
Indications
As of January 24, 2022, the United States Food and Drug Associated (FDA) fact-sheet for the drug bamlanivimab states that "due to the high frequency of the Omicron variant, bamlanivimab and etesevimab, administered together, are not currently authorized for use in any U.S. region because of markedly reduced activity against the Omicron variant. These drugs may not be administered for treatment or post-exposure prevention of COVID-19 under the Emergency Use Authorization until further notice by the Agency." This article is for historical purposes only to review the indications, mechanism, and administration of this therapy when it was first developed.
Bamlanivimab is a monoclonal antibody (mAb) directed against the spike protein (S-Protein) of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). Bamlanivimab, also known as LY-COV555, was derived from the convalescent plasma of coronavirus disease 2019 (COVID-19) patients.[1]
It is one of the potent neutralizing antibodies approved by the Food and Drug Administration (FDA) under Emergency Use Authorization (EUA) in August 2021 to be used in combination with etesivimab (another mAb against S-protein of SARS-CoV-2).[2] The other neutralizing antibodies available are casirivimab and imdevimab, which are used in combination therapy.[3][4][5] The other novel agent in this class is sotrovimab.[6]
The FDA has approved the administration of the combination drug as treatment and post-exposure prophylaxis in patients meeting the following criteria:
Treatment
- Mild to moderate COVID-19, at higher risk of progression to severe disease including hospitalization or death
- Patients with Direct SARS-CoV-2 Viral test positive results and within ten days of symptom onset
- Adults and pediatric population including neonates meeting above two criteria
Post-Exposure Prophylaxis
- Exposed to an individual infected with SARS-CoV-2 defined by close contact criteria as per Centers for Disease Control and Prevention (CDC) or at high risk for exposure in same institutional setting due to occurrence of SARS-CoV-2 in that setting, such as nursing home, prisons.
- At higher risk of progression to severe disease, including hospitalization or death
- Not fully vaccinated or not expected to have adequate response to complete vaccination. For example - patients with immunocompromising conditions, including those on immunosuppressive drugs.
- CDC describes close contact with an infected individual as being within 6 feet for at least 15 minutes, direct physical contact, droplet exposure, or providing care at home to an infected individual.
The following patient population qualifies as high-risk individuals:
- Age ≥ 65 years or <1 year
- Body mass index (BMI): Adults - BMI > 25 kg/m^2; age 12 to 17 years - BMI ≥ 85th percentile for age and sex
- Pregnancy
- Diabetes
- Cardiovascular disease including hypertension, congenital heart disease
- Lung disease - moderate to severe asthma, chronic obstructive pulmonary disease (COPD), Interstitial lung disease (ILD), cystic fibrosis, and pulmonary hypertension
- Chronic kidney disease
- Neurodevelopmental disorders
- Immunocompromised state including cancer, organ transplant, HIV, individuals on immunosuppressive treatment
- Sickle cell disease
- Dependence on medical-related technology, like tracheostomy, gastrostomy, or positive pressure ventilation unrelated to COVID-19[2]
Due to emerging variants, the FDA has authorized the combination drug to be used only in the states and territories where the data shows that resistance to the variants is < 5%. Health care providers are recommended to check the FDA website regularly for updates regarding this medication.
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
SARS-CoV-2 is a single-stranded enveloped RNA virus. The outer surface comprises the envelope protein, membrane protein, and a large number of glycosylated S-protein. The virus binds to the angiotensin-converting enzyme 2 (ACE-2) receptor of the host cell via S-protein. The S-protein comprises two subunits S1 and S2. With the help of the receptor-binding domain (RBD) of the S1 subunit, the virus binds to the ACE-2 receptor found on cells of the respiratory system, gastrointestinal system, and endothelium.[7][8]
Bamlanivimab is a neutralizing immunoglobulin G1 variant mAb to the spike protein of SARS-CoV-2. It comprises two identical light and heavy chain polypeptides composed of 214 and 455 amino acids respectively. This antibody blocks the attachment of S-protein to human ACE-2 receptors, which prevents subsequent viral entry and replication (see Image. Bamlanivimab Mechanism of Action). The drug binds an epitope on RBD in both open and closed confrontation, which led this mAb to be potentially used as a monotherapy in phase 2 of the Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) trial.[8] Bamlanivimab also showed antibody-dependent cell-mediated cytotoxicity on reporter cells following engagement with target cells that express spike protein in the in-vitro study.
