
Introduction
The basic concept of echocardiography was first demonstrated by Lazzaro Spallanzani in the 18 century when he described the reflected echoes of inaudible sound.[1] Hertz and Edler reported the first use of ultrasound in the cardiac evaluation and continuous monitoring of heart movements in 1954.[2] They used an industrial ultrasonic flaw detector and obtained time-varying echoes transcutaneously from the heart. The assessment of the mitral valve with the help of M-mode was the first clinical application of an echocardiogram.[3]
Since then, echocardiography has expanded tremendously and exponentially over the decades and has become an integral part of cardiac evaluation.[4] Although echocardiography started with B-mode, with the discovery of new technologies, including Doppler and 3-dimensional imaging, the echocardiographic examination has progressively become longer and more comprehensive.[5][6]
With the advent of echocardiographic contrast media and transesophageal probes, the sensitivity of echocardiographic examination has improved significantly, and it has become an important part of cardiac surgical procedures involving valvular reconstruction.[7][8]
In some aspects, new technologies have completely replaced old methods. In other circumstances, new technologies have been incorporated to enhance existing capabilities. Even in the contemporary era of newer imaging modalities, an echocardiogram is recommended as the first choice for structural and functional assessment of the heart. This chapter aims to review the basics of ultrasound physiology, important terms used in echocardiography, different echocardiographic techniques, and basic echocardiographic views.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomic Position of the Heart
The heart is normally positioned within the middle mediastinum with one-third of its mass located to the right side of the midline, and its own long axis is directed from the right shoulder (base of the heart) towards the left hypochondrium (apex of the heart). There are variations in this cardiac position related to the patient's body habitus, and minor changes may occur with respiration.[9]
At other times, diseases of the lung or pleura or other mediastinal structures can displace the heart, making image acquisition and interpretation a challenging proposition. On echocardiographic parasternal long-axis views, the right ventricular free wall is the anterior-most structure while the left ventricular posterior (inferolateral) wall is the posterior-most structure. (Figure 1)
Ultrasound Physiology
Echocardiographic probes utilize ultrasound waves (sound waves) of frequencies ranging from 1.5 to 7.5 MHz. The velocity of these waves depends on the nature of the material in which the sound travels. The normal velocity of sound in air is 330 m/s, while in the heart tissue, the velocity is around 1540 m/s.[10]
Ultrasound waves are produced due to the transformation of electrical oscillations into mechanical (sound) waves by the crystals in an echocardiographic probe. In contrast, the reflected mechanical waves are converted back to electrical signals. This phenomenon of inter-conversion of electrical and mechanical oscillations is called the piezoelectric effect. Each echocardiographic machine probe has this piezoelectric crystal transducer. On applying varying voltages, it vibrates and transmits ultrasound. On receiving the reflected ultrasound waves, the transducer generates an electrical signal analyzed by the echo machine.[11]
The ultrasound probe transmits sound waves to the body part which is being imaged. The tissues and the boundaries between them reflect the waves back to the probe. Distance from the probe to the tissue is calculated using the speed of sound in the tissue and the time of each echo's return. The two-dimensional image is formed by displaying the intensities of the echos and the distances calculated.
Indications
Echocardiographic examination indications may include the following:[12][13][14]
- Evaluation and monitoring of left ventricular systolic and diastolic function.
- Evaluation of valvular function
- Evaluation of right ventricular function
- Evaluation and quantification of cardiac chamber size.
- Evaluation of cardiac hemodynamics
- Evaluation of prosthetic valves structure and function
- Evaluation of congenital heart diseases, especially intra-cardiac shunts.
- Evaluation of coronary artery disease by stress echocardiogram
- Evaluation of the functional significance of a valvular lesion
- Evaluation of cardiac source of embolism
- Evaluation of cardiac masses
- Evaluation of pericardial diseases
Contraindications
Although transthoracic echocardiography has no contraindications, it has a few limitations. First, due to the effects of body tissue on the transmission of ultrasound waves, echocardiogram yields only limited information in patients at the extremes of body weights.
Transesophageal echocardiogram has the following contraindications:[15]
Absolute Contraindications
- Esophageal obstruction
- Pharyngeal obstruction
- Suspected or known perforated viscera
- Gastrointestinal bleeding
- Instability of cervical vertebrae
Relative Contraindications
- Esophageal varices
- Esophageal diverticula
- Cervical arthritis
- Oropharyngeal distortion
- Bleeding diathesis or coagulopathy
- Uncooperative patient
Equipment
Following equipment is required for an echocardiographic examination.
- Echocardiographic machine
- Electrocardiographic leads
- Gel, for good surface contact
- Echocardiographic contrast
- Saline for bubble contrast
- Intravenous cannula
- Defibrillator for emergency arrhythmias
Echocardiography Terms
- Frequency: Sound waves are mechanical vibrations. The number of vibrations per unit time is called frequency, expressed in Hertz, 1 Hz = 1 vibration per second. Higher the frequency of the probe, the better the resolution but, the lesser the penetration.
- Grayscale: This indicates the different amplitude detected by the ultrasound system. High amplitudes are displayed bright, low amplitudes as dark grey, and no signal as black.
- Depth and Sector: Adjusting depth helps to adjust the size of the image on the screen. Sector indicates the width of the scan area. Both influence frame rate. Higher the frame rate, the higher is the resolution.
- Gain: Increasing gain increases the overall brightness of the image.
- TGC (time gain compensation): This compensates for attenuation of ultrasound energy with depth. These knobs help to increase or decrease the brightness at different depth levels.
- Frame Rate: The more the frame rate, the better the temporal resolution. Decreasing the depth, narrowing the sector width, or using live zoom can increase the frame rate.
Personnel
- Echocardiography technologist
- Registered cardiac nurse
- Cardiologist, an expert in echocardiography/imaging
Preparation
No special preparations are required for a standard transthoracic echocardiogram. Ideally, chest hairs should be removed in male patients for good probe contact and proper image acquisition.
