
Introduction
Hypoalphalipoproteinemia (HA) is classified as a low high-density lipoprotein cholesterol (HDL-C) level. Contemporary literature has also reported HA as HDL levels below the 10th percentile for patients of the same age and gender without any other lipoprotein abnormalities.[1] The cutoff provided by The US National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) was < 40mg/dL.[2]
Metabolic syndrome constitutes the combination of abnormalities in HDL, triglycerides, abdominal waist circumference, blood pressure, and glucose levels. The ATP III criteria designated for HDL cholesterol levels that contribute to metabolic syndrome are sex-specific. For example, in men, the cutoff is <40mg/dL, but for women, the high-risk HDL cholesterol level is <50 mg/dL.
Familial hypoalphalipoproteinemia has an autosomal dominant mode of inheritance. As a result of low levels of alpha-lipoproteins, patients have a higher prevalence of premature coronary heart disease and stroke.[3][4] Low HDL cholesterol levels are among the most significant risk factors for developing coronary artery disease. In addition, coronary artery disease may lead to more harmful sequelae, such as stroke or myocardial infarction.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
HA includes multiple different conditions that may cause HDL levels to be reduced. However, the causes of decreased HDL levels are primarily hereditary.[5]
Some inherited causes of decreased HDL include:
- Tangier Disease[6]
- Familial hypoalphalipoproteinemia
- Caused by a mutation in the Apolipoprotein A-1 Gene[3]
- Familial combined hypolipidemia[7]
- Elevated Cholesteryl ester transfer protein activity[8]
- Lipoprotein lipase deficiency[9]
- Familial lecithin-cholesterol acyltransferase deficiency[10]
Secondary causes of decreased HDL levels include:
Epidemiology
A National Center for Health Statistics (NCHS) data brief reported the prevalence of low HDL cholesterol among U.S. adults aged ≥20. This report defined low HDL cholesterol levels as serum HDL levels less than 40 mg/dL. The report showed the differences in HDL levels in populations based on if adults fulfilled the 2008 physical activity guidelines from the U.S. Department of Health and Human Services.
Fulfilling physical activity guidelines was described as engaging in either ≥150 minutes per week of intermediate-intensity aerobic activity, ≥75 minutes per week of high-intensity aerobic exercise, or an equivalent combination. The prevalence of low HDL cholesterol was higher in adults who did not fulfill the physical activity guidelines (21.0%) than in those who did (17.7%).
The prevalence of low HDL cholesterol levels in all U.S. adults was 19%. For those who did not meet the physical activity guidelines, the prevalence of low HDL was 35.4% for men and 11.8% for women. For those who did meet the guidelines, the prevalence of low HDL was 25.0% for men and 9.1% for women.
The report showed substantial differences by race and ethnicity for those who met the physical activity guidelines. The prevalence was 20.7% of Hispanic adults, 18.1% of White adults, 14.4% of Asian adults, and 12.4% of Black adults.[18]
Pathophysiology
High-density lipoproteins are shown to be atheroprotective and exhibit various antiatherogenic properties. These include inhibition of inflammation, oxidation, and apoptosis. One of the most integral antiatherogenic functions is the capability to promote reverse cholesterol transport (RCT).[19]
RCT is a sequence of reactions in which HDL particles facilitate the release of lipids from the subendothelial space and intima and deliver them to the liver. In contrast, apoB-containing lipoproteins (LDL, VLDL, IDL) promote atherosclerosis by driving cholesterol and phospholipids into the subendothelial space.[19] High-density lipoproteins are also responsible for the transport of many different molecules. For example, they transport enzymes, apoproteins, globulins, acute phase reactants, microRNAs, and complement components.[20]
In some circumstances, the protein cargo carried by HDL can be converted from an atheroprotective to a pro-oxidative and pro-inflammatory state. This has been observed in patients with sepsis, CKD, chronic inflammatory conditions, recent acute coronary events, and diabetes mellitus. During these occasions, the apoprotein and enzyme components of HDL may be substituted by acute phase reactants (fibrinogen, serum amyloid A), which disable the ability of HDL to partake in reverse cholesterol transport or promote other antiatherogenic processes.[21]
History and Physical
Patients with low serum HDL cholesterol can significantly differ in their clinical presentation, depending on the underlying cause.
