[1]
Apfelbaum JL,Hagberg CA,Caplan RA,Blitt CD,Connis RT,Nickinovich DG,Hagberg CA,Caplan RA,Benumof JL,Berry FA,Blitt CD,Bode RH,Cheney FW,Connis RT,Guidry OF,Nickinovich DG,Ovassapian A,American Society of Anesthesiologists Task Force on Management of the Difficult Airway., Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013 Feb;
[PubMed PMID: 23364566]
Level 1 (high-level) evidence
[2]
Cook TM,Woodall N,Frerk C,Fourth National Audit Project., Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. British journal of anaesthesia. 2011 May;
[PubMed PMID: 21447488]
[3]
Joffe AM,Aziz MF,Posner KL,Duggan LV,Mincer SL,Domino KB, Management of Difficult Tracheal Intubation: A Closed Claims Analysis. Anesthesiology. 2019 Oct;
[PubMed PMID: 31584884]
[4]
Nørskov AK, Preoperative airway assessment - experience gained from a multicentre cluster randomised trial and the Danish Anaesthesia Database. Danish medical journal. 2016 May;
[PubMed PMID: 27127020]
Level 1 (high-level) evidence
[5]
Cook TM,Woodall N,Harper J,Benger J,Fourth National Audit Project., Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. British journal of anaesthesia. 2011 May;
[PubMed PMID: 21447489]
[6]
Schiff JH,Welker A,Fohr B,Henn-Beilharz A,Bothner U,Van Aken H,Schleppers A,Baldering HJ,Heinrichs W, Major incidents and complications in otherwise healthy patients undergoing elective procedures: results based on 1.37 million anaesthetic procedures. British journal of anaesthesia. 2014 Jul;
[PubMed PMID: 24801456]
[7]
Mosier JM,Joshi R,Hypes C,Pacheco G,Valenzuela T,Sakles JC, The Physiologically Difficult Airway. The western journal of emergency medicine. 2015 Dec
[PubMed PMID: 26759664]
[8]
Kornas RL,Owyang CG,Sakles JC,Foley LJ,Mosier JM,Society for Airway Management’s Special Projects Committee., Evaluation and Management of the Physiologically Difficult Airway: Consensus Recommendations From Society for Airway Management. Anesthesia and analgesia. 2021 Feb 1
[PubMed PMID: 33060492]
Level 3 (low-level) evidence
[10]
Kinsella SM,Winton AL,Mushambi MC,Ramaswamy K,Swales H,Quinn AC,Popat M, Failed tracheal intubation during obstetric general anaesthesia: a literature review. International journal of obstetric anesthesia. 2015 Nov;
[PubMed PMID: 26303751]
[11]
Mushambi MC,Kinsella SM,Popat M,Swales H,Ramaswamy KK,Winton AL,Quinn AC,Obstetric Anaesthetists' Association.,Difficult Airway Society., Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia. 2015 Nov;
[PubMed PMID: 26449292]
[12]
Austin N,Krishnamoorthy V,Dagal A, Airway management in cervical spine injury. International journal of critical illness and injury science. 2014 Jan;
[PubMed PMID: 24741498]