For transesophageal echocardiogram, patients are required to be in a fasting state for at least six hours. Intravenous access is required for the administration of drugs or contrast media. Cardiac monitoring is done throughout the procedure. Light sedation is generally helpful.
Technique or Treatment
Patient Position and Electrocardiography Lead Placement
For the parasternal and apical tomographic views, the patient is required to lie in the left lateral decubitus position, with the left arm extended behind the head. This position brings the heart into close contact with the chest wall. The subcostal and suprasternal views require the patient to be in the supine position.[16] The modified electrocardiogram (ECG) leads are placed, which allow identification of arrhythmias and timing of cardiac events during the echocardiographic examination. An electrocardiogram is used as a timing marker for digital recording gating of echocardiographic images.
Echocardiographic Modes
M Mode
Initially, echocardiographic images were obtained by sending ultrasound waves along a single line followed by the display of amplitude of the reflected signal as well as the depth of that signal on an oscilloscope, which was called A-mode echocardiography. When these lines of ultrasound images were plotted concerning time, an M-mode (motion mode) was produced. Despite the increasing emphasis on 2D and 3D imaging, the M-mode remains a complementary part of the echocardiographic examination. M mode has a high sampling rate as compared to 2D echocardiography, which provides excellent temporal resolution. It is very useful in the timing of subtle cardiac events that can be missed in the 2D echocardiographic examination. Rapidly moving structures such as the aortic valve and mitral valve, and endocardium have characteristic movements in M-mode.[17]
M-mode also has a great spatial resolution, which is useful for measuring ventricular dimensions in systole and diastole.[18] The M-mode images are displayed like graphs, with time on the x-axis and distance from the transducer on the y-axis. The structures close to the transducer are displayed at the top of the image. (Figure.2)
2D Echocardiogram
2D echocardiographic imaging provides tomographic views of various planes of the cardiac structures and acts as a guide for the M-mode and Doppler echocardiogram. In 2D echocardiographic imaging, instead of having a fixed line of sight, the scan line is swept back and forth across an arc. After complex manipulation of the data received by the transducer from the multiple scan lines, a 2D tomographic image is generated by the echocardiographic machine for display.[19]
Doppler Imaging
The introduction of the Doppler technique to the 2D echocardiography not only added new imaging capabilities but also transformed echocardiography into a modality that could provide a non-invasive hemodynamic assessment. The Doppler principle states that “the sound frequency increases as the source moves toward the observer and decreases as the source moves away.” This change in frequency between the transmitter and the reflected sound waves is called the Doppler shift.[20] This Doppler frequency shift is used to measure the velocity of the red blood cell by using the Doppler equation.[21]
The cos θ in the Doppler equation calculates velocity dependent on the angle between the beam and the moving object (red blood cell). Echocardiography machines do not typically incorporate the angle for calculating the resultant velocity. Thus, it is necessary to have the angle between the ultrasound beam and the blood flow jet as close to zero as possible (cos 0 = 1). When this is not possible, the angle should be <20° so that the true flow velocity is underestimated by <6% (cos 20 = 0.94). Adhering to this requirement sometimes mandates off-axis or unusual 2D images to align the Doppler ultrasound signal with the desired target.
Spectral Analysis: The term used to describe how Doppler images (pulsed wave Doppler and continuous wave Doppler) are displayed.
- Pulsed Wave (PW) Doppler: The purpose of PW Doppler mode is to measure the Doppler shift to assess a velocity at a specific location of interest within a small sample volume (e.g., mitral inflow velocity at the mitral valve leaflet tips, the systolic velocity at the LVOT, and blood flow within the pulmonary veins). (Figure.3)) A single crystal sends short bursts of ultrasound waves at a specific pulse repetition frequency (PRF) to a specific location in this mode. The sound waves are reflected from moving blood cells at this location and received by the same crystal.[22]. The maximal velocity that can be measured is limited by the time required to transmit and receive the reflected ultrasound wave, which is called the Nyquist limit. If a velocity is greater than the Nyquist limit, the signal appears as a wrap around the baseline called aliasing. Color Doppler and tissue Doppler imaging (TDI) are based on the principle of pulsed-wave Doppler.
- Continuous Wave (CW) Doppler: CW Doppler utilizes two crystals; one of the crystals continuously sends ultrasound waves, and the other continuously receives the waves. Unlike PW Doppler, CW Doppler measures the maximal velocity along the entire ultrasound beam, and it does not help in localizing the precise position of that peak velocity.[23] Aliasing is not a feature of continuous-wave Doppler, so it is used to measure the higher velocities, e,g aortic stenosis. (Figure.4)
In general, CW Doppler is used to assessing a high-velocity flow, and PW Doppler is used to measuring the low-velocity flow in specific areas.
3D Echocardiogram
3D echocardiographic images are obtained using a transducer that transmits and receives data simultaneously in a 3D volume, in the form of either real-time 3D images or simultaneous biplane (orthogonal) 2D images. The 3D data set is then manipulated using different software packages to assess function and anatomy. It is more accurate than 2D echocardiography for the localization of valvular abnormalities, left ventricular volume calculation, improved assessment of the right ventricle, guiding surgical interventions (e.g., mitral valve repair), and complex congenital heart disease. 3D color flow imaging allows for a comprehensive assessment of vena contracta and areas of flow convergence (PISA), which can improve the quantification of valvular regurgitation. It has been documented to allow for a more rapid evaluation of mitral valve area (MVA) in mitral stenosis as compared with conventional 2D planimetry.[24][25][26]
Echocardiographic Tomographic Views
Parasternal Views: The parasternal views are obtained in the left lateral decubitus position by placing the transducer at the left of the sternal border in the third or fourth intercostal space. A hybrid position between the steep left lateral and supine positions may be required to optimize the view. This position allows imaging of the long axis as well as the short axis of the heart.[27][16]
- Parasternal long axis (PLAX) view: The PLAX view is traditionally the first view of a standard transthoracic echocardiographic examination. The ultrasound beam is lined up between the patient’s right shoulder and the left flank. The right ventricular outflow tract (RVOT) is located at the top of the image, the aorta to the right, the inferolateral (or posterior) wall on the bottom, and the cardiac apex on the left. The anteroseptal is visualized between the right ventricular outflow tract (RVOT) and the left ventricular (LV) cavity. (Figure.1) Tilting the transducer towards the left shoulder with slight clockwise rotation brings the right ventricular (RV) inflow into view. This is good for obtaining the tricuspid regurgitation (TR) velocity and examining the tricuspid valve, RV apex, and the right atrium.
