[1]
Aframian A, Smith TO, Tennent TD, Cobb JP, Hing CB. Origin and insertion of the medial patellofemoral ligament: a systematic review of anatomy. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2017 Dec:25(12):3755-3772. doi: 10.1007/s00167-016-4272-1. Epub 2016 Sep 8
[PubMed PMID: 27631645]
Level 1 (high-level) evidence
[2]
Bicos J, Fulkerson JP, Amis A. Current concepts review: the medial patellofemoral ligament. The American journal of sports medicine. 2007 Mar:35(3):484-92
[PubMed PMID: 17303819]
[3]
Guerrero P, Li X, Patel K, Brown M, Busconi B. Medial patellofemoral ligament injury patterns and associated pathology in lateral patella dislocation: an MRI study. Sports medicine, arthroscopy, rehabilitation, therapy & technology : SMARTT. 2009 Jul 30:1(1):17. doi: 10.1186/1758-2555-1-17. Epub 2009 Jul 30
[PubMed PMID: 19643022]
[4]
LaPrade MD, Kennedy MI, Wijdicks CA, LaPrade RF. Anatomy and biomechanics of the medial side of the knee and their surgical implications. Sports medicine and arthroscopy review. 2015 Jun:23(2):63-70. doi: 10.1097/JSA.0000000000000054. Epub
[PubMed PMID: 25932874]
[5]
Waligora AC, Johanson NA, Hirsch BE. Clinical anatomy of the quadriceps femoris and extensor apparatus of the knee. Clinical orthopaedics and related research. 2009 Dec:467(12):3297-306. doi: 10.1007/s11999-009-1052-y. Epub 2009 Aug 19
[PubMed PMID: 19690926]
[6]
Mérida-Velasco JA, Sánchez-Montesinos I, Espín-Ferra J, Rodríguez-Vázquez JF, Mérida-Velasco JR, Jiménez-Collado J. Development of the human knee joint. The Anatomical record. 1997 Jun:248(2):269-78
[PubMed PMID: 9185993]
[7]
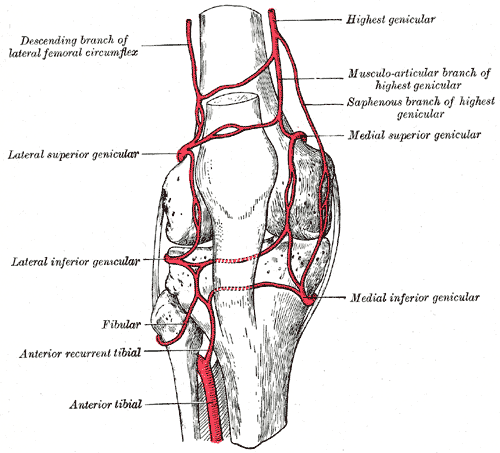
Shim SS, Leung G. Blood supply of the knee joint. A microangiographic study in children and adults. Clinical orthopaedics and related research. 1986 Jul:(208):119-25
[PubMed PMID: 3522019]
[8]