Patients may have an underlying history of:
- Premature atherosclerosis
- Coronary heart disease
- Peripheral Vascular disease
- Stroke or TIA
- Carotid stenosis
Patients may also have a history of secondary causes of low HDL cholesterol, including the following:
- Tobacco use
- Sedentary lifestyle
- Renal disease
- Medications (beta blockers, thiazides, benzodiazepines)
Patients with HDL deficiency, but normal levels of LDL-C and triglycerides, can present with xanthomas and premature coronary heart disease. Patients with premature coronary disease may show signs of congestive heart failure (jugular venous distention, crackles at lung bases on auscultation, hepatomegaly, pitting edema) or arrhythmias (such as atrial fibrillation)
Patients with familial lecithin: cholesterol acyltransferase (LCAT) deficiency may present with corneal opacities, anemia, proteinuria, and kidney failure.[22] The corneal opacification reported in familial LCAT deficiency presents as multiple, small, gray-colored dots in the entire corneal stroma. Vision is usually not affected. Some reports of premature atherosclerosis in the carotid, aortic, and femoral arteries have been reported, but early coronary heart disease is not typically seen.[23]
Familial partial LCAT deficiency (fish-eye disease), a variant of LCAT deficiency, was first reported in 1975 in a 61-year-old woman with marked corneal opacifications. The patient's eye resembled "boiled fish." Consequently, this condition was called fish-eye disease. The same corneal opacifications were also seen in her sisters and father.[23]
Tangier disease is caused by a mutation in the ATP-binding cassette transporter A1 (ABCA1) gene. Patients with Tangier disease have evidence of orange mucosa in their oral pharynx. The orange color is secondary to cholesterol-laden macrophages. Other significant clinical findings in Tangier disease are corneal opacification, hepatosplenomegaly, and peripheral neuropathy. In some cases, premature coronary heart disease (CHD) has been reported.[24] ApoA-1 variants with amino acid mutations have been associated with amyloidosis.
Evaluation
Laboratory workup of hypoalphalipoproteinemia includes a comprehensive metabolic profile, a plasma fasting lipid profile, and a plasma ApoA-I level. Secondary causes of low HDL levels must also be considered and ruled out before diagnosing HA. Low HDL levels can be seen in patients with marked hypertriglyceridemia, monoclonal gammopathy, or severe liver failure. Low HDL levels can also be seen in patients taking anabolic steroids, beta-blockers, or benzodiazepines.
Secondary etiologies causing a decrease in HDL can be ruled out with a complete medical history and a metabolic profile, including protein electrophoresis, a fasting lipid profile, and a hepatic panel. In the absence of any secondary causes of low HDL levels, the following step in the workup is to measure plasma ApoA-I levels using immunoassay to evaluate for hereditary causes of low HDL.
A review of the medication list of a patient presenting with low HDL levels will help rule out secondary causes. For example, beta-blockers may increase triglyceride and VLDL levels while causing a decrease in HDL levels.[25]
Lipid abnormalities in disease-specific causes of low HDL-cholesterol:
ApoA-I deficiency: normal triglycerides and LDL-C, HDL-C <5mg/dL, and undetectable ApoA-I levels. Tangier disease: increased triglycerides, decreased LDL-C, HDL-C <5 mg/dL, and ApoA-I present (<10 mg/dL) Partial LCAT deficiency (fish-eye disease): increased triglycerides, LDL-C levels about 50% of normal, HDL-C about 10% of normal, and ApoA-I levels around 20% of normal. LCAT deficiency: increased triglycerides, decreased LDL-C, HDL-C <5 mg/dL, and ApoA-I levels <40 mg/dL.[24]
Treatment / Management
When treating patients with hypoalphalipoproteinemia, the objective is to reduce cardiovascular risk and increase HDL cholesterol levels.
Statins
- Atorvastatin
- Fluvastatin
- Lovastatin
- Pravastatin
- Rosuvastatin
- Simvastatin
- Pitavastatin
Statins have been shown to increase HDL-C levels by up to 15%.[26] The primary mechanism of statins is to inhibit 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase (HMG-CoA reductase), the rate-limiting enzyme in the mevalonate pathway. The mevalonate pathway is the metabolic pathway responsible for cholesterol synthesis. Inhibition of HMG-CoA reductase leads to decreased LDL cholesterol production. Statins also increase HDL and ApoA-I levels by inhibiting the GGpp/Rho signal transduction pathway, which leads to activation of PPAR-alpha and increased hepatocyte expression of ApoA-I and ApoA-II, resulting in increased production of HDL.[27] (B3)
Statins also reduce triglycerides transferred into HDL particles by cholesterol ester transfer protein (CETP), which leads to a reduction in HDL catabolism by hepatic lipase.[26] Patients with average levels of triglycerides and LDL-C with below-average HDL-C may acquire substantial clinical benefits from statin use.