- Parasternal short axis (PSAX) view: While the transducer is in the parasternal long-axis position, rotating the transducer clockwise by approximately 90° displays the heart in the short axis. The ultrasound beam in this view is directed roughly from the left shoulder to the right flank. Using different degrees of transducer tilting, and moving up or down an intercostal space, results in different views of the heart. For example, on tilting from superior to inferior, the views obtained are aortic valve–RV outflow view, mitral valve level view, mid-ventricle at the papillary muscles, and the SAX view at the level of LV apex.
Apical Tomographic Views: The apical position is obtained with the patient in the left lateral position and the probe placed at the maximum apical impulse. This position allows imaging of the long axis of the heart.[28][16]
- Apical four-chamber (A4C) view: The A4C view is obtained with the ultrasound beam transecting the thorax in a superior-inferior fashion. In most echocardiographic laboratories, the transducer is oriented to place the left ventricle on the right side of the screen and the right ventricle on the left side. The apex is at the top of the image, and the atria are at the bottom, regardless of the orientation. The inferoseptal and anterolateral walls and the apex of the left ventricle are assessed in this view. Assessment of the right ventricular structure and function is also done in this view. (Figure.5)
- Apical five-chamber (A5C) view: A slight rotation of the transducer introduces the proximal aorta, a fifth “chamber,” as well as the aortic valve and LVOT. This view allows for qualitative assessment of aortic valve morphology along with the hemodynamic assessment of the LVOT and aortic valve.
- Apical two-chamber (A2C) view: From the apical 4C view, 90° counterclockwise rotation gives the A2C view. In this view, in addition to the left atrium, the LV anterior wall, inferior wall, apex, and mitral valve are also well visualized. (Figure.6)
- Apical long axis/three-chamber (A3C) view: A slightly more counterclockwise rotation (approximately 30°) from the A2C view brings the aorta back into the image, resulting in the A3C, or apical long-axis view. This view essentially has the same anatomical structures as those in the PLAX view with a different orientation. The apex is better visualized, and the RVOT usually drops out of the image. Additional information on mitral and aortic valve hemodynamics can also be obtained in this view. (Figure.7)
Subcostal Tomographic Views: The subcostal view is obtained with the patient in the supine position and the probe located caudal to the xiphoid process. The transducer is placed in the midline nearly parallel to the long axis of the patient’s body so that the ultrasound beam slices toward the spine. This shows the right ventricle at the top right, the left ventricle at the bottom right, and their respective atria on the left. (Figure.8) Clockwise rotation along with inferior tilting brings the inferior vena cava (IVC) and hepatic veins into view for right-sided hemodynamic assessments.[29][16]
Suprasternal Tomographic Views: Suprasternal view is obtained by placing the transducer in the suprasternal notch and pointing inferiorly. It is used to assess the ascending aorta, aortic arch, and descending aorta. Hemodynamics from this position can better characterize AR, patent ductus arteriosus, and the presence of coarctation of the aorta.[16][30]
Trans-esophageal Echocardiogram
Transesophageal echocardiography (TEE) is performed when transthoracic echocardiography (TTE) is insufficient to answer a particular question or there is a discrepancy between the clinical examination and TTE findings. It is also used to better define a pathology that has been identified by TTE or to obtain better images when transthoracic images are inadequate. The proximity of the esophagus to the heart improves visualization of the cardiac structures, particularly those located posteriorly. In addition, due to the shorter distance between the probe and the cardiac structures, higher frequency probes can be used in TEE, which further enhances the resolution. However, imaging planes are somewhat constrained by the relative position of the esophagus and the cardiac structure, making transthoracic imaging superior in assessing certain structures (i.e., pulmonic valve) and Doppler measurements.[31]
TEE is a useful imaging modality in the operating room as well as the cardiac catheterization laboratory. In cardiothoracic surgery, TEE is used to assess the mechanism of valvular abnormalities, and it subsequently helps evaluate the efficacy of valve repair or replacement. For example, TEE can be used to guide the location of the aortic cross-clamp so that the segments with severe atheromatous plaque can be avoided, thereby reducing the risk of embolization. In addition, TEE is an essential tool in providing a better assessment of left ventricular function and regional wall motion abnormalities. In congenital heart surgery, it is standard to assess the adequacy of repair with TEE in the operating room itself.
Transesophageal echocardiogram has been increasingly utilized in catheterization laboratories to help guide catheter position, transseptal punctures, implantation of percutaneous valves, and placement of left atrial appendage occluding devices, as well as the closure of periprosthetic leaks, atrial septal defects, ventricular septal defects, and patent foramen ovale. Prevention and early recognition of complications achieved by TEE imaging are often crucial for periprocedural success.[32] Details and tomographic views of transesophageal echocardiograms need a separate chapter.
Complications
Other than an allergic reaction to gel, a transthoracic echocardiogram has no significant complications. A transesophageal echocardiogram is rarely associated with trauma to the teeth, oral mucosa, and esophagus. Esophageal rupture, vasovagal reflex, and aspiration pneumonia are the other rare complications associated with a transesophageal echocardiogram.