This study also revealed enhanced viral clearance via an intrinsic immune response along with the mAb infusion. But with emerging variants and resistance, FDA revoked the EUA for monotherapy in April 2021. The EUA for combination therapy of bamlanivimab and etesevimab was reinstated in August 2021 with the caveat to unauthorize the use of the combination therapy where the frequency of resistance to the variants exceeds 5%.
Administration
Bamlanivimab is authorized by FDA when administered as an infusion in combination with etesevimab. It should be administered using an aseptic technique by a qualified healthcare professional at an infusion center. The infusion center should have access to immediate care in case of an infusion-related adverse reaction. Each drug comes in individual single-dose vials, stored at a refrigerated temperature of 2 degrees C to 8 degrees C. FDA recommends confirming the shelf life of unopened vials at FDA website as they authorized an extension to the shelf-life.
Prior to preparation, the vials must be allowed to equilibrate to room temperature for approximately 20 minutes. Each vial is visually inspected for any discoloration or any particulate matter. The drugs should be clear to opalescent and colorless to slightly yellow in color. The drugs are mixed with prefilled 0.9% normal saline bag (50 ml, 100 ml, 150 ml, 250 ml) and should be used immediately for infusion. If the infusion mix cannot be used immediately, the bag can be stored at a refrigerated temperature for 24 hours and at room temperature for 7 hours.
The dose recommended for treatment and post-exposure prophylaxis is as follows;
- Adults(≥18 years) and pediatric patients(<18 years, at least 40 kgs)= Bamlanivimab 700 mg + Etesevimab 1400 mg
- Pediatric patients < 40 kgs based on body weight:
- >20 kg to < 40 kgs= Bamlanivimab 350 mg + Etesevimab 700 mg
- <12 kg to 20 kg: Bamlanivimab 175 mg + Etesevimab 350 mg
- 1 kg to 12 kg: Bamlanivimab 12 mg/kg+ Etesevimab 24 mg/kg; The dosing regimen for this group is predicted based on pharmacokinetic modeling and simulation. The pediatric clinical trial included age from 10 months and weighing 8.6 kgs.
For patients weighing ≥ 40 kgs and <50 kgs, extending the infusion time to at least 70 minutes is recommended to ensure safe use. For pediatric patients <18 years and weighing <40 kgs, FDA recommends using a syringe pump and weight-based maximum infusion rate as mentioned in their Fact Sheet. No dose adjustment is necessary for geriatric, renal, or hepatic conditions. FDA also recommends providing the patient with a fact sheet regarding the information on the drugs before the infusion[2]
Adverse Effects
Limited clinical data is available for this drug therapy. Infusion-related adverse effects have been noted during the BLAZE-1 trial (randomized, placebo-control double-blind study). Currently BLAZE-2 trial is ongoing, and further data is still in process.
The adverse effects were noted in 69% of cases who received the combination infusion compared to 60% in placebo cases in the BLAZE-1 trial. The most common effects were as follows:
- GI symptoms (nausea, vomiting, diarrhea, constipation, GERD)[9][10]
- Skin-rash, pruritus, utricaria
- Dizziness[10]
However, severe hypersensitivity reactions such as anaphylaxis have also been observed. Hypersensitivity reactions occurring 24 hours post-infusion have also been reported. Infusion-related reactions have been reported during and up to 24 hours post-infusion.
