[1]
Stewart EEM, Valsecchi M, Schütz AC. A review of interactions between peripheral and foveal vision. Journal of vision. 2020 Nov 2:20(12):2. doi: 10.1167/jov.20.12.2. Epub
[PubMed PMID: 33141171]
[2]
Friedman DS, O'Colmain BJ, Muñoz B, Tomany SC, McCarty C, de Jong PT, Nemesure B, Mitchell P, Kempen J, Eye Diseases Prevalence Research Group. Prevalence of age-related macular degeneration in the United States. Archives of ophthalmology (Chicago, Ill. : 1960). 2004 Apr:122(4):564-72
[PubMed PMID: 15078675]
[3]
Spraul CW, Lang GE, Grossniklaus HE, Lang GK. Histologic and morphometric analysis of the choroid, Bruch's membrane, and retinal pigment epithelium in postmortem eyes with age-related macular degeneration and histologic examination of surgically excised choroidal neovascular membranes. Survey of ophthalmology. 1999 Oct:44 Suppl 1():S10-32
[PubMed PMID: 10548114]
Level 3 (low-level) evidence
[4]
Ba J, Peng RS, Xu D, Li YH, Shi H, Wang Q, Yu J. Intravitreal anti-VEGF injections for treating wet age-related macular degeneration: a systematic review and meta-analysis. Drug design, development and therapy. 2015:9():5397-405. doi: 10.2147/DDDT.S86269. Epub 2015 Sep 28
[PubMed PMID: 26451092]
Level 1 (high-level) evidence
[5]
Chew EY, Clemons TE, Agrón E, Sperduto RD, Sangiovanni JP, Davis MD, Ferris FL 3rd, Age-Related Eye Disease Study Research Group. Ten-year follow-up of age-related macular degeneration in the age-related eye disease study: AREDS report no. 36. JAMA ophthalmology. 2014 Mar:132(3):272-7. doi: 10.1001/jamaophthalmol.2013.6636. Epub
[PubMed PMID: 24385141]
[6]
Tomany SC, Wang JJ, Van Leeuwen R, Klein R, Mitchell P, Vingerling JR, Klein BE, Smith W, De Jong PT. Risk factors for incident age-related macular degeneration: pooled findings from 3 continents. Ophthalmology. 2004 Jul:111(7):1280-7
[PubMed PMID: 15234127]
[7]
Katsi VK, Marketou ME, Vrachatis DA, Manolis AJ, Nihoyannopoulos P, Tousoulis D, Vardas PE, Kallikazaros I. Essential hypertension in the pathogenesis of age-related macular degeneration: a review of the current evidence. Journal of hypertension. 2015 Dec:33(12):2382-8. doi: 10.1097/HJH.0000000000000766. Epub
[PubMed PMID: 26536087]
[8]
Black JR, Clark SJ. Age-related macular degeneration: genome-wide association studies to translation. Genetics in medicine : official journal of the American College of Medical Genetics. 2016 Apr:18(4):283-9. doi: 10.1038/gim.2015.70. Epub 2015 May 28
[PubMed PMID: 26020418]
[9]
Kauppinen A, Paterno JJ, Blasiak J, Salminen A, Kaarniranta K. Inflammation and its role in age-related macular degeneration. Cellular and molecular life sciences : CMLS. 2016 May:73(9):1765-86. doi: 10.1007/s00018-016-2147-8. Epub 2016 Feb 6
[PubMed PMID: 26852158]
[10]
Schultz DW, Klein ML, Humpert AJ, Luzier CW, Persun V, Schain M, Mahan A, Runckel C, Cassera M, Vittal V, Doyle TM, Martin TM, Weleber RG, Francis PJ, Acott TS. Analysis of the ARMD1 locus: evidence that a mutation in HEMICENTIN-1 is associated with age-related macular degeneration in a large family. Human molecular genetics. 2003 Dec 15:12(24):3315-23