Tuxøe JI, Teir M, Winge S, Nielsen PL. The medial patellofemoral ligament: a dissection study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2002 May:10(3):138-40
[PubMed PMID: 12012030]
[9]
Lobenhoffer P, Biedert R, Stauffer E, Lattermann C, Gerich TG, Müller W. Occurrence and distribution of free nerve endings in the distal iliotibial tract system of the knee. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 1996:4(2):111-5
[PubMed PMID: 8884732]
[10]
Kittl C, Becker DK, Raschke MJ, Müller M, Wierer G, Domnick C, Glasbrenner J, Michel P, Herbort M. Dynamic Restraints of the Medial Side of the Knee: The Semimembranosus Corner Revisited. The American journal of sports medicine. 2019 Mar:47(4):863-869. doi: 10.1177/0363546519829384. Epub
[PubMed PMID: 30870030]
[11]
Miao P, Xu Y, Pan C, Liu H, Wang C. Vastus medialis oblique and vastus lateralis activity during a double-leg semisquat with or without hip adduction in patients with patellofemoral pain syndrome. BMC musculoskeletal disorders. 2015 Oct 12:16():289. doi: 10.1186/s12891-015-0736-6. Epub 2015 Oct 12
[PubMed PMID: 26459411]
[12]
Raoulis V, Fyllos A, Klontzas ME, Chytas D, Mitrousias V, Banios K, Maris TG, Karantanas AH, Zibis A. Surgical and Radiological Anatomy of the Medial Patellofemoral Ligament: A Magnetic Resonance Imaging and Cadaveric Study. Diagnostics (Basel, Switzerland). 2021 Nov 10:11(11):. doi: 10.3390/diagnostics11112076. Epub 2021 Nov 10
[PubMed PMID: 34829423]
[13]
Krebs C, Tranovich M, Andrews K, Ebraheim N. The medial patellofemoral ligament: Review of the literature. Journal of orthopaedics. 2018 Jun:15(2):596-599. doi: 10.1016/j.jor.2018.05.004. Epub 2018 May 7
[PubMed PMID: 29881201]
[14]
Schöttle PB, Schmeling A, Rosenstiel N, Weiler A. Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. The American journal of sports medicine. 2007 May:35(5):801-4
[PubMed PMID: 17267773]
[15]