[15]
Wong DT,Dallaire A,Singh KP,Madhusudan P,Jackson T,Singh M,Wong J,Chung F, High-Flow Nasal Oxygen Improves Safe Apnea Time in Morbidly Obese Patients Undergoing General Anesthesia: A Randomized Controlled Trial. Anesthesia and analgesia. 2019 Oct;
[PubMed PMID: 31584919]
Level 1 (high-level) evidence
[16]
Gleason JM,Christian BR,Barton ED, Nasal Cannula Apneic Oxygenation Prevents Desaturation During Endotracheal Intubation: An Integrative Literature Review. The western journal of emergency medicine. 2018 Mar;
[PubMed PMID: 29560073]
[17]
Ramachandran SK,Cosnowski A,Shanks A,Turner CR, Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration. Journal of clinical anesthesia. 2010 May;
[PubMed PMID: 20400000]
Level 1 (high-level) evidence
[18]
Weingart SD,Levitan RM, Preoxygenation and prevention of desaturation during emergency airway management. Annals of emergency medicine. 2012 Mar;
[PubMed PMID: 22050948]
[19]
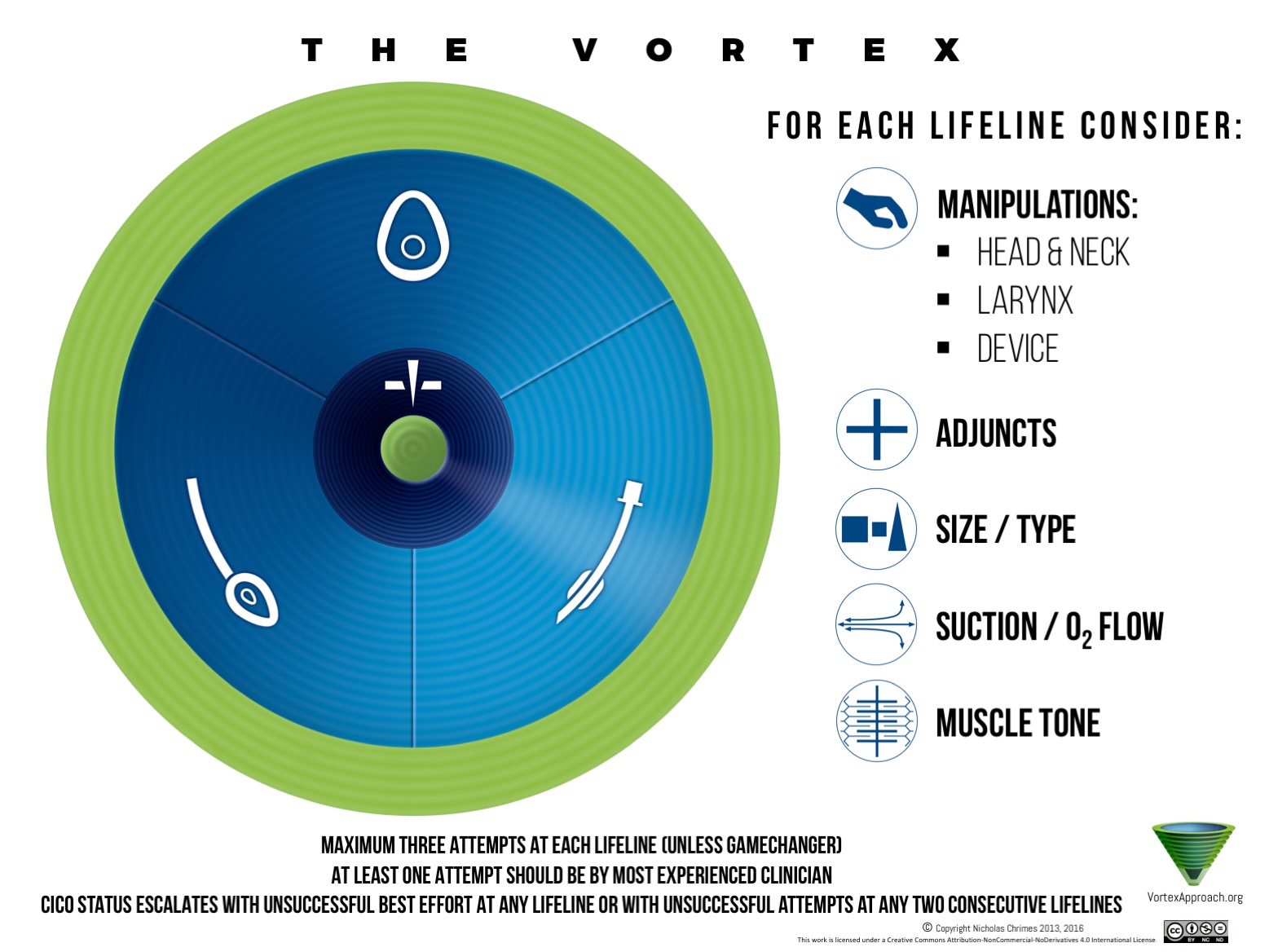
Charco-Mora P,Urtubia R,Reviriego-Agudo L, The Vortex model: A different approach to the difficult airway. Revista espanola de anestesiologia y reanimacion. 2018 Aug - Sep;
[PubMed PMID: 30037388]
[20]
Ikeda A,Isono S,Sato Y,Yogo H,Sato J,Ishikawa T,Nishino T, Effects of muscle relaxants on mask ventilation in anesthetized persons with normal upper airway anatomy. Anesthesiology. 2012 Sep
[PubMed PMID: 22846679]
[21]
Priebe HJ, Could 'safe practice' be compromising safe practice? Should anaesthetists have to demonstrate that face mask ventilation is possible before giving a neuromuscular blocker? Anaesthesia. 2008 Jun;
[PubMed PMID: 18477282]
[22]
Henderson JJ,Popat MT,Latto IP,Pearce AC,Difficult Airway Society., Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia. 2004 Jul;
[PubMed PMID: 15200543]
[23]
Goto T,Watase H,Morita H,Nagai H,Brown CA 3rd,Brown DF,Hasegawa K,Japanese Emergency Medicine Network Investigators., Repeated attempts at tracheal intubation by a single intubator associated with decreased success rates in emergency departments: an analysis of a multicentre prospective observational study. Emergency medicine journal : EMJ. 2015 Oct;
[PubMed PMID: 25552546]
Level 2 (mid-level) evidence
[24]
Li T,Jafari D,Meyer C,Voroba A,Haddad G,Abecassis S,Bank M,Dym A,Naqvi A,Gujral R,Rolston D, Video laryngoscopy is associated with improved first-pass intubation success compared with direct laryngoscopy in emergency department trauma patients. Journal of the American College of Emergency Physicians open. 2021 Feb;
[PubMed PMID: 33532760]
[25]