Overall safety summary in FDA factsheet also mentions fever, hypo/hypertension, altered mental status, pre/syncope, cardiac (chest pain/discomfort, arrhythmias). Clinical worsening of the symptoms for COVID-19 has also been reported, with some requiring hospitalization. FDA recommends reporting any serious adverse events considered potentially related to the infusion within seven days from the onset of the event.
Contraindications
There is no absolute contraindication for the use of bamlanivimab. However, it has not been authorized for use in the following patient population:
- Hospitalized due to COVID-19 infection
- Requiring oxygen therapy
- Requiring increased oxygen supplementation due to COVID-19 compared to baseline need due to comorbidities unrelated to COVID-19
- Pre-exposure prophylaxis for COVID-19
- Substitution for vaccination
- Areas where resistance to combination or individual therapy for SARS-CoV-2 variants exceeds 5%[2]
Monitoring
Monitoring for Adverse Reaction
Patients should be assessed at the infusion center before the infusion. The high-risk category patients with mild to moderate COVID-19 disease are at high risk for progression to severe COVID-19 illness and may not qualify for the infusion.
Those who meet the criteria for infusion should be observed for any hypersensitivity reaction or infusion-related reaction mentioned above during the infusion time and at least 1-hour post-infusion. Patients should also be advised to watch out for any symptoms for at least seven days post-infusion.[2]
As bamlanivimab is not metabolized by cytochrome 450 enzymes or renally excreted, concomitant drug interactions are very unlikely.
Monitoring for Drug Resistance
There is a potential risk for treatment failure due to emerging variants that are resistant to the combination drug. The combination drug does not have activity against the Omicron variant. Updates regarding the resistance trends and authorized use of combination therapy can be accessed via the U.S department of health and human services website and the CDC website.
Toxicity
During the clinical trials, doses up to 7000 mg, i.e., ten times the authorized dose of bamlanivimab, have been administered without any dose-limiting toxicity. In case of overdose, supportive treatment is recommended, along with monitoring of vitals and clinical status. In case of an overdose, there is no specific antidote.
Specific Populations
- Pediatric use: Phase 2/3 of the BLAZE-1 Trial was completed in December 2021. No dosing adjustment were made to population of 12-18 years and weighing at least 40 kgs. Dosing adjustment recommendation besides this age/weight group is mentioned above.
- Geriatric use: BLAZE- 1 Trial included 30% of age 65 and 10% 75. No pharmacokinetic differences were noted compared to the younger population.
- Renally impairment: Renal impairment is not expected as the drug is not eliminated via the urine.
- Hepatic impairment: The drug has not been evaluated in cases of moderate or severe hepatic impairment. With mild hepatic impairment, it has been shown to have no difference compared to normal hepatic function.
- Pregnancy: Human IgG1 antibodies can cross the placental barrier. Therefore, the drug has the potential to cross the placental barrier. FDA recommends using the drug in pregnant women if the potential benefit outweighs the risk to both mother and the fetus. There are no sufficient data regarding birth defects secondary to drug use.
- Lactating mothers: Bamlanivimab has a molecular weight of 146,000 Da. Because it is a very large protein, the amount of the drug present in the milk is expected to be low.[11] There is no data available regarding the effect of bamlanivimab on breast milk production and breast-fed infant[2]. The use of the drug should be considered on an individual basis.
Nonclinical Toxicology studies including carcinogenesis, mutagenesis, and reproductive toxicology have not yet been conducted.