The AFCAPS/TexCAPS study enrolled 5608 men and 997 women with average triglycerides and LCL-C with below-average HDL-C. Participants received either Lovastatin or a placebo in addition to a low-saturated fat, low-cholesterol diet. Participants who received Lovastatin increased HDL-C by an average of 6%. Participants with a baseline HDL-C >45 mg/dL experienced a 15% relative risk reduction for cardiovascular events, while the risk reduction for participants with a baseline HDL-C <45 mg/dL was 45%.[28] (B2)
Fibric Acid Derivatives (Fibrates)
- Gemfibrozil
- Fenofibrate
- Fenofibric Acid
Fibrates are synthetic PPAR-alpha agonists that influence HDL metabolism. On average, fibrates raise serum HDL-C by approximately 10%.[29](A1)
A study with 2531 male participants with CHD, HDL-C <40 mg/dL, and LDL-C <140 mg/dL compared gemfibrozil therapy (1200mg/day) with a placebo. After one year, HDL-C increased by 6%, and triglycerides decreased by 31%. There was a 24% reduction in the combined outcome of death from stroke, CHD, and nonfatal myocardial infarction. Gemfibrozil therapy significantly decreased the risk of major CV events in participants with CHD whose primary lipid irregularity was a low HDL-C.[30](A1)
Nicotinic Acid (Niacin)
Niacin binds to receptors on macrophages and adipocytes (mouse PUMA-G and human HM74 receptors).[31] Triglyceride lipase is inhibited in the adipose tissue when niacin binds to this receptor. This leads to decreased fatty acids delivered to the liver, which decreases serum triglyceride levels and hepatic VLDL secretion. HDL cholesterol levels will rise because of reduced triglyceride enrichment by CETP. While niacin can significantly raise HDL-C levels in patients with no other lipid irregularity, there is little data indicating that this effect has a cardiovascular benefit.[32] Niacin also inhibits hepatocyte diacylglycerol acyltransferase-2, an essential enzyme for triglyceride synthesis.[33](B3)
In the AIM-HIGH trial, 3414 patients taking statins with well-controlled LDL and low HDL-C were assigned to receive either niacin or a placebo. Despite a significant increase in HDL-C levels in statin-treated patients with the addition of niacin, no clinical benefit was found.[34] (A1)
Lifestyle Changes
Smoking cessation may yield an increase in HDL levels in thirty days.[35] Weight loss, either through dieting or exercise, causes a favorable change in plasma lipoprotein levels.[36] The combination of frequent exercise and diet will improve plasma lipoprotein levels even more.[37](A1)
Differential Diagnosis
It is essential to rule out secondary causes of low HDL cholesterol levels before looking for a genetic syndrome. A thorough medical history will help rule out secondary causes such as inflammatory conditions, monoclonal gammopathies, or medication use (beta-blockers, benzodiazepines, testosterone replacement therapy). A complete lipid panel can distinguish isolated HDL deficiency from other hereditary lipid disorders, such as familial combined hyperlipidemia. Genetic causes of HDL deficiency, such as Tangier disease, ApoA-I deficiency, and LCAT deficiency, will have decreased HDL levels with normal or reduced LDL levels. In contrast, familial combined hyperlipidemia will have decreased HDL with increased LDL levels.[24]
Prognosis
The meta-analysis of four prospective studies (FHS, LRCF CPPT, MRFIT) concluded that CHD risk is inversely related to HDL-C levels. The FHS, CPPT, and MRFIT studies demonstrated that for each 1 mg/dL increase in HDL, there was a 3% decrease in CHD risk for women and a 2% decrease for men.
The Lipid Research Clinics Prevalence Mortality Follow-up Study (LRCF) documented only fatal outcomes. A 1-mg/dL increase in HDL cholesterol decreased cardiovascular disease mortality rates by 3.7% in men and 4.7% in women.[38]
Complications
Many studies have shown that low HDL levels are inversely related to coronary heart disease (CHD). A study published in 1977, titled The Cooperative Lipoprotein Phenotyping Study, included 6859 men and women. It showed an inverse relationship between HDL-C levels and CHD prevalence, despite adjusting for LDL-C and triglyceride levels.[39] An inverse relationship between HDL-C and CHD risk was observed in a 2-year case-control study of 6595 men aged 20-49 living in Tromsø, Norway.[40]
The Münster Heart Study (PROCAM) concluded that participants with a serum HDL cholesterol level <35 mg/dL had a 3-fold greater risk for developing coronary artery disease compared to participants who had HDL cholesterol levels >35 mg/dL.[41] A meta-analysis among Asians suggested a strong association between low HDL cholesterol levels and coronary artery disease. Compared to participants with normal lipid levels, isolated low HDL cholesterol increases the risk for cardiovascular events by 67%.[41] The Emerging Risk Factors Collaboration published a study in 2009 comprised of 302,340 subjects. It demonstrated that the inverse relationship between HDL cholesterol and cardiovascular risk is still significant, even after adjusting for non-HDL cholesterol.[42]
The Framingham Heart Study described the higher cardiovascular disease risk related to a low HDL cholesterol level, regardless of LDL cholesterol levels. In all tertiles of LDL cholesterol levels of participants, the relative risk of a cardiac event increased as HDL cholesterol levels decreased.[43] An 8-year follow-up in the Framingham Heart study demonstrated that participants at the 80th percentile of HDL cholesterol had half the risk of developing coronary heart disease compared to participants in the 20th percentile of HDL cholesterol.[44]
A meta-analysis of four prospective American studies (Framingham Heart Study, Lipid Research Clinics Prevalence Mortality Follow-up Study, Coronary Primary Prevention Trial, Multiple Risk Factor Intervention Trial) was published by Gordon et al. in 1989. An increase of 1 mg/dL of HDL cholesterol was associated with a significant coronary heart disease risk decrease of 2% in men and 3% in women.[38]
A study published in April 2022 by Dong et al. showed that many gene loci identified with low HDL levels are associated with various types of cancer.[45]
Genes with the highest prevalence of damaging variants were:
- ABCA1 (Chronic myelogenous leukemia)[46]
- Stab1 (Bladder cancer and Acute Myelogenous Leukemia)[47]
- OSBPL1A
- CPS1 (Hepatocellular carcinoma)[48]
- CD36 (Ovarian cancer)[49]
- LRP1[50]
- ABCA8 (Hepatocellular carcinoma)[51]
- GOT2
- AMPD3 (Gastrointestinal stromal tumors and lung cancers)[52][53]
- WWOX
- IRS1 (Medulloblastoma, breast cancer, and osteosarcoma)[54]
A large-population study by Pedersen et al. revealed substantial increases in tumor growth associated with low HDL levels. The increased risk was most documented in hematological and nervous system cancers. It was also seen to a minor extent for breast and lung cancer.[55]
Deterrence and Patient Education
Genetic causes of hypoalphalipoproteinemia are not preventable. However, genetic screening can be done in some cases.