Clinical Significance
Echocardiography is a reliable and non-invasive imaging modality for assessing cardiac structure, function, and hemodynamics. Compared to other cardiovascular imaging modalities, it is easily available and relatively inexpensive and does not expose the patient to radiation. Portable machines provide the ease of doing the study at the bedside for sick patients. Echocardiography displays live real-time images and are widely available. Although it is operator-dependent, its accuracy is comparable with other imaging modalities.[33]
Enhancing Healthcare Team Outcomes
A comprehensive echocardiographic examination requires a team that includes an imaging cardiologist as well as an echocardiography technician. It is vital to take a proper history and perform a detailed physical examination pre-procedure to understand the appropriate indications of the procedure. Communication between the referring physician, echocardiography technicians, and the cardiologist is essential, especially when there is a discrepancy in the clinical examination and echocardiography findings.
Media
(Click Image to Enlarge)
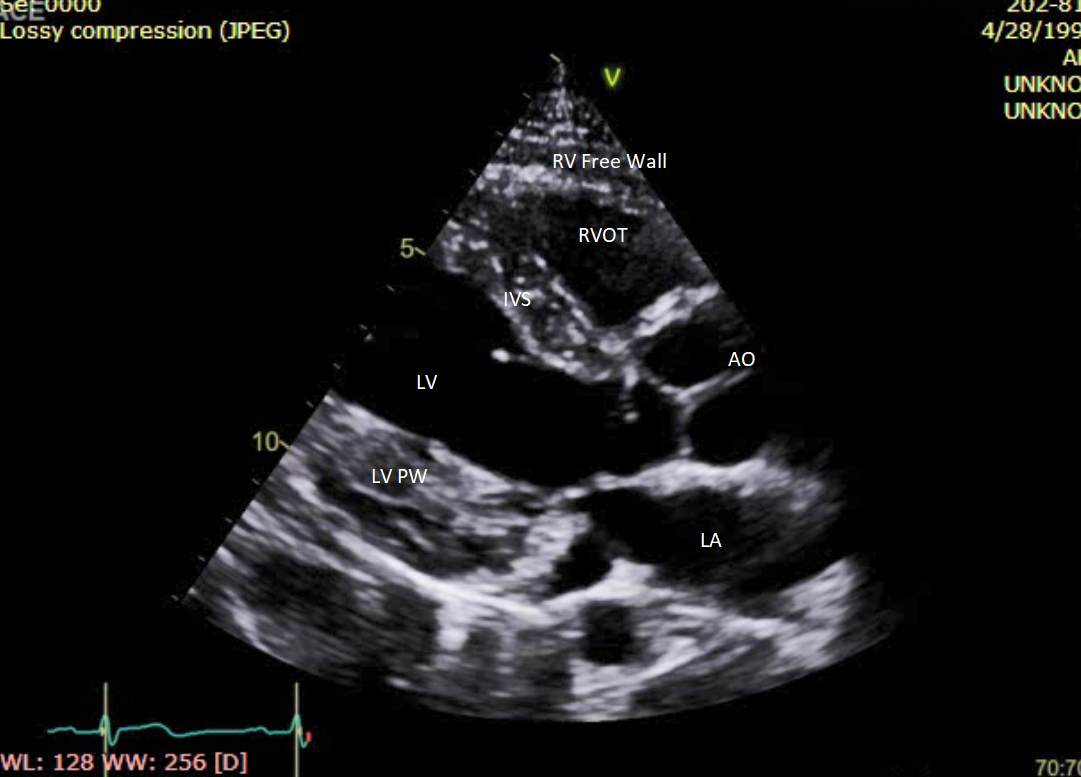
Figure.1 Parasternal long axis (PLAX) view. RV=Right ventricle, RVOT= Right ventricular outflow tract, LV= Left ventricle, LV PW= Left ventricular posterior wall, LA= Left atrium, AO= Aorta, IVS= Interventricular septum
Contributed by Intisar Ahmed
(Click Image to Enlarge)
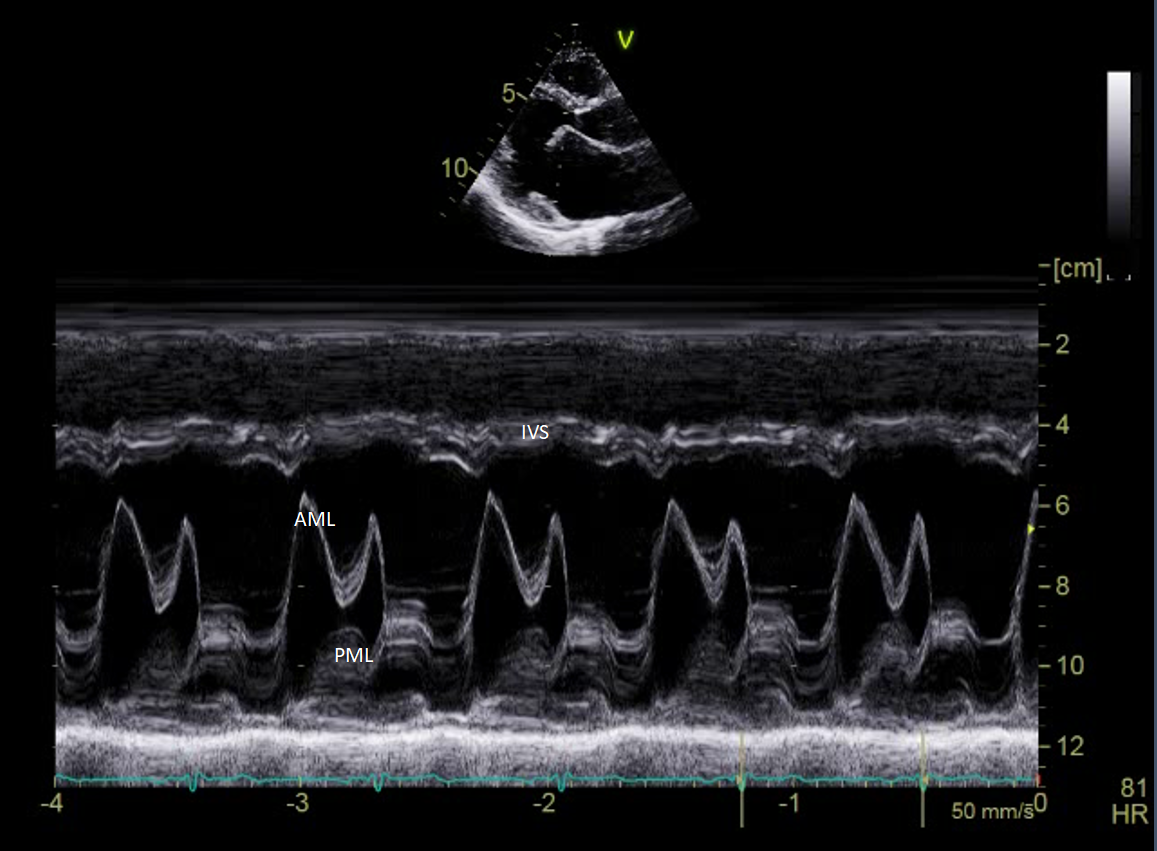
Figure.2 M-mode at mitral valve leaflets. AML=Anterior mitral leaflet, PML= Posterior mitral leaflet, IVS= Interventricular septum
Contributed by Intisar Ahmed
(Click Image to Enlarge)
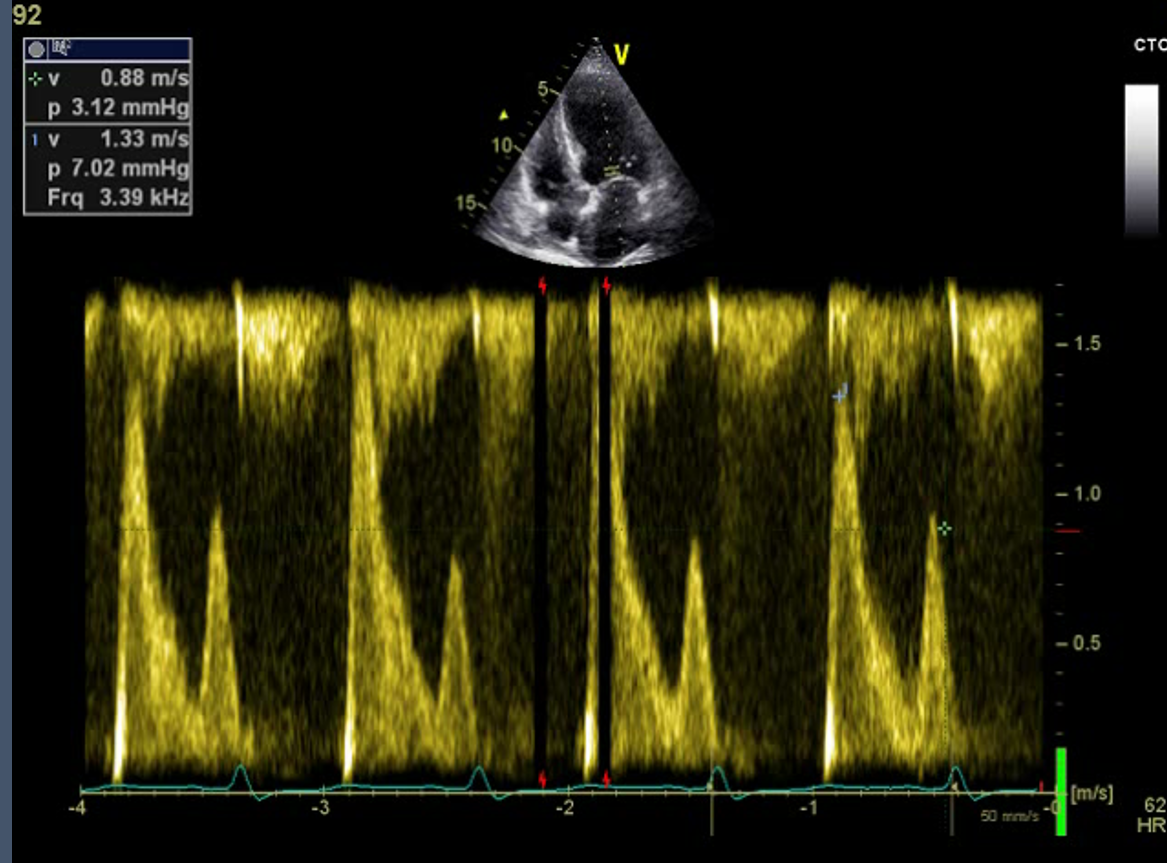
Figure.3 Pulsed wave (PW) Doppler at mitral inflow.
