Learning Outcome
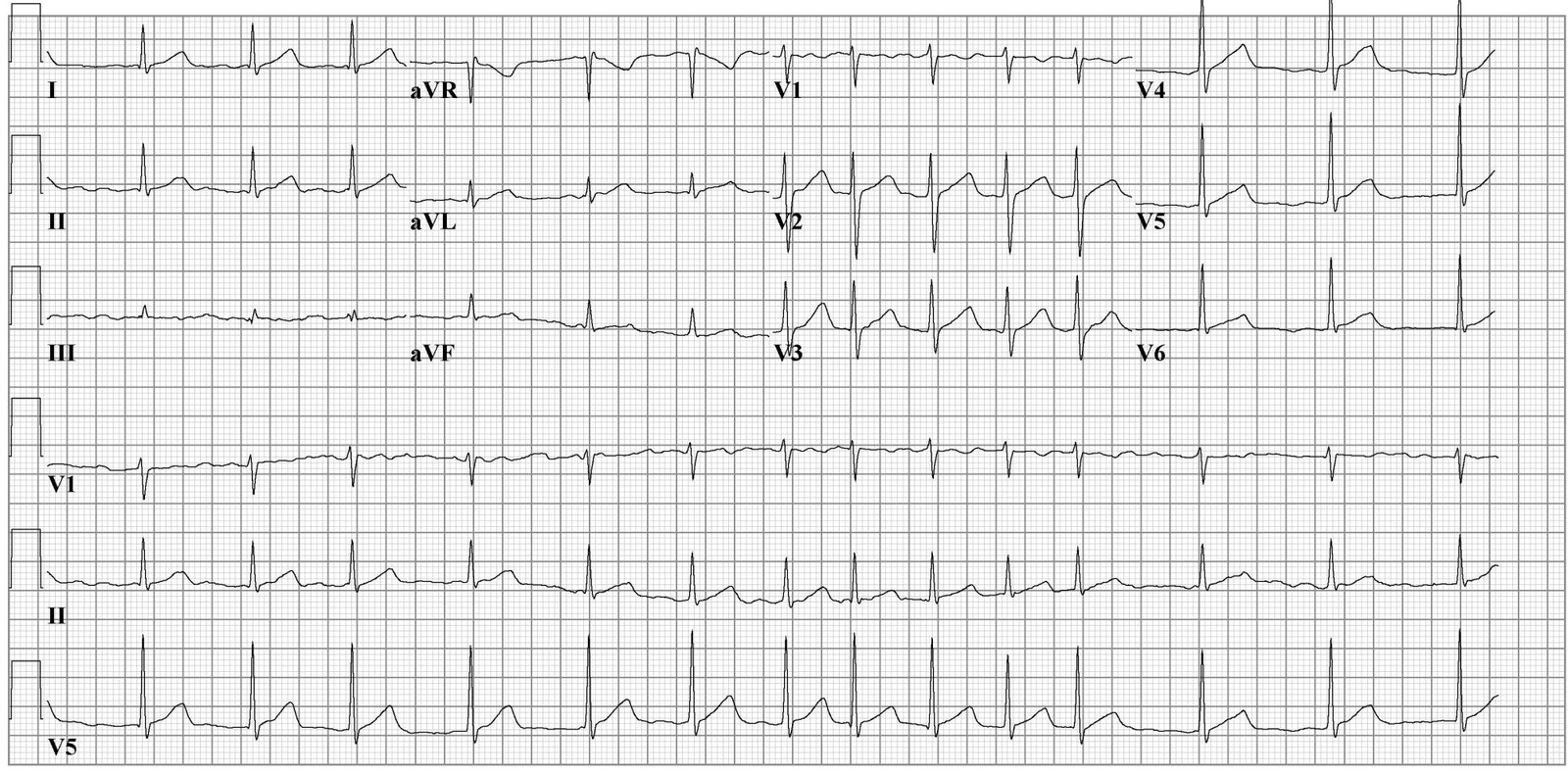
- Know the ECG features of atrial fibrillation
- Describe the risk factors for atrial fibrillation
- Learn how to manage a patient with atrial fibrillation
- Recall the complications of atrial fibrillation

Atrial fibrillation is the most common type of heart arrhythmia. It is due to abnormal electrical activity within the atria of the heart causing them to fibrillate. Is characterized as a tachyarrhythmia, which means that the heart rate is often fast. This arrhythmia may be paroxysmal (less than 7 days) or persistent (more than 7 days). Due to its rhythm irregularity, blood flow through the heart becomes turbulent and has a high chance of forming a thrombus (blood clot) which can ultimately dislodge and cause a stroke. Atrial fibrillation is the leading cardiac cause of stroke. Risk factors for atrial fibrillation include advanced age, high blood pressure, underlying heart and lung disease, congenital heart disease, and increased alcohol consumption. Symptoms vary from asymptomatic to symptoms such as chest pain, palpitations, fast heart rate, shortness of breath, nausea, dizziness, diaphoresis (severe sweating), and generalized fatigue. Although atrial fibrillation may be a permanent disease, various treatments have been developed, and risk modifying strategies to help reduce the risk of stroke in patients that remain in atrial fibrillation exist. Treatments include anticoagulation, rate control medication, rhythm control medication, cardioversion, ablation, and other interventional cardiac procedures. [1][2][3]
There are many causes of atrial fibrillation. Advanced age, congenital heart disease, underlying heart disease (valvular disease, coronary artery disease, structural heart disease), increased alcohol consumption, hypertension, and obstructive sleep apnea are all common causes of atrial fibrillation. Any process that causes inflammation, stress, damage, and ischemia to the structure and electrical system of the heart can lead to the development of atrial fibrillation. In some cases, the cause is iatrogenic.[4]
The prevalence of atrial fibrillation has been increasing worldwide. It is known that the prevalence of atrial fibrillation generally increases with age. It has been estimated that the number of individuals with atrial fibrillation will double or triple by the year 2050. Although the world white prevalence of atrial fibrillation is approximately 1%, it is found in approximately 9% in individuals over the age of 75. At the age of 80, the lifetime risk of developing atrial fibrillation jumps to 22%. In addition, atrial fibrillation has more commonly been associated with males and seen more often in whites as compared to black.[5][6]