Hypoalphalipoproteinemia from secondary causes can be treated by managing the primary source. Smoking cessation, proper diet, and regular exercise will help increase HDL levels.[36]
Enhancing Healthcare Team Outcomes
The management of hypoalphalipoproteinemia requires care coordination and management from the interprofessional team consisting of a primary care clinician, cardiologist, nurse, pharmacist, and mid-level providers. Hypoalphalipoproteinemia is typically discovered during routine visits by a primary care provider in an outpatient setting. The diagnostics involve regular blood work, mainly the lipid panel, which shows reduced levels of high-density lipoprotein cholesterol. Per the United States Preventive Services Task Force (USPSTF), lipid panel screening should be done at baseline for females between the ages of 20-45 and males between the ages of 20 to 35. In addition, routine follow-up visits should be scheduled for patients at risk for HA, other lipid disorders, and coronary artery disease.
The primary care provider should discuss methods on how to raise HDL levels. Counseling should be provided on preventative strategies for risk factors, such as smoking prevention, alcohol reduction, dietary modifications, and increased physical activity and exercise. Patients who smoke may be referred to licensed therapists for behavior modification therapy. Licensed dieticians can help with diet and weight loss strategies. Patients with severe cardiovascular events should be directed to cardiovascular rehabilitation and routinely follow up with a cardiologist.
Patients should initially be guided on lifestyle preventative changes before initiating pharmacological therapy, depending on their lipid panel results and underlying history of comorbidities. Management with statins should be initiated promptly as they can be life-saving and significantly decrease the risk of cardiovascular disease.[56] [Level 1]
In most cases, care in the inpatient setting is not required unless treating severe sequelae of HA such as a myocardial infarction or stroke. Therefore, most patients with hypoalphalipoproteinemia can be managed in an outpatient setting. Patients with HA may have underlying comorbidities such as hypertension, hyperlipidemia, diabetes mellitus, and obesity, which may serve as risk factors for complications such as myocardial infarction or stroke. In such cases, input from subspecialists such as cardiology may be warranted.
Interprofessional care coordination and communication among the healthcare team will lead to timely management of patients with HA and can decrease its associated adverse events and complications such as CAD, MI, and stroke and further improve patient outcomes.
Media
(Click Image to Enlarge)
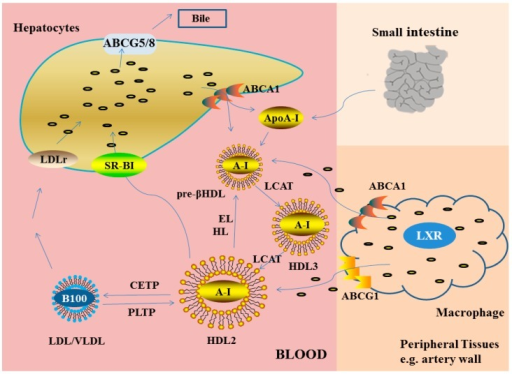
Reverse cholesterol transport see Text Pathophysiology section for explanation
Contributed from the National Institute of Health; ijms-16-17245-f002 Sourced from: https://openi.nlm.nih.gov
(Click Image to Enlarge)
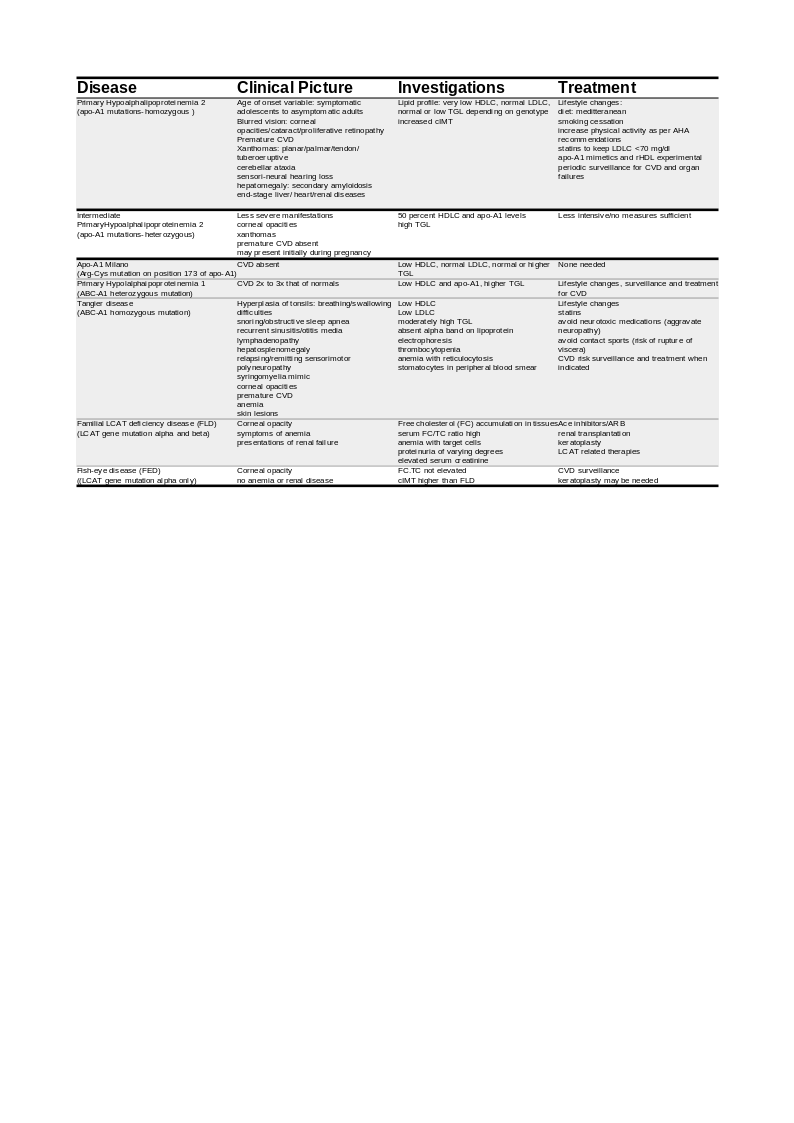
Table showing Clinical Characteristics and Management Guidelines for Primary Hypoalphalipoproteinemia
Contributed by Venkatraman Rajkumar, MD
References
Genest J Jr, Bard JM, Fruchart JC, Ordovas JM, Schaefer EJ. Familial hypoalphalipoproteinemia in premature coronary artery disease. Arteriosclerosis and thrombosis : a journal of vascular biology. 1993 Dec:13(12):1728-37 [PubMed PMID: 8241092]
Level 3 (low-level) evidenceExpert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001 May 16:285(19):2486-97 [PubMed PMID: 11368702]