[PubMed PMID: 14570714]
[11]
Wong WL, Su X, Li X, Cheung CM, Klein R, Cheng CY, Wong TY. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. The Lancet. Global health. 2014 Feb:2(2):e106-16. doi: 10.1016/S2214-109X(13)70145-1. Epub 2014 Jan 3
[PubMed PMID: 25104651]
Level 1 (high-level) evidence
[12]
Jonas JB, Cheung CMG, Panda-Jonas S. Updates on the Epidemiology of Age-Related Macular Degeneration. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2017 Nov-Dec:6(6):493-497. doi: 10.22608/APO.2017251. Epub 2017 Sep 14
[PubMed PMID: 28906084]
[13]
Gehrs KM, Anderson DH, Johnson LV, Hageman GS. Age-related macular degeneration--emerging pathogenetic and therapeutic concepts. Annals of medicine. 2006:38(7):450-71
[PubMed PMID: 17101537]
[14]
Ferris FL 3rd, Fine SL, Hyman L. Age-related macular degeneration and blindness due to neovascular maculopathy. Archives of ophthalmology (Chicago, Ill. : 1960). 1984 Nov:102(11):1640-2
[PubMed PMID: 6208888]
[15]
Green WR, Enger C. Age-related macular degeneration histopathologic studies. The 1992 Lorenz E. Zimmerman Lecture. Ophthalmology. 1993 Oct:100(10):1519-35
[PubMed PMID: 7692366]
[16]
Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP. Age-related macular degeneration: etiology, pathogenesis, and therapeutic strategies. Survey of ophthalmology. 2003 May-Jun:48(3):257-93
[PubMed PMID: 12745003]
Level 3 (low-level) evidence
[17]
Gass JD. Biomicroscopic and histopathologic considerations regarding the feasibility of surgical excision of subfoveal neovascular membranes. American journal of ophthalmology. 1994 Sep 15:118(3):285-98
[PubMed PMID: 7521987]
Level 2 (mid-level) evidence
[18]
Shaimov TB, Panova IE, Shaimov RB, Shaimovа VA, Shai Mova TA, Fomin AV, Shaimov TB, Panova IE, Shaimov RB, Shaimova VA, Shaimova TA, Fomin AV. [Optical coherence tomography angiography in the diagnosis of neovascular age-related macular degeneration]. Vestnik oftalmologii. 2015 Sep-Oct:131(5):4-13. doi: 10.17116/oftalma201513154-12. Epub
[PubMed PMID: 26845866]
[19]
Freund KB, Ho IV, Barbazetto IA, Koizumi H, Laud K, Ferrara D, Matsumoto Y, Sorenson JA, Yannuzzi L. Type 3 neovascularization: the expanded spectrum of retinal angiomatous proliferation. Retina (Philadelphia, Pa.). 2008 Feb:28(2):201-11. doi: 10.1097/IAE.0b013e3181669504. Epub
[PubMed PMID: 18301024]
[20]
Yannuzzi LA, Freund KB, Takahashi BS. Review of retinal angiomatous proliferation or type 3 neovascularization. Retina (Philadelphia, Pa.). 2008 Mar:28(3):375-84. doi: 10.1097/IAE.0b013e3181619c55. Epub
[PubMed PMID: 18327130]
[21]
Spaide RF, Jaffe GJ, Sarraf D, Freund KB, Sadda SR, Staurenghi G, Waheed NK, Chakravarthy U, Rosenfeld PJ, Holz FG, Souied EH, Cohen SY, Querques G, Ohno-Matsui K, Boyer D, Gaudric A, Blodi B, Baumal CR, Li X, Coscas GJ, Brucker A, Singerman L, Luthert P, Schmitz-Valckenberg S, Schmidt-Erfurth U, Grossniklaus HE, Wilson DJ, Guymer R, Yannuzzi LA, Chew EY, Csaky K, Monés JM, Pauleikhoff D, Tadayoni R, Fujimoto J. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology. 2020 May:127(5):616-636. doi: 10.1016/j.ophtha.2019.11.004. Epub 2019 Nov 14