History and physical exam are crucial for diagnosing and risk stratifying patients with atrial fibrillation. A complete history should focus on symptoms such as palpitations, chest pain, shortness of breath, increased lower extremity swelling, dyspnea with exertion, dizziness, among others. In addition, history is imperative in identifying risk factors such as hypertension, history of valvular, structure, or ischemic heart disease, obstructive sleep apnea, obesity hypoventilation syndrome, smoking, alcohol intake, illicit drug use, history of rheumatic fever/heart disease, history of pericarditis, hyperlipidemia, among others. A physical exam should include the patient's overall appearance (obese), examine the patient neck for signs of JVD, carotid bruits, circumference. A cardiovascular exam should consist of carefully auscultating all 4 cardiac posts and palpating for apical impulse. A pulmonary exam should consist of auscultation, percussion, and specialized tests, if needed, to assess pulmonary status. Extremities should be evaluated for edema, peripheral pulses in both upper and lower extremities, and integumentary signs of PVD such as hair loss and skin breakdown. An abdominal exam should consist of palpating the aorta and listening for abdominal bruits. Depending on the severity of the atrial fibrillation, signs, and symptoms can range from none to evidence of acute heart failure.
Aside from a detailed history and examine, the ECG is critical in making the diagnosis of atrial fibrillation. On ECG, atrial fibrillation presents with the typical narrow complex "irregularly irregular" pattern with no distinguishable p-waves. Laboratory work is required to evaluate for the causes of atrial fibrillation, for example, a complete blood count (CBC) for infection, basic metabolic panel (BMP) for electrolyte abnormalities, thyroid function tests to evaluate for hyperthyroidism, and a chest x-ray to evaluate the thorax for any abnormality. It is imperative to evaluate the patient for pulmonary embolism (for example with d-dimer, CT scan) because right heart strain can lead to atrial malfunctioning and result in atrial fibrillation. The patient should be risk stratified for pulmonary embolism using the PERC and/or Wells criteria. In addition, a transesophageal echocardiogram should be done for these patients to evaluate for atrial thrombus secondary to atrial fibrillation and heart structure. It is important to note that Transesophageal echocardiogram (TEE) should always be done prior to cardioversion for these patients to minimize the risk of stroke.[7][8]
The management of atrial fibrillation in the acute setting relies on patient hemodynamic stability and risk stratification. If the patient is hemodynamically unstable, immediate cardioversion with anticoagulant therapy is indicated. TEE is recommended prior to any cardioversion; however, if the patient is in hemodynamic stability due to atrial fibrillation with a rapid ventricular response, cardioversion may be performed without prior TEE. If the patient has evidence of rapid ventricular response, rate control should be initiated using a beta-blocker or calcium-channel blocker. These medications can be used as intravenous (IV) pushes or drips. Typically, the patient is given a bolus then started on a drip if symptoms do not resolve. Digoxin can be considered as a rate control agent but is not recommended as a first-line agent due to its side-effects and tolerance. Amiodarone can also be considered for a rhythm controlling agent but is also not first-line therapy in the acute setting. Amiodarone is also considered as a rhythm control, but cardiology should be consulted prior to use.