Level 1 (high-level) evidenceVergani C, Bettale G. Familial hypo-alpha-lipoproteinemia. Clinica chimica acta; international journal of clinical chemistry. 1981 Jul 18:114(1):45-52 [PubMed PMID: 7249374]
Level 3 (low-level) evidenceGlueck CJ, Daniels SR, Bates S, Benton C, Tracy T, Third JL. Pediatric victims of unexplained stroke and their families: familial lipid and lipoprotein abnormalities. Pediatrics. 1982 Mar:69(3):308-16 [PubMed PMID: 6977760]
Level 2 (mid-level) evidenceCohen JC, Kiss RS, Pertsemlidis A, Marcel YL, McPherson R, Hobbs HH. Multiple rare alleles contribute to low plasma levels of HDL cholesterol. Science (New York, N.Y.). 2004 Aug 6:305(5685):869-72 [PubMed PMID: 15297675]
Brooks-Wilson A, Marcil M, Clee SM, Zhang LH, Roomp K, van Dam M, Yu L, Brewer C, Collins JA, Molhuizen HO, Loubser O, Ouelette BF, Fichter K, Ashbourne-Excoffon KJ, Sensen CW, Scherer S, Mott S, Denis M, Martindale D, Frohlich J, Morgan K, Koop B, Pimstone S, Kastelein JJ, Genest J Jr, Hayden MR. Mutations in ABC1 in Tangier disease and familial high-density lipoprotein deficiency. Nature genetics. 1999 Aug:22(4):336-45 [PubMed PMID: 10431236]
Soro A, Jauhiainen M, Ehnholm C, Taskinen MR. Determinants of low HDL levels in familial combined hyperlipidemia. Journal of lipid research. 2003 Aug:44(8):1536-44 [PubMed PMID: 12777471]
Kuivenhoven JA, Jukema JW, Zwinderman AH, de Knijff P, McPherson R, Bruschke AV, Lie KI, Kastelein JJ. The role of a common variant of the cholesteryl ester transfer protein gene in the progression of coronary atherosclerosis. The Regression Growth Evaluation Statin Study Group. The New England journal of medicine. 1998 Jan 8:338(2):86-93 [PubMed PMID: 9420339]
Level 1 (high-level) evidenceNordestgaard BG, Abildgaard S, Wittrup HH, Steffensen R, Jensen G, Tybjaerg-Hansen A. Heterozygous lipoprotein lipase deficiency: frequency in the general population, effect on plasma lipid levels, and risk of ischemic heart disease. Circulation. 1997 Sep 16:96(6):1737-44 [PubMed PMID: 9323055]
Zannis VI, Chroni A, Krieger M. Role of apoA-I, ABCA1, LCAT, and SR-BI in the biogenesis of HDL. Journal of molecular medicine (Berlin, Germany). 2006 Apr:84(4):276-94 [PubMed PMID: 16501936]
Level 3 (low-level) evidencevan Leeuwen HJ, Heezius EC, Dallinga GM, van Strijp JA, Verhoef J, van Kessel KP. Lipoprotein metabolism in patients with severe sepsis. Critical care medicine. 2003 May:31(5):1359-66 [PubMed PMID: 12771603]
McMahon M, Grossman J, FitzGerald J, Dahlin-Lee E, Wallace DJ, Thong BY, Badsha H, Kalunian K, Charles C, Navab M, Fogelman AM, Hahn BH. Proinflammatory high-density lipoprotein as a biomarker for atherosclerosis in patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis and rheumatism. 2006 Aug:54(8):2541-9 [PubMed PMID: 16868975]
van Leuven SI, Hezemans R, Levels JH, Snoek S, Stokkers PC, Hovingh GK, Kastelein JJ, Stroes ES, de Groot E, Hommes DW. Enhanced atherogenesis and altered high density lipoprotein in patients with Crohn's disease. Journal of lipid research. 2007 Dec:48(12):2640-6 [PubMed PMID: 17890779]
Murali MR, Kratz A, Finberg KE. Case records of the Massachusetts General Hospital. Case 40-2006. A 64-year-old man with anemia and a low level of HDL cholesterol. The New England journal of medicine. 2006 Dec 28:355(26):2772-9 [PubMed PMID: 17192544]
Level 3 (low-level) evidenceKasiske BL, Ma JZ, Kalil RS, Louis TA. Effects of antihypertensive therapy on serum lipids. Annals of internal medicine. 1995 Jan 15:122(2):133-41 [PubMed PMID: 7992988]