Enhancing Healthcare Team Outcomes
Bamlanivimab has been associated with decreasing the viral load and further spreading the disease (even as monotherapy), as shown in phase 1 of the BLAZE-1 trial. The other study by Ganesh et al. at Mayo clinic facilities from November 2020 and February 2021 revealed that bamlanivimab reduced the rate of hospitalization at days 14 and 21, along with lower intensive care admission and all-cause mortality.[12]
But with emerging new strains of the SARS-CoV-2 virus that are resistant to only bamlanivimab therapy, the use of bamlanivimab monotherapy was revoked by FDA in April 2021.[9] Later, data from phase 2/3 (ambulatory setting) of BLAZE-1 therapy revealed that the combination therapy with etesevimab has decreased the incidence of hospitalization and death in high-risk populations.[10][13]
The data from phase 3 of the BLAZE-1 clinical trial revealed an accelerated decline in viral load in patients receiving the combination therapy and reduced the rate of hospitalization by 70%.[14] The Phase 2/3 BLAZE-1 Trial also included the pediatric population, the youngest participant was 10 months and weighed 8.6 kg. BLAZE-2 study involved a single infusion of bamlanivimab 4200 mg vs placebo in residents and staff of skilled nursing facility after a confirmed positive COVID-19 test. The data revealed a reduced risk of being infected by 57% which supported post-exposure prophylaxis treatment. [15]
Primary care, Urgent and Immediate care physicians should triage patients meeting the criteria for receiving the monoclonal antibody therapy.[13][16] Patients should only receive the infusion at a well-equipped infusion center with access to advanced health facilities in case of an adverse event.
Pharmacists help in dose preparation and storage of the drug, and nurses assist in administering and monitoring the patient during and 1-hour post-infusion. Physicians and Nurses should coordinate to educate the patient regarding possible adverse effects and provide the patient with the fact sheet about the drug provided by FDA prior to the drug administration. The care team and the patient should follow the directions provided in the fact sheet to notify of any adverse event within seven calendar days.
Media
(Click Image to Enlarge)
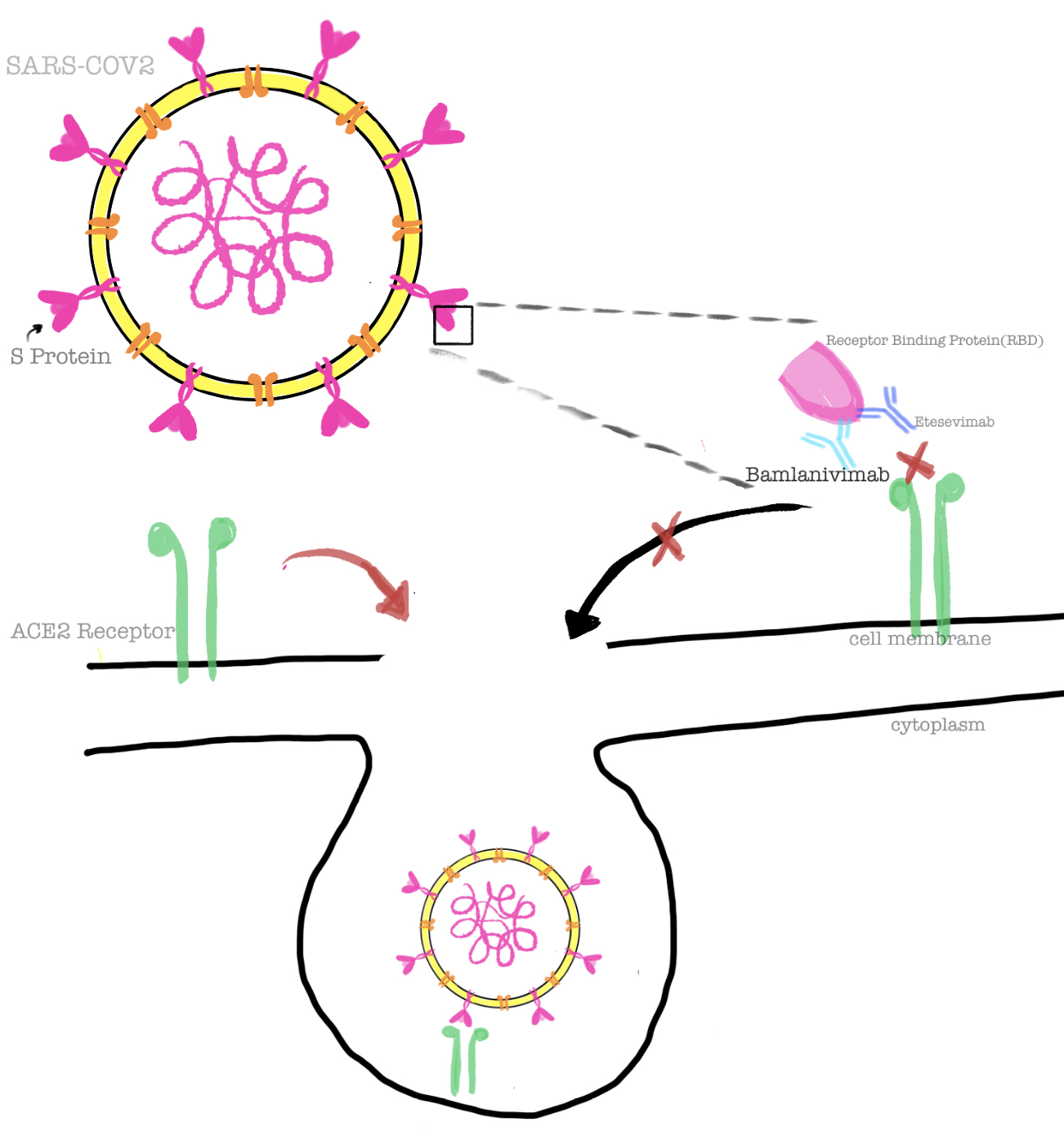
Bamlanivimab Mechanism of Action.