Law JA,Broemling N,Cooper RM,Drolet P,Duggan LV,Griesdale DE,Hung OR,Jones PM,Kovacs G,Massey S,Morris IR,Mullen T,Murphy MF,Preston R,Naik VN,Scott J,Stacey S,Turkstra TP,Wong DT,Canadian Airway Focus Group., The difficult airway with recommendations for management--part 1--difficult tracheal intubation encountered in an unconscious/induced patient. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2013 Nov;
[PubMed PMID: 24132407]
[26]
Foley LJ, Urdaneta F, Berkow L, Aziz MF, Baker PA, Jagannathan N, Rosenblatt W, Straker TM, Wong DT, Hagberg CA. Difficult Airway Management in Adult Coronavirus Disease 2019 Patients: Statement by the Society of Airway Management. Anesthesia and analgesia. 2021 Oct 1:133(4):876-890. doi: 10.1213/ANE.0000000000005554. Epub
[PubMed PMID: 33711004]
[27]
Brozek T,Bruthans J,Porizka M,Blaha J,Ulrichova J,Michalek P, A Randomized Comparison of Non-Channeled Glidescope{sup}TM{/sup} Titanium Versus Channeled KingVision{sup}TM{/sup} Videolaryngoscope for Orotracheal Intubation in Obese Patients with BMI > 35 kg·m{sup}-2{/sup}. Diagnostics (Basel, Switzerland). 2020 Nov 29
[PubMed PMID: 33260374]
Level 1 (high-level) evidence
[28]
Gerstein NS,Braude DA,Hung O,Sanders JC,Murphy MF, The Fastrach Intubating Laryngeal Mask Airway: an overview and update. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2010 Jun;
[PubMed PMID: 20112078]
Level 3 (low-level) evidence
[29]
Ovassapian A,Glassenberg R,Randel GI,Klock A,Mesnick PS,Klafta JM, The unexpected difficult airway and lingual tonsil hyperplasia: a case series and a review of the literature. Anesthesiology. 2002 Jul;
[PubMed PMID: 12131113]
Level 2 (mid-level) evidence
[30]
Roth D, Pace NL, Lee A, Hovhannisyan K, Warenits AM, Arrich J, Herkner H. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. The Cochrane database of systematic reviews. 2018 May 15:5(5):CD008874. doi: 10.1002/14651858.CD008874.pub2. Epub 2018 May 15
[PubMed PMID: 29761867]
Level 1 (high-level) evidence
[31]
Detsky ME, Jivraj N, Adhikari NK, Friedrich JO, Pinto R, Simel DL, Wijeysundera DN, Scales DC. Will This Patient Be Difficult to Intubate?: The Rational Clinical Examination Systematic Review. JAMA. 2019 Feb 5:321(5):493-503. doi: 10.1001/jama.2018.21413. Epub
[PubMed PMID: 30721300]
Level 1 (high-level) evidence
[33]
Flin R,Fioratou E,Frerk C,Trotter C,Cook TM, Human factors in the development of complications of airway management: preliminary evaluation of an interview tool. Anaesthesia. 2013 Aug;
[PubMed PMID: 23682749]
Level 3 (low-level) evidence
[34]
Schulz CM,Burden A,Posner KL,Mincer SL,Steadman R,Wagner KJ,Domino KB, Frequency and Type of Situational Awareness Errors Contributing to Death and Brain Damage: A Closed Claims Analysis. Anesthesiology. 2017 Aug;
[PubMed PMID: 28459735]