Contributed by Intisar Ahmed
(Click Image to Enlarge)
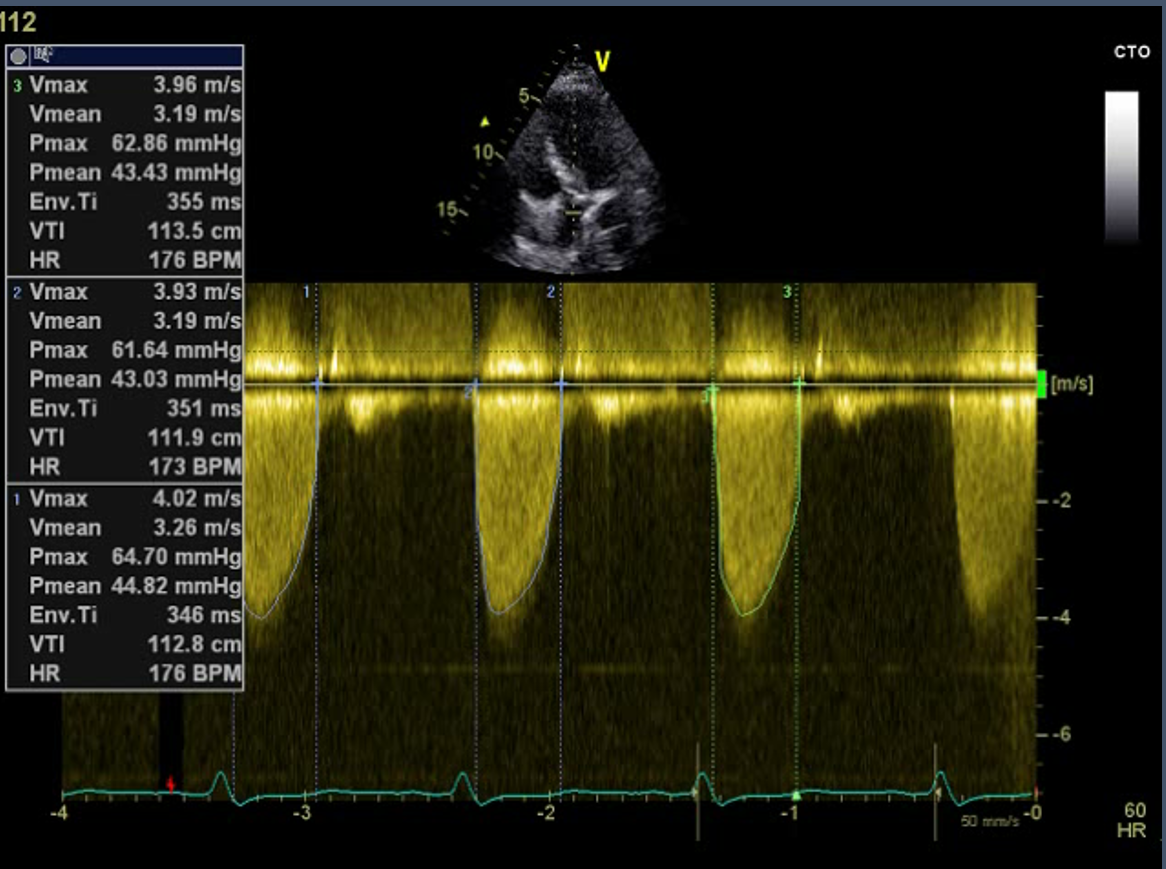
Figure.4 Continuous wave (CW) Doppler at aortic valve
Contributed by Intisar Ahmed
(Click Image to Enlarge)
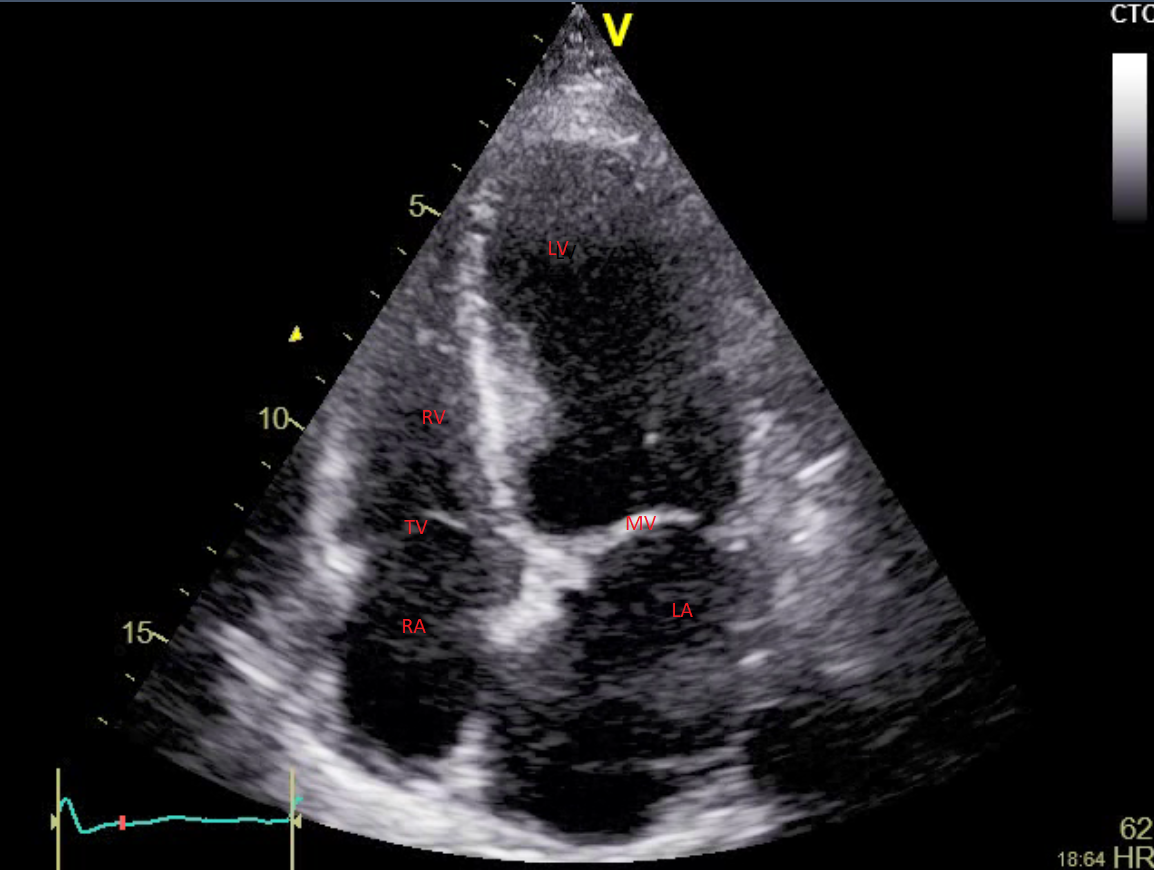
Figure.5 Apical four chamber (A4C) view. LV= Left ventricle, RV= Right ventricle, LA= Left atrium, RA= Right atrium, MV= Mitral valve, TV= Tricuspid valve
Contributed by Intisar Ahmed
References
Singh S, Goyal A. The origin of echocardiography: a tribute to Inge Edler. Texas Heart Institute journal. 2007:34(4):431-8 [PubMed PMID: 18172524]
Edler I, Hertz CH. The use of ultrasonic reflectoscope for the continuous recording of the movements of heart walls. 1954. Clinical physiology and functional imaging. 2004 May:24(3):118-36 [PubMed PMID: 15165281]
Mintz GS, Kotler MN, Parry WR, Segal BL. Statistical comparison of M mode and two dimensional echocardiographic diagnosis of flail mitral leaflets. The American journal of cardiology. 1980 Feb:45(2):253-9 [PubMed PMID: 7355735]
Bom N,van der Steen AF,de Jong N,Roelandt JR, Early, recent and future applications of echocardiography. Clinical physiology and functional imaging. 2004 May; [PubMed PMID: 15165283]
Coman IM, Popescu BA. Shigeo Satomura: 60 years of Doppler ultrasound in medicine. Cardiovascular ultrasound. 2015 Dec 23:13():48. doi: 10.1186/s12947-015-0042-3. Epub 2015 Dec 23 [PubMed PMID: 26699126]
Li X, Ashraf M, Thiele K, Bhat AH, Sakaguchi R, Mitchell JC, Brie JA, Young M, Bader RS, Pemberton J, Sahn DJ. A novel method for the assessment of the accuracy of computing laminar flow stroke volumes using a real-time 3D ultrasound system: In vitro studies. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2005 Dec:6(6):396-404 [PubMed PMID: 15927537]
Level 3 (low-level) evidenceKaragodin I, Genovese D, Kruse E, Patel AR, Rashedi N, Lang RM, Mor-Avi V. Contrast-enhanced echocardiographic measurement of longitudinal strain: accuracy and its relationship with image quality. The international journal of cardiovascular imaging. 2020 Mar:36(3):431-439. doi: 10.1007/s10554-019-01732-4. Epub 2019 Nov 13 [PubMed PMID: 31720940]
Level 2 (mid-level) evidenceHan JC,Zhang HB,Gao S,Yu SM,Han J,Meng X,He YH, [Evaluation of the intraoperative transesophageal echocardiography for the aortic valve reconstruction]. Zhonghua yi xue za zhi. 2018 Oct 16; [PubMed PMID: 30392264]
Anderson RH, Razavi R, Taylor AM. Cardiac anatomy revisited. Journal of anatomy. 2004 Sep:205(3):159-77 [PubMed PMID: 15379923]
Holmes JH. Diagnostic ultrasound during the early years of A.I.U.M. Journal of clinical ultrasound : JCU. 1980 Aug:8(4):299-308 [PubMed PMID: 6772678]
Krishnamoorthy VK, Sengupta PP, Gentile F, Khandheria BK. History of echocardiography and its future applications in medicine. Critical care medicine. 2007 Aug:35(8 Suppl):S309-13 [PubMed PMID: 17667454]
American College of Cardiology Foundation Appropriate Use Criteria Task Force.,American Society of Echocardiography.,American Heart Association.,American Society of Nuclear Cardiology.,Heart Failure Society of America.,Heart Rhythm Society.,Society for Cardiovascular Angiography and Interventions.,Society of Critical Care Medicine.,Society of Cardiovascular Computed Tomography.,Society for Cardiovascular Magnetic Resonance.,American College of Chest Physicians.,Douglas PS,Garcia MJ,Haines DE,Lai WW,Manning WJ,Patel AR,Picard MH,Polk DM,Ragosta M,Parker Ward R,Weiner RB, ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2011 Mar; [PubMed PMID: 21338862]