Contributed by J Shrestha, MD
References
Chen P, Nirula A, Heller B, Gottlieb RL, Boscia J, Morris J, Huhn G, Cardona J, Mocherla B, Stosor V, Shawa I, Adams AC, Van Naarden J, Custer KL, Shen L, Durante M, Oakley G, Schade AE, Sabo J, Patel DR, Klekotka P, Skovronsky DM, BLAZE-1 Investigators. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with Covid-19. The New England journal of medicine. 2021 Jan 21:384(3):229-237. doi: 10.1056/NEJMoa2029849. Epub 2020 Oct 28 [PubMed PMID: 33113295]
. An EUA for bamlanivimab and etesevimab for COVID-19. The Medical letter on drugs and therapeutics. 2021 Apr 5:63(1621):49-50 [PubMed PMID: 33830966]
Level 3 (low-level) evidenceSherchan R, Cannady, Jr P. Casirivimab. StatPearls. 2024 Jan:(): [PubMed PMID: 34283490]
Sherchan R,Cannady, Jr P, Imdevimab StatPearls. 2021 Jan [PubMed PMID: 34283431]
. An EUA for casirivimab and imdevimab for COVID-19. The Medical letter on drugs and therapeutics. 2020 Dec 28:62(1614):201-202 [PubMed PMID: 33451174]
Level 3 (low-level) evidence. An EUA for sotrovimab for treatment of COVID-19. The Medical letter on drugs and therapeutics. 2021 Jun 28:63(1627):97-xx98 [PubMed PMID: 34181630]
Level 3 (low-level) evidenceFocosi D, Maggi F. Neutralising antibody escape of SARS-CoV-2 spike protein: Risk assessment for antibody-based Covid-19 therapeutics and vaccines. Reviews in medical virology. 2021 Nov:31(6):e2231. doi: 10.1002/rmv.2231. Epub 2021 Mar 16 [PubMed PMID: 33724631]
Taylor PC,Adams AC,Hufford MM,de la Torre I,Winthrop K,Gottlieb RL, Neutralizing monoclonal antibodies for treatment of COVID-19. Nature reviews. Immunology. 2021 Jun [PubMed PMID: 33875867]
Dougan M, Nirula A, Azizad M, Mocherla B, Gottlieb RL, Chen P, Hebert C, Perry R, Boscia J, Heller B, Morris J, Crystal C, Igbinadolor A, Huhn G, Cardona J, Shawa I, Kumar P, Adams AC, Van Naarden J, Custer KL, Durante M, Oakley G, Schade AE, Holzer TR, Ebert PJ, Higgs RE, Kallewaard NL, Sabo J, Patel DR, Dabora MC, Klekotka P, Shen L, Skovronsky DM, BLAZE-1 Investigators. Bamlanivimab plus Etesevimab in Mild or Moderate Covid-19. The New England journal of medicine. 2021 Oct 7:385(15):1382-1392. doi: 10.1056/NEJMoa2102685. Epub 2021 Jul 14 [PubMed PMID: 34260849]
