
Level 1 (high-level) evidenceSalmenkari H, Korpela R, Vapaatalo H. Renin-angiotensin system in intestinal inflammation-Angiotensin inhibitors to treat inflammatory bowel diseases? Basic & clinical pharmacology & toxicology. 2021 Sep:129(3):161-172. doi: 10.1111/bcpt.13624. Epub 2021 Jun 27 [PubMed PMID: 34128327]
Chen YJ,Li LJ,Tang WL,Song JY,Qiu R,Li Q,Xue H,Wright JM, First-line drugs inhibiting the renin angiotensin system versus other first-line antihypertensive drug classes for hypertension. The Cochrane database of systematic reviews. 2018 Nov 14 [PubMed PMID: 30480768]
Level 2 (mid-level) evidencePatel S, Rauf A, Khan H, Abu-Izneid T. Renin-angiotensin-aldosterone (RAAS): The ubiquitous system for homeostasis and pathologies. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie. 2017 Oct:94():317-325. doi: 10.1016/j.biopha.2017.07.091. Epub 2017 Jul 31 [PubMed PMID: 28772209]
Silva P, Brown RS, Epstein FH. Adaptation to potassium. Kidney international. 1977 Jun:11(6):466-75 [PubMed PMID: 327141]
Level 3 (low-level) evidenceYee AH, Burns JD, Wijdicks EF. Cerebral salt wasting: pathophysiology, diagnosis, and treatment. Neurosurgery clinics of North America. 2010 Apr:21(2):339-52. doi: 10.1016/j.nec.2009.10.011. Epub [PubMed PMID: 20380974]
Williams B, Drug discovery in renin-angiotensin system intervention: past and future. Therapeutic advances in cardiovascular disease. 2016 Jun; [PubMed PMID: 27126389]
Level 3 (low-level) evidenceYeo WW,Chadwick IG,Kraskiewicz M,Jackson PR,Ramsay LE, Resolution of ACE inhibitor cough: changes in subjective cough and responses to inhaled capsaicin, intradermal bradykinin and substance-P. British journal of clinical pharmacology. 1995 Nov; [PubMed PMID: 8703645]
Lunde H, Hedner T, Samuelsson O, Lötvall J, Andrén L, Lindholm L, Wiholm BE. Dyspnoea, asthma, and bronchospasm in relation to treatment with angiotensin converting enzyme inhibitors. BMJ (Clinical research ed.). 1994 Jan 1:308(6920):18-21 [PubMed PMID: 8298346]
Malini PL,Strocchi E,Zanardi M,Milani M,Ambrosioni E, Thromboxane antagonism and cough induced by angiotensin-converting-enzyme inhibitor. Lancet (London, England). 1997 Jul 5; [PubMed PMID: 9217714]
Level 1 (high-level) evidenceMatchar DB, McCrory DC, Orlando LA, Patel MR, Patel UD, Patwardhan MB, Powers B, Samsa GP, Gray RN. Systematic review: comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for treating essential hypertension. Annals of internal medicine. 2008 Jan 1:148(1):16-29 [PubMed PMID: 17984484]
Level 1 (high-level) evidenceGhouse J, Ahlberg G, Andreasen L, Banasik K, Brunak S, Schwinn M, Larsen IH, Petersen O, Sørensen E, Ullum H, Rasmussen ER, Eriksson N, Hallberg P, Wadelius M, Bundgaard H, Olesen MS. Association of Variants Near the Bradykinin Receptor B(2) Gene With Angioedema in Patients Taking ACE Inhibitors. Journal of the American College of Cardiology. 2021 Aug 17:78(7):696-709. doi: 10.1016/j.jacc.2021.05.054. Epub [PubMed PMID: 34384552]
Kifor I,Moore TJ,Fallo F,Sperling E,Chiou CY,Menachery A,Williams GH, Potassium-stimulated angiotensin release from superfused adrenal capsules and enzymatically dispersed cells of the zona glomerulosa. Endocrinology. 1991 Aug; [PubMed PMID: 1855477]
Level 3 (low-level) evidenceBakris GL, Weir MR. Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: is this a cause for concern? Archives of internal medicine. 2000 Mar 13:160(5):685-93 [PubMed PMID: 10724055]
Level 1 (high-level) evidenceKostis JB, Shelton B, Gosselin G, Goulet C, Hood WB Jr, Kohn RM, Kubo SH, Schron E, Weiss MB, Willis PW 3rd, Young JB, Probstfield J. Adverse effects of enalapril in the Studies of Left Ventricular Dysfunction (SOLVD). SOLVD Investigators. American heart journal. 1996 Feb:131(2):350-5 [PubMed PMID: 8579032]