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P, Dehmer GJ, Doherty JU, Schoenhagen P, Amin Z, Bashore TM, Boyle A, Calnon DA, Carabello B, Cerqueira MD, Conte J, Desai M, Edmundowicz D, Ferrari VA, Ghoshhajra B, Mehrotra P, Nazarian S, Reece TB, Tamarappoo B, Tzou WS, Wong JB, Doherty JU, Dehmer GJ, Bailey SR, Bhave NM, Brown AS, Daugherty SL, Dean LS, Desai MY, Duvernoy CS, Gillam LD, Hendel RC, Kramer CM, Lindsay BD, Manning WJ, Mehrotra P, Patel MR, Sachdeva R, Wann LS, Winchester DE, Wolk MJ, Allen JM. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate Use Criteria for Multimodality Imaging in Valvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2018 Apr:31(4):381-404. doi: 10.1016/j.echo.2017.08.012. Epub 2017 Oct 20 [PubMed PMID: 29066081]
Writing Group Members, Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P, Rating Panel Members, Dehmer GJ, Doherty JU, Schoenhagen P, Bashore TM, Bhave NM, Calnon DA, Carabello B, Conte J, Dickfeld T, Edmundowicz D, Ferrari VA, Hall ME, Ghoshhajra B, Mehrotra P, Naqvi TZ, Reece TB, Starling RC, Szerlip M, Tzou WS, Wong JB, Appropriate Use Criteria Task Force, Doherty JU, Dehmer GJ, Bailey SR, Bhave NM, Brown AS, Daugherty SL, Dean LS, Desai MY, Duvernoy CS, Gillam LD, Hendel RC, Kramer CM, Lindsay BD, Manning WJ, Patel MR, Sachdeva R, Wann LS, Winchester DE, Wolk MJ. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2019 Appropriate Use Criteria for Multimodality Imaging in the Assessment of Cardiac Structure and Function in Nonvalvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and the Society of Thoracic Surgeons. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2019 May:32(5):553-579. doi: 10.1016/j.echo.2019.01.008. Epub 2019 Feb 7 [PubMed PMID: 30744922]
Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D'Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010 Nov:23(11):1115-27; quiz 1220-1. doi: 10.1016/j.echo.2010.08.013. Epub [PubMed PMID: 20864313]
Mitchell C,Rahko PS,Blauwet LA,Canaday B,Finstuen JA,Foster MC,Horton K,Ogunyankin KO,Palma RA,Velazquez EJ, Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2019 Jan; [PubMed PMID: 30282592]
Feigenbaum H. Role of M-mode technique in today's echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010 Mar:23(3):240-57; 335-7. doi: 10.1016/j.echo.2010.01.015. Epub [PubMed PMID: 20206828]
Kühl HP, Hanrath P, Franke A. M-mode echocardiography overestimates left ventricular mass in patients with normal left ventricular shape: a comparative study using three-dimensional echocardiography. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2003 Dec:4(4):312-9 [PubMed PMID: 14611828]
Level 2 (mid-level) evidenceBonagura JD, Blissitt KJ. Echocardiography. Equine veterinary journal. Supplement. 1995 Sep:(19):5-17 [PubMed PMID: 8933064]
Level 3 (low-level) evidenceNaredo E,Monteagudo I, Doppler techniques. Clinical and experimental rheumatology. 2014 Jan-Feb; [PubMed PMID: 24529255]
Level 3 (low-level) evidencePellett AA, Kerut EK. The Doppler equation. Echocardiography (Mount Kisco, N.Y.). 2004 Feb:21(2):197-8 [PubMed PMID: 14961804]