In the chronic setting of atrial fibrillation, the patient should be risk stratified using the CHADs-2-Vasc score which is helpful in estimate risk of CVA per year. If the patient receives a 0 score, they will be considered "low-risk" and anticoagulation is not recommended. If the patient receives a score of 1, they are "low-moderate" risk; the physician should consider anticoagulant or antiplatelet therapy. If the patient receives a score of greater than 2, they are in the "moderate-high" risk, and anticoagulation therapy is indicated.[2] Rate or rhythm control should also be given to the patient, medications such as beta-blockers, calcium channel blockers, amiodarone, dronedarone, and digoxin. HAS-BLED is also a scoring system that can be used to asses the risk of bleeding for the patient. This is a good indicator of bleeding risk for a patient that is considering starting anticoagulation.
Non-pharmacological therapy includes ablation therapy. Pacemaker placement is considered in severe causes resulting in heart failure in atrial fibrillation.[9][10][11]
Atrial fibrillation is a chronic disorder that can seriously affect the quality of life and costs the healthcare billions of dollars each year. While cardiologists treat the disorder, the role of the pharmacist is critical. Many of these patients are on multiple medications including antiarrhythmic agents and anticoagulants. In addition, there is some evidence indicating that use of Angiotensin receptor blockers and statins may lower the frequency of atrial fibrillation and increase the probability of successful cardioversion. Thus, the pharmacist has to make sure that the patient' medication doses are therapeutic, there are no drug interactions and that the patient has therapeutic anticoagulation to prevent a stroke. The nurse has to educate the patient on medication compliance for hypertension, coronary disease and ensure follow-up at regular intervals. Finally, the patient should be educated about the symptoms of a stroke and when to return to the emergency department.[12][13][14] (Level V)
Outcomes
Atrial fibrillation prevalence has been on the rise. The risk of stroke is 5-times higher in a patient with known atrial fibrillation compared to the general public. It is estimated that 19.6% of patients over the age of 65, will have apparent atrial fibrillation by 2030. The most feared side effect of atrial fibrillation is acute stroke which can lead to severe morbidity and mortality. It has been shown though that 60% of strokes secondary to atrial fibrillation can be avoided with the use of anticoagulants. Using the CHADs-2-VASc score to evaluate patients with atrial fibrillation is a helpful guide for management of these patients with the ultimate goal of preventing stroke. Proper risk factor stratification and medical/surgical therapy can decrease the risk of stroke and heart failure significantly.[3]
Atrial fibrillation is a common disease that affects many individuals. The prevalence of this disease increases with age with the most severe complication being acute CVA. Due to the irregularly of the atria, blood blow through this chamber becomes turbulent leading to a blood clot (thrombus). This thrombus is commonly found in the atrial appendage. The thrombus can dislodge and embolize to the brain and other parts of the body. It is important for the patient to seek medical care immediately if they are experiencing chest pain, palpitations, shortness of breath, severe sweating, or extreme dizziness.