Level 1 (high-level) evidenceSachs B,Meier T,Nöthen MM,Stieber C,Stingl J, [Drug-induced angioedema : Focus on bradykinin]. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete. 2018 Apr [PubMed PMID: 29392343]
Khera R, Clark C, Lu Y, Guo Y, Ren S, Truax B, Spatz ES, Murugiah K, Lin Z, Omer SB, Vojta D, Krumholz HM. Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers With the Risk of Hospitalization and Death in Hypertensive Patients With COVID-19. Journal of the American Heart Association. 2021 Jul 6:10(13):e018086. doi: 10.1161/JAHA.120.018086. Epub 2021 Feb 24 [PubMed PMID: 33624516]
Wilkins B, Hullikunte S, Simmonds M, Sasse A, Larsen P, Harding SA. Improving the Prescribing Gap For Guideline Recommended Medications Post Myocardial Infarction. Heart, lung & circulation. 2019 Feb:28(2):257-262. doi: 10.1016/j.hlc.2017.10.025. Epub 2017 Nov 14 [PubMed PMID: 29523466]
Shaikh A. A Practical Approach to Hypertension Management in Diabetes. Diabetes therapy : research, treatment and education of diabetes and related disorders. 2017 Oct:8(5):981-989. doi: 10.1007/s13300-017-0310-3. Epub 2017 Sep 19 [PubMed PMID: 28929319]
Gubler MC,Antignac C, Renin-angiotensin system in kidney development: renal tubular dysgenesis. Kidney international. 2010 Mar; [PubMed PMID: 19924102]
Level 3 (low-level) evidenceRaebel MA,McClure DL,Simon SR,Chan KA,Feldstein A,Andrade SE,Lafata JE,Roblin D,Davis RL,Gunter MJ,Platt R, Laboratory monitoring of potassium and creatinine in ambulatory patients receiving angiotensin converting enzyme inhibitors and angiotensin receptor blockers. Pharmacoepidemiology and drug safety. 2007 Jan; [PubMed PMID: 16470693]
Level 2 (mid-level) evidenceDiBianco R. Adverse reactions with angiotensin converting enzyme (ACE) inhibitors. Medical toxicology. 1986 Mar-Apr:1(2):122-41 [PubMed PMID: 3023783]
Lip GY, Ferner RE. Poisoning with anti-hypertensive drugs: angiotensin converting enzyme inhibitors. Journal of human hypertension. 1995 Sep:9(9):711-5 [PubMed PMID: 8551483]
Alzahrani T,Tiu J,Panjrath G,Solomon A, The effect of angiotensin-converting enzyme inhibitors on clinical outcomes in patients with ischemic cardiomyopathy and midrange ejection fraction: a post hoc subgroup analysis from the PEACE trial. Therapeutic advances in cardiovascular disease. 2018 Nov 15 [PubMed PMID: 30442080]
Level 2 (mid-level) evidenceBrar S, Ye F, James MT, Hemmelgarn B, Klarenbach S, Pannu N, Interdisciplinary Chronic Disease Collaboration. Association of Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use With Outcomes After Acute Kidney Injury. JAMA internal medicine. 2018 Dec 1:178(12):1681-1690. doi: 10.1001/jamainternmed.2018.4749. Epub [PubMed PMID: 30422153]
Saglimbene V,Palmer SC,Ruospo M,Natale P,Maione A,Nicolucci A,Vecchio M,Tognoni G,Craig JC,Pellegrini F,Lucisano G,Hegbrant J,Ariano R,Lamacchia O,Sasso A,Morano S,Filardi T,De Cosmo S,Pugliese G,Procaccini DA,Gesualdo L,Palasciano G,Johnson DW,Tonelli M,Strippoli GFM, The Long-Term Impact of Renin-Angiotensin System (RAS) Inhibition on Cardiorenal Outcomes (LIRICO): A Randomized, Controlled Trial. Journal of the American Society of Nephrology : JASN. 2018 Nov 12 [PubMed PMID: 30420421]
Level 1 (high-level) evidenceMansur JM, Medication Safety Systems and the Important Role of Pharmacists. Drugs [PubMed PMID: 26932714]
Simonetti V,Comparcini D,Tomietto M,Pavone D,Flacco ME,Cicolini G, Effectiveness of a family nurse-led programme on accuracy of blood pressure self-measurement: A randomised controlled trial. Journal of clinical nursing. 2021 Apr 19; [PubMed PMID: 33872417]
Level 1 (high-level) evidenceMao CT, Liu MH, Hsu KH, Fu TC, Wang JS, Huang YY, Yang NI, Wang CH. Effect of multidisciplinary disease management for hospitalized heart failure under a national health insurance programme. Journal of cardiovascular medicine (Hagerstown, Md.). 2015 Sep:16(9):616-24. doi: 10.2459/JCM.0000000000000089. Epub [PubMed PMID: 25105284]
Level 1 (high-level) evidence