Mistry JB, Bonner KF, Gwam CU, Thomas M, Etcheson JI, Delanois RE. Management of Injuries to the Medial Patellofemoral Ligament: A Review. The journal of knee surgery. 2018 May:31(5):439-447. doi: 10.1055/s-0037-1604142. Epub 2017 Jul 18
[PubMed PMID: 28719945]
[16]
Duchman KR, Bollier MJ. The Role of Medial Patellofemoral Ligament Repair and Imbrication. American journal of orthopedics (Belle Mead, N.J.). 2017 Mar/Apr:46(2):87-91
[PubMed PMID: 28437493]
[17]
Aliberti GM, Kraeutler MJ, Miskimin C, Scillia AJ, Belk JW, Mulcahey MK. Autograft Versus Allograft for Medial Patellofemoral Ligament Reconstruction: A Systematic Review. Orthopaedic journal of sports medicine. 2021 Oct:9(10):23259671211046639. doi: 10.1177/23259671211046639. Epub 2021 Oct 19
[PubMed PMID: 34692883]
Level 1 (high-level) evidence
[18]
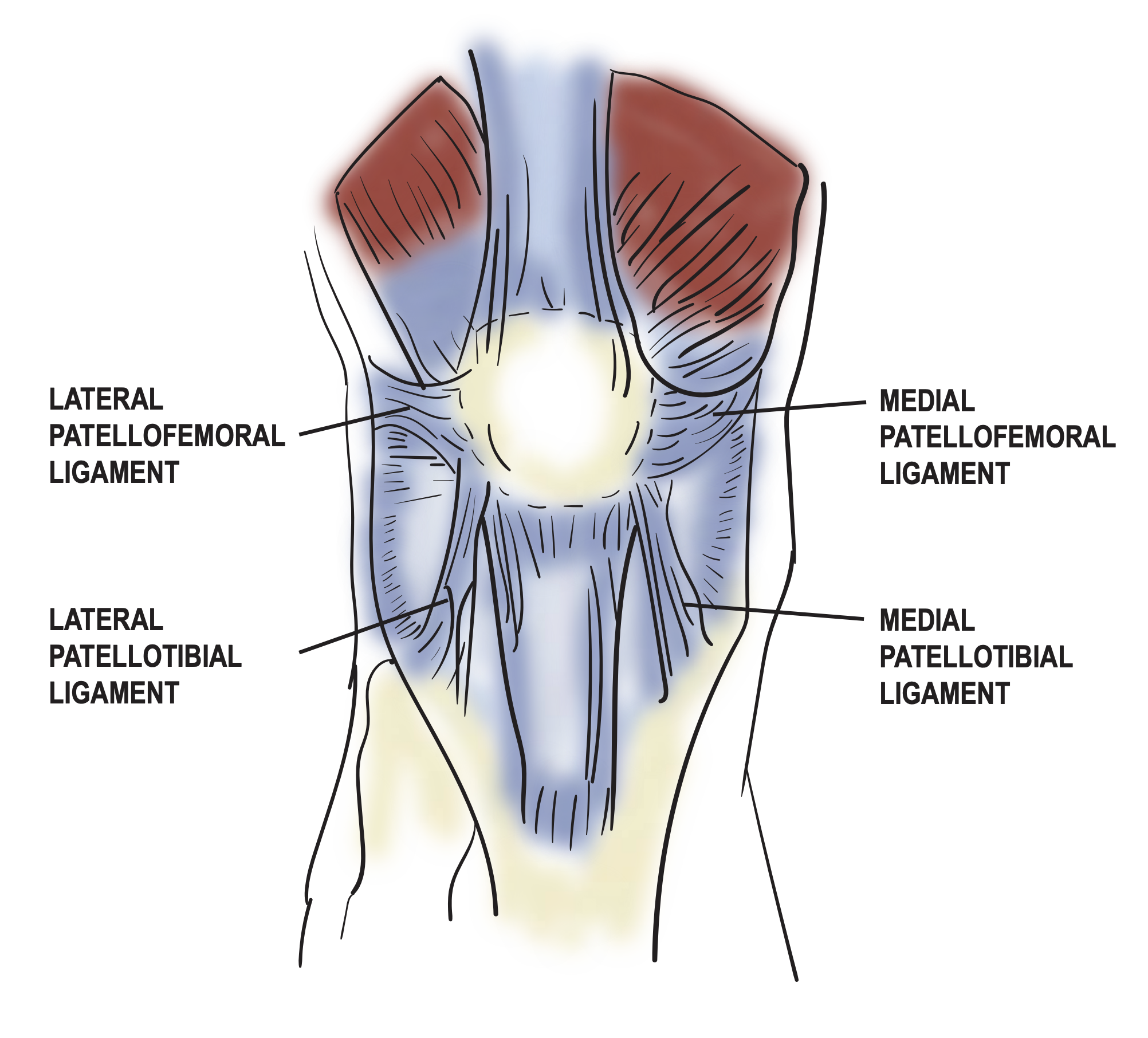
Kruckeberg BM, Chahla J, Moatshe G, Cinque ME, Muckenhirn KJ, Godin JA, Ridley TJ, Brady AW, Arendt EA, LaPrade RF. Quantitative and Qualitative Analysis of the Medial Patellar Ligaments: An Anatomic and Radiographic Study. The American journal of sports medicine. 2018 Jan:46(1):153-162. doi: 10.1177/0363546517729818. Epub 2017 Oct 10
[PubMed PMID: 29016187]
Level 2 (mid-level) evidence
[19]
Mizuno Y,Kumagai M,Mattessich SM,Elias JJ,Ramrattan N,Cosgarea AJ,Chao EY, Q-angle influences tibiofemoral and patellofemoral kinematics. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2001 Sep;
[PubMed PMID: 11562129]
[20]
Hall MJ, Mandalia VI. Tibial tubercle osteotomy for patello-femoral joint disorders. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2016 Mar:24(3):855-61. doi: 10.1007/s00167-014-3388-4. Epub 2014 Oct 19
[PubMed PMID: 25326765]
[21]
Hensler D, Sillanpaa PJ, Schoettle PB. Medial patellofemoral ligament: anatomy, injury and treatment in the adolescent knee. Current opinion in pediatrics. 2014 Feb:26(1):70-8. doi: 10.1097/MOP.0000000000000055. Epub
[PubMed PMID: 24362407]
Level 3 (low-level) evidence