[1]
Baghdanian AH, Baghdanian AA, Armetta A, Babayan RK, LeBedis CA, Soto JA, Anderson SW. Utility of MDCT findings in predicting patient management outcomes in renal trauma. Emergency radiology. 2017 Jun:24(3):263-272. doi: 10.1007/s10140-016-1473-3. Epub 2016 Dec 21
[PubMed PMID: 28004326]
[2]
Ząbkowski T, Skiba R, Saracyn M, Zieliński H. Analysis of Renal Trauma in Adult Patients: A 6-Year Own Experiences of Trauma Center. Urology journal. 2015 Sep 4:12(4):2276-9
[PubMed PMID: 26341772]
[3]
McPhee M, Arumainayagam N, Clark M, Burfitt N, DasGupta R. Renal injury management in an urban trauma centre and implications for urological training. Annals of the Royal College of Surgeons of England. 2015 Apr:97(3):194-7. doi: 10.1308/003588414X14055925061117. Epub
[PubMed PMID: 26263803]
[4]
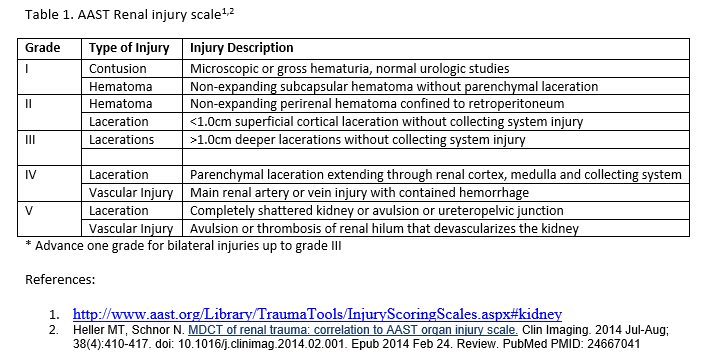
Heller MT, Schnor N. MDCT of renal trauma: correlation to AAST organ injury scale. Clinical imaging. 2014 Jul-Aug:38(4):410-417. doi: 10.1016/j.clinimag.2014.02.001. Epub 2014 Feb 24
[PubMed PMID: 24667041]
[5]
Voelzke BB, Leddy L. The epidemiology of renal trauma. Translational andrology and urology. 2014 Jun:3(2):143-9. doi: 10.3978/j.issn.2223-4683.2014.04.11. Epub
[PubMed PMID: 26816762]
[6]
Dayal M, Gamanagatti S, Kumar A. Imaging in renal trauma. World journal of radiology. 2013 Aug 28:5(8):275-84. doi: 10.4329/wjr.v5.i8.275. Epub
[PubMed PMID: 24003353]
[7]
Hotaling JM, Sorensen MD, Smith TG 3rd, Rivara FP, Wessells H, Voelzke BB. Analysis of diagnostic angiography and angioembolization in the acute management of renal trauma using a national data set. The Journal of urology. 2011 Apr:185(4):1316-20. doi: 10.1016/j.juro.2010.12.003. Epub 2011 Feb 22
[PubMed PMID: 21334643]
[8]
Breyer BN, McAninch JW, Elliott SP, Master VA. Minimally invasive endovascular techniques to treat acute renal hemorrhage. The Journal of urology. 2008 Jun:179(6):2248-52; discussion 2253. doi: 10.1016/j.juro.2008.01.104. Epub 2008 Apr 18
[PubMed PMID: 18423679]
[9]
Joseph DK, Daman D, Kinler RL, Burns K, Jacobs L. Management of Major Blunt Renal Injury: A Twelve-Year Review at an Urban, Level I Trauma Hospital. The American surgeon. 2018 Mar 1:84(3):451-454
[PubMed PMID: 29559064]
[10]
Brandes SB, McAninch JW. Urban free falls and patterns of renal injury: a 20-year experience with 396 cases. The Journal of trauma. 1999 Oct:47(4):643-9; discussion 649-50
[PubMed PMID: 10528597]
Level 3 (low-level) evidence
[11]
Gross JA, Lehnert BE, Linnau KF, Voelzke BB, Sandstrom CK. Imaging of Urinary System Trauma. Radiologic clinics of North America. 2015 Jul:53(4):773-88, ix. doi: 10.1016/j.rcl.2015.02.005. Epub 2015 Apr 9
[PubMed PMID: 26046510]
[12]
Mingoli A, La Torre M, Migliori E, Cirillo B, Zambon M, Sapienza P, Brachini G. Operative and nonoperative management for renal trauma: comparison of outcomes. A systematic review and meta-analysis. Therapeutics and clinical risk management. 2017:13():1127-1138. doi: 10.2147/TCRM.S139194. Epub 2017 Aug 31
[PubMed PMID: 28894376]
Level 1 (high-level) evidence
[13]
van der Wilden GM, Velmahos GC, Joseph DK, Jacobs L, Debusk MG, Adams CA, Gross R, Burkott B, Agarwal S, Maung AA, Johnson DC, Gates J, Kelly E, Michaud Y, Charash WE, Winchell RJ, Desjardins SE, Rosenblatt MS, Gupta S, Gaeta M, Chang Y, de Moya MA. Successful nonoperative management of the most severe blunt renal injuries: a multicenter study of the research consortium of New England Centers for Trauma. JAMA surgery. 2013 Oct:148(10):924-31. doi: 10.1001/jamasurg.2013.2747. Epub
[PubMed PMID: 23945834]
Level 2 (mid-level) evidence
[14]
Martin JG, Shah J, Robinson C, Dariushnia S. Evaluation and Management of Blunt Solid Organ Trauma. Techniques in vascular and interventional radiology. 2017 Dec:20(4):230-236. doi: 10.1053/j.tvir.2017.10.001. Epub 2017 Nov 10
[PubMed PMID: 29224654]
[15]
Aragona F, Pepe P, Patanè D, Malfa P, D'Arrigo L, Pennisi M. Management of severe blunt renal trauma in adult patients: a 10-year retrospective review from an emergency hospital. BJU international. 2012 Sep:110(5):744-8. doi: 10.1111/j.1464-410X.2011.10901.x. Epub 2012 Feb 7
[PubMed PMID: 22313622]
Level 2 (mid-level) evidence
[16]
Morey AF, Brandes S, Dugi DD 3rd, Armstrong JH, Breyer BN, Broghammer JA, Erickson BA, Holzbeierlein J, Hudak SJ, Pruitt JH, Reston JT, Santucci RA, Smith TG 3rd, Wessells H, American Urological Assocation. Urotrauma: AUA guideline. The Journal of urology. 2014 Aug:192(2):327-35. doi: 10.1016/j.juro.2014.05.004. Epub 2014 May 20
[PubMed PMID: 24857651]
[17]
Xu J, Yu Q, Zhu S, Li S. Evaluation of a lens opacities classification system II (LOCS II) in the survey population-based sample. Yan ke xue bao = Eye science. 1991 Sep:7(3):140-2
[PubMed PMID: 1842367]
Level 3 (low-level) evidence
[18]
Starnes M, Demetriades D, Hadjizacharia P, Inaba K, Best C, Chan L. Complications following renal trauma. Archives of surgery (Chicago, Ill. : 1960). 2010 Apr:145(4):377-81; discussion 381-2. doi: 10.1001/archsurg.2010.30. Epub
[PubMed PMID: 20404289]