Level 1 (high-level) evidenceWallace RB, Hunninghake DB, Reiland S, Barrett-Connor E, Mackenthun A, Hoover J, Wahl P. Alterations of plasma high-density lipoprotein cholesterol levels associated with consumption of selected medications. The Lipid Research Clinics Program Prevalence Study. Circulation. 1980 Nov:62(4 Pt 2):IV77-82 [PubMed PMID: 6106533]
Bagatell CJ, Heiman JR, Matsumoto AM, Rivier JE, Bremner WJ. Metabolic and behavioral effects of high-dose, exogenous testosterone in healthy men. The Journal of clinical endocrinology and metabolism. 1994 Aug:79(2):561-7 [PubMed PMID: 8045977]
Zwald ML, Akinbami LJ, Fakhouri TH, Fryar CD. Prevalence of Low High-density Lipoprotein Cholesterol Among Adults, by Physical Activity: United States, 2011-2014. NCHS data brief. 2017 Mar:(276):1-8 [PubMed PMID: 28282020]
Toth PP. Reverse cholesterol transport: high-density lipoprotein's magnificent mile. Current atherosclerosis reports. 2003 Sep:5(5):386-93 [PubMed PMID: 12911849]
Vaisar T, Pennathur S, Green PS, Gharib SA, Hoofnagle AN, Cheung MC, Byun J, Vuletic S, Kassim S, Singh P, Chea H, Knopp RH, Brunzell J, Geary R, Chait A, Zhao XQ, Elkon K, Marcovina S, Ridker P, Oram JF, Heinecke JW. Shotgun proteomics implicates protease inhibition and complement activation in the antiinflammatory properties of HDL. The Journal of clinical investigation. 2007 Mar:117(3):746-56 [PubMed PMID: 17332893]
Ansell BJ, Fonarow GC, Fogelman AM. High-density lipoprotein: is it always atheroprotective? Current atherosclerosis reports. 2006 Sep:8(5):405-11 [PubMed PMID: 16901411]
Schaefer EJ, Santos RD, Asztalos BF. Marked HDL deficiency and premature coronary heart disease. Current opinion in lipidology. 2010 Aug:21(4):289-97. doi: 10.1097/MOL.0b013e32833c1ef6. Epub [PubMed PMID: 20616715]
Level 3 (low-level) evidenceSchaefer EJ. Clinical, biochemical, and genetic features in familial disorders of high density lipoprotein deficiency. Arteriosclerosis (Dallas, Tex.). 1984 Jul-Aug:4(4):303-22 [PubMed PMID: 6431953]
Santos RD, Asztalos BF, Martinez LR, Miname MH, Polisecki E, Schaefer EJ. Clinical presentation, laboratory values, and coronary heart disease risk in marked high-density lipoprotein-deficiency states. Journal of clinical lipidology. 2008 Aug:2(4):237-47. doi: 10.1016/j.jacl.2008.06.002. Epub 2008 Jun 13 [PubMed PMID: 21291740]
Wolinsky H. The effects of beta-adrenergic blocking agents on blood lipid levels. Clinical cardiology. 1987 Oct:10(10):561-6 [PubMed PMID: 2889552]
Schaefer EJ, Asztalos BF. The effects of statins on high-density lipoproteins. Current atherosclerosis reports. 2006 Jan:8(1):41-9 [PubMed PMID: 16455013]
Martin G, Duez H, Blanquart C, Berezowski V, Poulain P, Fruchart JC, Najib-Fruchart J, Glineur C, Staels B. Statin-induced inhibition of the Rho-signaling pathway activates PPARalpha and induces HDL apoA-I. The Journal of clinical investigation. 2001 Jun:107(11):1423-32 [PubMed PMID: 11390424]
Level 3 (low-level) evidenceGotto AM Jr, Whitney E, Stein EA, Shapiro DR, Clearfield M, Weis S, Jou JY, Langendörfer A, Beere PA, Watson DJ, Downs JR, de Cani JS. Relation between baseline and on-treatment lipid parameters and first acute major coronary events in the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS). Circulation. 2000 Feb 8:101(5):477-84 [PubMed PMID: 10662743]
Level 2 (mid-level) evidenceBirjmohun RS, Hutten BA, Kastelein JJ, Stroes ES. Efficacy and safety of high-density lipoprotein cholesterol-increasing compounds: a meta-analysis of randomized controlled trials. Journal of the American College of Cardiology. 2005 Jan 18:45(2):185-97 [PubMed PMID: 15653014]