Mao YK, Zhao BW, Zhou L, Wang B, Chen R, Wang SS. Z-score reference ranges for pulsed-wave Doppler indices of the cardiac outflow tracts in normal fetuses. The international journal of cardiovascular imaging. 2019 May:35(5):811-825. doi: 10.1007/s10554-018-01517-1. Epub 2019 Jan 8 [PubMed PMID: 30623353]
Bolger AF, Eidenvall L, Ask P, Loyd D, Wranne B. Understanding continuous-wave Doppler signal intensity as a measure of regurgitant severity. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 1997 Jul-Aug:10(6):613-22 [PubMed PMID: 9282351]
Level 3 (low-level) evidenceMowers KL,Fullerton JB,Hicks D,Singh GK,Johnson MC,Anwar S, 3D Echocardiography Provides Highly Accurate 3D Printed Models in Congenital Heart Disease. Pediatric cardiology. 2021 Jan; [PubMed PMID: 33083888]
Lakatos BK, Tokodi M, Kispál E, Merkely B, Kovács A. Morphological and Functional Assessment of the Right Ventricle Using 3D Echocardiography. Journal of visualized experiments : JoVE. 2020 Oct 28:(164):. doi: 10.3791/61214. Epub 2020 Oct 28 [PubMed PMID: 33191942]
Sugimoto T, Dulgheru R, Marchetta S, Ilardi F, Contu L, Go YY, Lancellotti P. What Does 3D Echocardiography Add to 2D Echocardiography in the Assessment of Mitral Regurgitation? Current cardiology reports. 2017 Aug 24:19(10):90. doi: 10.1007/s11886-017-0901-7. Epub 2017 Aug 24 [PubMed PMID: 28840567]
Remenyi B, Davis K, Draper A, Bayley N, Paratz E, Reeves B, Appelbe A, Wheaton G, da Silva Almeida IT, Dos Santos J, Carapetis J, Francis JR. Single Parasternal-Long-Axis-View-Sweep Screening Echocardiographic Protocol to Detect Rheumatic Heart Disease: A Prospective Study of Diagnostic Accuracy. Heart, lung & circulation. 2020 Jun:29(6):859-866. doi: 10.1016/j.hlc.2019.02.196. Epub 2019 Jun 11 [PubMed PMID: 31320258]
Denault AY,Langevin S,Lessard MR,Courval JF,Desjardins G, Transthoracic echocardiographic evaluation of the heart and great vessels. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2018 Apr; [PubMed PMID: 29352414]
Flower L, Madhivathanan PR, Andorka M, Olusanya O, Roshdy A, Sanfilippo F. Getting the most from the subcostal view: The rescue window for intensivists. Journal of critical care. 2021 Jun:63():202-210. doi: 10.1016/j.jcrc.2020.09.003. Epub 2020 Sep 13 [PubMed PMID: 32958350]
Zhang XY, Cao TS, Yuan LJ, Liu J, Duan YY. Value of the echocardiographic suprasternal view for diagnosis of patent ductus arteriosus subtypes. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2012 Sep:31(9):1421-7 [PubMed PMID: 22922622]
Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, Lang RM, Reeves ST, Shanewise JS, Siu SC, Stewart W, Picard MH. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2013 Sep:26(9):921-64. doi: 10.1016/j.echo.2013.07.009. Epub [PubMed PMID: 23998692]
Mahmood F, Shernan SK. Perioperative transoesophageal echocardiography: current status and future directions. Heart (British Cardiac Society). 2016 Aug 1:102(15):1159-67. doi: 10.1136/heartjnl-2015-307962. Epub 2016 Apr 5 [PubMed PMID: 27048769]
Level 3 (low-level) evidenceChiriac A, Kadkhodayan A, Pislaru SV, Dailey EJ, Scott CG, Buechler TE, Newman JS, Pellikka PA. Clinical Importance of Transthoracic Echocardiography with Direct Input from Treating Physicians. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2016 Mar:29(3):195-204. doi: 10.1016/j.echo.2015.11.009. Epub 2015 Dec 11 [PubMed PMID: 26687690]