[PubMed PMID: 31864668]
Level 3 (low-level) evidence
[22]
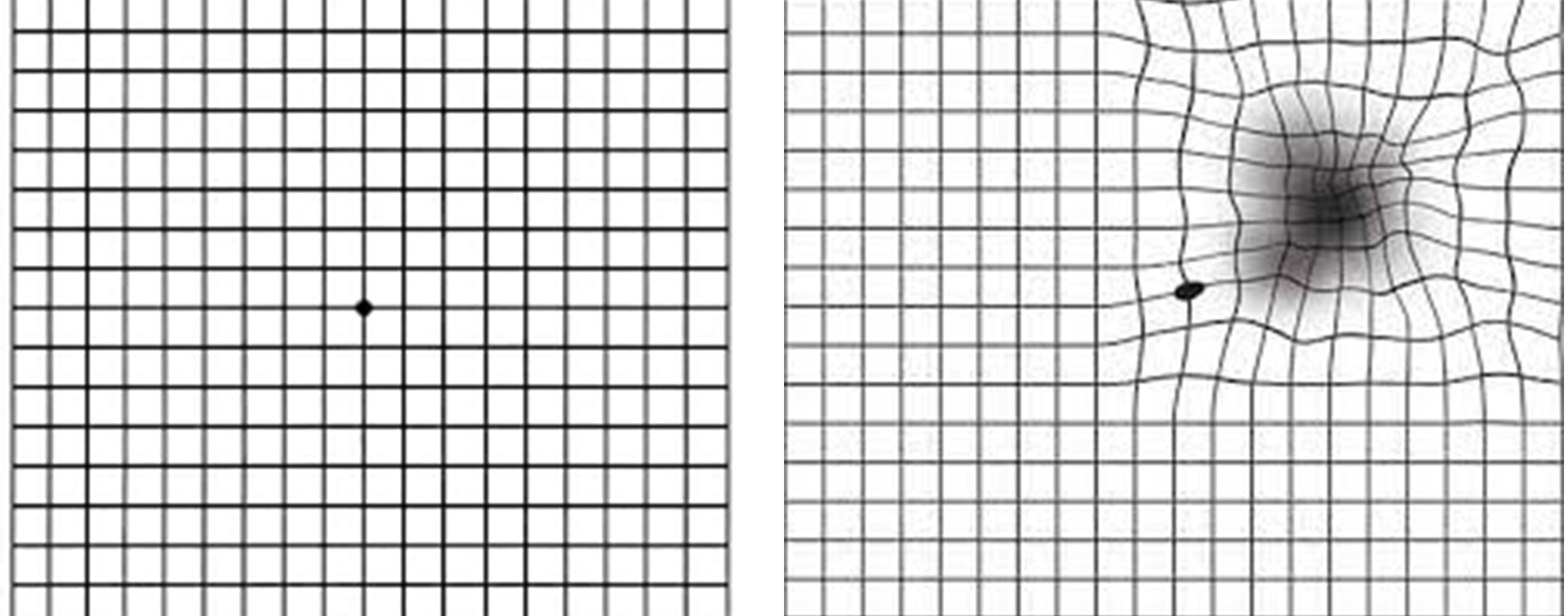
Fine AM, Elman MJ, Ebert JE, Prestia PA, Starr JS, Fine SL. Earliest symptoms caused by neovascular membranes in the macula. Archives of ophthalmology (Chicago, Ill. : 1960). 1986 Apr:104(4):513-4
[PubMed PMID: 2420316]
[23]
Bressler NM, Bressler SB, Gragoudas ES. Clinical characteristics of choroidal neovascular membranes. Archives of ophthalmology (Chicago, Ill. : 1960). 1987 Feb:105(2):209-13
[PubMed PMID: 2434067]
[24]
Zayit-Soudry S, Moroz I, Loewenstein A. Retinal pigment epithelial detachment. Survey of ophthalmology. 2007 May-Jun:52(3):227-43
[PubMed PMID: 17472800]
Level 3 (low-level) evidence
[25]
Gass JD. Serous retinal pigment epithelial detachment with a notch. A sign of occult choroidal neovascularization. Retina (Philadelphia, Pa.). 1984 Fall-Winter:4(4):205-20
[PubMed PMID: 6085179]
[26]
Tripathy K,Chawla R,Kumar V,Sharma YR,Venkatesh P, A 56-year-old male with unilateral painless diminution of vision. Oman journal of ophthalmology. 2016 May-Aug
[PubMed PMID: 27433043]
[27]
Drexler W, Fujimoto JG. State-of-the-art retinal optical coherence tomography. Progress in retinal and eye research. 2008 Jan:27(1):45-88
[PubMed PMID: 18036865]
[28]
Spaide RF. Enhanced depth imaging optical coherence tomography of retinal pigment epithelial detachment in age-related macular degeneration. American journal of ophthalmology. 2009 Apr:147(4):644-52. doi: 10.1016/j.ajo.2008.10.005. Epub 2009 Jan 18
[PubMed PMID: 19152869]
[29]
Chang LK, Sarraf D. Tears of the retinal pigment epithelium: an old problem in a new era. Retina (Philadelphia, Pa.). 2007 Jun:27(5):523-34
[PubMed PMID: 17558312]
[30]
Landa G, Su E, Garcia PM, Seiple WH, Rosen RB. Inner segment-outer segment junctional layer integrity and corresponding retinal sensitivity in dry and wet forms of age-related macular degeneration. Retina (Philadelphia, Pa.). 2011 Feb:31(2):364-70. doi: 10.1097/IAE.0b013e3181e91132. Epub
[PubMed PMID: 21221051]
[31]
Jia Y, Tan O, Tokayer J, Potsaid B, Wang Y, Liu JJ, Kraus MF, Subhash H, Fujimoto JG, Hornegger J, Huang D. Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Optics express. 2012 Feb 13:20(4):4710-25. doi: 10.1364/OE.20.004710. Epub
[PubMed PMID: 22418228]
[32]
Ma J, Desai R, Nesper P, Gill M, Fawzi A, Skondra D. Optical Coherence Tomographic Angiography Imaging in Age-Related Macular Degeneration. Ophthalmology and eye diseases. 2017:9():1179172116686075. doi: 10.1177/1179172116686075. Epub 2017 Mar 20
[PubMed PMID: 28579843]
[34]
Castillo MM, Mowatt G, Elders A, Lois N, Fraser C, Hernández R, Amoaku W, Burr JM, Lotery A, Ramsay CR, Azuara-Blanco A. Optical coherence tomography for the monitoring of neovascular age-related macular degeneration: a systematic review. Ophthalmology. 2015 Feb:122(2):399-406. doi: 10.1016/j.ophtha.2014.07.055. Epub 2014 Oct 22