Level 1 (high-level) evidenceRubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. The New England journal of medicine. 1999 Aug 5:341(6):410-8 [PubMed PMID: 10438259]
Level 1 (high-level) evidenceTunaru S, Kero J, Schaub A, Wufka C, Blaukat A, Pfeffer K, Offermanns S. PUMA-G and HM74 are receptors for nicotinic acid and mediate its anti-lipolytic effect. Nature medicine. 2003 Mar:9(3):352-5 [PubMed PMID: 12563315]
Level 3 (low-level) evidenceLavie CJ, Mailander L, Milani RV. Marked benefit with sustained-release niacin therapy in patients with "isolated" very low levels of high-density lipoprotein cholesterol and coronary artery disease. The American journal of cardiology. 1992 Apr 15:69(12):1083-5 [PubMed PMID: 1561983]
Kamanna VS, Kashyap ML. Mechanism of action of niacin. The American journal of cardiology. 2008 Apr 17:101(8A):20B-26B. doi: 10.1016/j.amjcard.2008.02.029. Epub [PubMed PMID: 18375237]
AIM-HIGH Investigators, Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, Koprowicz K, McBride R, Teo K, Weintraub W. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. The New England journal of medicine. 2011 Dec 15:365(24):2255-67. doi: 10.1056/NEJMoa1107579. Epub 2011 Nov 15 [PubMed PMID: 22085343]
Level 1 (high-level) evidenceMoffatt RJ, Effects of cessation of smoking on serum lipids and high density lipoprotein-cholesterol. Atherosclerosis. 1988 Nov; [PubMed PMID: 3214483]
Wood PD, Stefanick ML, Dreon DM, Frey-Hewitt B, Garay SC, Williams PT, Superko HR, Fortmann SP, Albers JJ, Vranizan KM. Changes in plasma lipids and lipoproteins in overweight men during weight loss through dieting as compared with exercise. The New England journal of medicine. 1988 Nov 3:319(18):1173-9 [PubMed PMID: 3173455]
Level 1 (high-level) evidenceWood PD, Stefanick ML, Williams PT, Haskell WL. The effects on plasma lipoproteins of a prudent weight-reducing diet, with or without exercise, in overweight men and women. The New England journal of medicine. 1991 Aug 15:325(7):461-6 [PubMed PMID: 1852180]
Level 1 (high-level) evidenceGordon DJ, Probstfield JL, Garrison RJ, Neaton JD, Castelli WP, Knoke JD, Jacobs DR Jr, Bangdiwala S, Tyroler HA. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989 Jan:79(1):8-15 [PubMed PMID: 2642759]
Level 2 (mid-level) evidenceCastelli WP, Doyle JT, Gordon T, Hames CG, Hjortland MC, Hulley SB, Kagan A, Zukel WJ. HDL cholesterol and other lipids in coronary heart disease. The cooperative lipoprotein phenotyping study. Circulation. 1977 May:55(5):767-72 [PubMed PMID: 191215]
Miller NE, Thelle DS, Forde OH, Mjos OD. The Tromsø heart-study. High-density lipoprotein and coronary heart-disease: a prospective case-control study. Lancet (London, England). 1977 May 7:1(8019):965-8 [PubMed PMID: 67464]
Level 2 (mid-level) evidenceAssmann G, Cullen P, Schulte H. The Münster Heart Study (PROCAM). Results of follow-up at 8 years. European heart journal. 1998 Feb:19 Suppl A():A2-11 [PubMed PMID: 9519336]
Emerging Risk Factors Collaboration, Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, Wood AM, Lewington S, Sattar N, Packard CJ, Collins R, Thompson SG, Danesh J. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009 Nov 11:302(18):1993-2000. doi: 10.1001/jama.2009.1619. Epub [PubMed PMID: 19903920]
Castelli WP. Cholesterol and lipids in the risk of coronary artery disease--the Framingham Heart Study. The Canadian journal of cardiology. 1988 Jul:4 Suppl A():5A-10A [PubMed PMID: 3179802]
Castelli WP, Garrison RJ, Wilson PW, Abbott RD, Kalousdian S, Kannel WB. Incidence of coronary heart disease and lipoprotein cholesterol levels. The Framingham Study. JAMA. 1986 Nov 28:256(20):2835-8 [PubMed PMID: 3773200]