Gottlieb RL, Nirula A, Chen P, Boscia J, Heller B, Morris J, Huhn G, Cardona J, Mocherla B, Stosor V, Shawa I, Kumar P, Adams AC, Van Naarden J, Custer KL, Durante M, Oakley G, Schade AE, Holzer TR, Ebert PJ, Higgs RE, Kallewaard NL, Sabo J, Patel DR, Klekotka P, Shen L, Skovronsky DM. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA. 2021 Feb 16:325(7):632-644. doi: 10.1001/jama.2021.0202. Epub [PubMed PMID: 33475701]
Level 1 (high-level) evidence. Bamlanivimab. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 33226744]
Ganesh R,Pawlowski CF,O'Horo JC,Arndt LL,Arndt RF,Bell SJ,Bierle DM,Borgen MD,Hanson SN,Heyliger A,Larsen JJ,Lenehan PJ,Orenstein R,Puranik A,Speicher LL,Tulledge-Scheitel SM,Venkatakrishnan AJ,Wilker CG,Badley AD,Razonable RR, Intravenous bamlanivimab use associates with reduced hospitalization in high-risk patients with mild to moderate COVID-19. The Journal of clinical investigation. 2021 Oct 1 [PubMed PMID: 34411003]
Dougan M, Azizad M, Mocherla B, Gottlieb RL, Chen P, Hebert C, Perry R, Boscia J, Heller B, Morris J, Crystal C, Igbinadolor A, Huhn G, Cardona J, Shawa I, Kumar P, Blomkalns A, Adams AC, Van Naarden J, Custer KL, Knorr J, Oakley G, Schade AE, Holzer TR, Ebert PJ, Higgs RE, Sabo J, Patel DR, Dabora MC, Williams M, Klekotka P, Shen L, Skovronsky DM, Nirula A. A Randomized, Placebo-Controlled Clinical Trial of Bamlanivimab and Etesevimab Together in High-Risk Ambulatory Patients With COVID-19 and Validation of the Prognostic Value of Persistently High Viral Load. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2022 Aug 24:75(1):e440-e449. doi: 10.1093/cid/ciab912. Epub [PubMed PMID: 34718468]
Level 1 (high-level) evidenceDoggrell SA. Do we need bamlanivimab? Is etesevimab a key to treating Covid-19? Expert opinion on biological therapy. 2021 Nov:21(11):1359-1362. doi: 10.1080/14712598.2021.1985458. Epub 2021 Sep 29 [PubMed PMID: 34555986]
Level 3 (low-level) evidenceKnorr J, Tuttle JL, Sabo JA, East DH, Price KL, Shen L. Innovative clinical trial design and delivery: a phase 3 COVID-19 post-exposure prophylaxis study in skilled nursing and assisted living facilities (BLAZE-2). Trials. 2021 Oct 21:22(1):726. doi: 10.1186/s13063-021-05699-3. Epub 2021 Oct 21 [PubMed PMID: 34674750]
Level 1 (high-level) evidenceAleem A,Olarewaju O,Pozun A, Evaluating And Referring Patients For Outpatient Monoclonal Antibody Therapy For Coronavirus (COVID-19) In The Emergency Department StatPearls. 2021 Jan; [PubMed PMID: 34662075]