Markides V, Schilling RJ. Atrial fibrillation: classification, pathophysiology, mechanisms and drug treatment. Heart (British Cardiac Society). 2003 Aug:89(8):939-43 [PubMed PMID: 12860883]
Amin A, Houmsse A, Ishola A, Tyler J, Houmsse M. The current approach of atrial fibrillation management. Avicenna journal of medicine. 2016 Jan-Mar:6(1):8-16. doi: 10.4103/2231-0770.173580. Epub [PubMed PMID: 26955600]
McManus DD, Rienstra M, Benjamin EJ. An update on the prognosis of patients with atrial fibrillation. Circulation. 2012 Sep 4:126(10):e143-6. doi: 10.1161/CIRCULATIONAHA.112.129759. Epub [PubMed PMID: 22949543]
Mohanty S,Trivedi C,Gianni C,Natale A, Gender specific considerations in atrial fibrillation treatment: a review. Expert opinion on pharmacotherapy. 2018 Mar [PubMed PMID: 29424249]
Peters SAE, Woodward M. Established and novel risk factors for atrial fibrillation in women compared with men. Heart (British Cardiac Society). 2019 Feb:105(3):226-234. doi: 10.1136/heartjnl-2018-313630. Epub 2018 Aug 29 [PubMed PMID: 30158135]
Choi YJ, Choi EK, Han KD, Jung JH, Park J, Lee E, Choe W, Lee SR, Cha MJ, Lim WH, Oh S. Temporal trends of the prevalence and incidence of atrial fibrillation and stroke among Asian patients with hypertrophic cardiomyopathy: A nationwide population-based study. International journal of cardiology. 2018 Dec 15:273():130-135. doi: 10.1016/j.ijcard.2018.08.038. Epub 2018 Aug 11 [PubMed PMID: 30150122]
Robert R, Porot G, Vernay C, Buffet P, Fichot M, Guenancia C, Pommier T, Mouhat B, Cottin Y, Lorgis L. Incidence, Predictive Factors, and Prognostic Impact of Silent Atrial Fibrillation After Transcatheter Aortic Valve Implantation. The American journal of cardiology. 2018 Aug 1:122(3):446-454. doi: 10.1016/j.amjcard.2018.04.029. Epub 2018 May 1 [PubMed PMID: 30201110]
Tarride JE, Quinn FR, Blackhouse G, Sandhu RK, Burke N, Gladstone DJ, Ivers NM, Dolovich L, Thornton A, Nakamya J, Ramasundarahettige C, Frydrych PA, Henein S, Ng K, Congdon V, Birtwhistle RV, Ward R, Healey JS. Is Screening for Atrial Fibrillation in Canadian Family Practices Cost-Effective in Patients 65 Years and Older? The Canadian journal of cardiology. 2018 Nov:34(11):1522-1525. doi: 10.1016/j.cjca.2018.05.016. Epub 2018 Jun 21 [PubMed PMID: 30144961]
Karnad A, Pannelay A, Boshnakova A, Lovell AD, Cook RG. Stroke prevention in Europe: how are 11 European countries progressing toward the European Society of Cardiology (ESC) recommendations? Risk management and healthcare policy. 2018:11():117-125. doi: 10.2147/RMHP.S163439. Epub 2018 Aug 22 [PubMed PMID: 30197544]
Laäs DJ, Naidoo M. Oral anticoagulants and atrial fibrillation: A South African perspective. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 2018 Jul 25:108(8):640-646. doi: 10.7196/SAMJ.2018.v108i8.13309. Epub 2018 Jul 25 [PubMed PMID: 30182879]
Bai CJ, Madan N, Alshahrani S, Aggarwal NT, Volgman AS. Sex Differences in Atrial Fibrillation-Update on Risk Assessment, Treatment, and Long-Term Risk. Current treatment options in cardiovascular medicine. 2018 Aug 27:20(10):79. doi: 10.1007/s11936-018-0682-3. Epub 2018 Aug 27 [PubMed PMID: 30146677]
Brieger D, Amerena J, Attia JR, Bajorek B, Chan KH, Connell C, Freedman B, Ferguson C, Hall T, Haqqani HM, Hendriks J, Hespe CM, Hung J, Kalman JM, Sanders P, Worthington J, Yan T, Zwar NA. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. The Medical journal of Australia. 2018 Oct 15:209(8):356-362 [PubMed PMID: 30067936]
Pharithi RB, Ranganathan D, O'Brien J, Egom EE, Burke C, Ryan D, McAuliffe C, Vaughan M, Coughlan T, Morrissey E, McHugh J, Moore D, Collins R. Is the prescription right? A review of non-vitamin K antagonist anticoagulant (NOAC) prescriptions in patients with non-valvular atrial fibrillation. Safe prescribing in atrial fibrillation and evaluation of non-vitamin K oral anticoagulants in stroke prevention (SAFE-NOACS) group. Irish journal of medical science. 2019 Feb:188(1):101-108. doi: 10.1007/s11845-018-1837-7. Epub 2018 Jun 2 [PubMed PMID: 29860595]
Dan GA, Iliodromitis K, Scherr D, Marín F, Lenarczyk R, Estner HL, Kostkiewicz M, Dagres N, Lip GYH. Translating guidelines into practice for the management of atrial fibrillation: results of an European Heart Rhythm Association Survey. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2018 Aug 1:20(8):1382-1387. doi: 10.1093/europace/euy094. Epub [PubMed PMID: 29893840]