Dong W, Wong KHY, Liu Y, Levy-Sakin M, Hung WC, Li M, Li B, Jin SC, Choi J, Lopez-Giraldez F, Vaka D, Poon A, Chu C, Lao R, Balamir M, Movsesyan I, Malloy MJ, Zhao H, Kwok PY, Kane JP, Lifton RP, Pullinger CR. Whole-exome sequencing reveals damaging gene variants associated with hypoalphalipoproteinemia. Journal of lipid research. 2022 Jun:63(6):100209. doi: 10.1016/j.jlr.2022.100209. Epub 2022 Apr 20 [PubMed PMID: 35460704]
Viaud M, Abdel-Wahab O, Gall J, Ivanov S, Guinamard R, Sore S, Merlin J, Ayrault M, Guilbaud E, Jacquel A, Auberger P, Wang N, Levine RL, Tall AR, Yvan-Charvet L. ABCA1 Exerts Tumor-Suppressor Function in Myeloproliferative Neoplasms. Cell reports. 2020 Mar 10:30(10):3397-3410.e5. doi: 10.1016/j.celrep.2020.02.056. Epub [PubMed PMID: 32160545]
Hollmén M, Figueiredo CR, Jalkanen S. New tools to prevent cancer growth and spread: a 'Clever' approach. British journal of cancer. 2020 Aug:123(4):501-509. doi: 10.1038/s41416-020-0953-0. Epub 2020 Jun 29 [PubMed PMID: 32595212]
Cancer Genome Atlas Research Network. Electronic address: wheeler@bcm.edu, Cancer Genome Atlas Research Network. Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell. 2017 Jun 15:169(7):1327-1341.e23. doi: 10.1016/j.cell.2017.05.046. Epub [PubMed PMID: 28622513]
Ladanyi A, Mukherjee A, Kenny HA, Johnson A, Mitra AK, Sundaresan S, Nieman KM, Pascual G, Benitah SA, Montag A, Yamada SD, Abumrad NA, Lengyel E. Adipocyte-induced CD36 expression drives ovarian cancer progression and metastasis. Oncogene. 2018 Apr:37(17):2285-2301. doi: 10.1038/s41388-017-0093-z. Epub 2018 Feb 5 [PubMed PMID: 29398710]
Langlois B, Perrot G, Schneider C, Henriet P, Emonard H, Martiny L, Dedieu S. LRP-1 promotes cancer cell invasion by supporting ERK and inhibiting JNK signaling pathways. PloS one. 2010 Jul 14:5(7):e11584. doi: 10.1371/journal.pone.0011584. Epub 2010 Jul 14 [PubMed PMID: 20644732]
Cui Y, Liang S, Zhang S, Zhang C, Zhao Y, Wu D, Wang J, Song R, Wang J, Yin D, Liu Y, Pan S, Liu X, Wang Y, Han J, Meng F, Zhang B, Guo H, Lu Z, Liu L. ABCA8 is regulated by miR-374b-5p and inhibits proliferation and metastasis of hepatocellular carcinoma through the ERK/ZEB1 pathway. Journal of experimental & clinical cancer research : CR. 2020 May 19:39(1):90. doi: 10.1186/s13046-020-01591-1. Epub 2020 May 19 [PubMed PMID: 32430024]
Wong M, Funasaka K, Obayashi T, Miyahara R, Hirooka Y, Hamaguchi M, Goto H, Senga T. AMPD3 is associated with the malignant characteristics of gastrointestinal stromal tumors. Oncology letters. 2017 Mar:13(3):1281-1287. doi: 10.3892/ol.2016.5532. Epub 2016 Dec 23 [PubMed PMID: 28454247]
Level 3 (low-level) evidenceFernandez P, Carretero J, Medina PP, Jimenez AI, Rodriguez-Perales S, Paz MF, Cigudosa JC, Esteller M, Lombardia L, Morente M, Sanchez-Verde L, Sotelo T, Sanchez-Cespedes M. Distinctive gene expression of human lung adenocarcinomas carrying LKB1 mutations. Oncogene. 2004 Jun 24:23(29):5084-91 [PubMed PMID: 15077168]
Reiss K, Del Valle L, Lassak A, Trojanek J. Nuclear IRS-1 and cancer. Journal of cellular physiology. 2012 Aug:227(8):2992-3000. doi: 10.1002/jcp.24019. Epub [PubMed PMID: 22454254]
Level 3 (low-level) evidencePedersen KM, Çolak Y, Bojesen SE, Nordestgaard BG. Low high-density lipoprotein and increased risk of several cancers: 2 population-based cohort studies including 116,728 individuals. Journal of hematology & oncology. 2020 Sep 30:13(1):129. doi: 10.1186/s13045-020-00963-6. Epub 2020 Sep 30 [PubMed PMID: 32998735]
Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998 May 27:279(20):1615-22 [PubMed PMID: 9613910]
Level 1 (high-level) evidence