[PubMed PMID: 25444343]
Level 1 (high-level) evidence
[35]
Schachat AP, Thompson JT. Optical coherence tomography, fluorescein angiography, and the management of neovascular age-related macular degeneration. Ophthalmology. 2015 Feb:122(2):222-3. doi: 10.1016/j.ophtha.2014.09.015. Epub
[PubMed PMID: 25618425]
[36]
Barbazetto I, Burdan A, Bressler NM, Bressler SB, Haynes L, Kapetanios AD, Lukas J, Olsen K, Potter M, Reaves A, Rosenfeld P, Schachat AP, Strong HA, Wenkstern A, Treatment of Age-Related Macular Degeneration with Photodynamic Therapy Study Group, Verteporfin in Photodynamic Therapy Study Group. Photodynamic therapy of subfoveal choroidal neovascularization with verteporfin: fluorescein angiographic guidelines for evaluation and treatment--TAP and VIP report No. 2. Archives of ophthalmology (Chicago, Ill. : 1960). 2003 Sep:121(9):1253-68
[PubMed PMID: 12963608]
[37]
. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1999 Oct:117(10):1329-45
[PubMed PMID: 10532441]
Level 1 (high-level) evidence
[38]
Dyer DS, Brant AM, Schachat AP, Bressler SB, Bressler NM. Angiographic features and outcome of questionable recurrent choroidal neovascularization. American journal of ophthalmology. 1995 Oct:120(4):497-505
[PubMed PMID: 7573308]
[39]
Chuang EL, Bird AC. The pathogenesis of tears of the retinal pigment epithelium. American journal of ophthalmology. 1988 Mar 15:105(3):285-90
[PubMed PMID: 2449819]
[41]
Regillo CD, Benson WE, Maguire JI, Annesley WH Jr. Indocyanine green angiography and occult choroidal neovascularization. Ophthalmology. 1994 Feb:101(2):280-8
[PubMed PMID: 7509471]
[42]
Bottoni F, Massacesi A, Cigada M, Viola F, Musicco I, Staurenghi G. Treatment of retinal angiomatous proliferation in age-related macular degeneration: a series of 104 cases of retinal angiomatous proliferation. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Dec:123(12):1644-50
[PubMed PMID: 16344434]
Level 3 (low-level) evidence
[43]
Koh A, Lee WK, Chen LJ, Chen SJ, Hashad Y, Kim H, Lai TY, Pilz S, Ruamviboonsuk P, Tokaji E, Weisberger A, Lim TH. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina (Philadelphia, Pa.). 2012 Sep:32(8):1453-64
[PubMed PMID: 22426346]
[44]
Saito M, Iida T, Kano M, Itagaki K. Angiographic results of retinal-retinal anastomosis and retinal-choroidal anastomosis after treatments in eyes with retinal angiomatous proliferation. Clinical ophthalmology (Auckland, N.Z.). 2012:6():1385-91. doi: 10.2147/OPTH.S36333. Epub 2012 Aug 28
[PubMed PMID: 22969283]
[45]
Kaiser SM, Arepalli S, Ehlers JP. Current and Future Anti-VEGF Agents for Neovascular Age-Related Macular Degeneration. Journal of experimental pharmacology. 2021:13():905-912. doi: 10.2147/JEP.S259298. Epub 2021 Sep 29
[PubMed PMID: 34616189]
[46]
VEGF Inhibition Study in Ocular Neovascularization (V.I.S.I.O.N.) Clinical Trial Group, D'Amico DJ, Masonson HN, Patel M, Adamis AP, Cunningham ET Jr, Guyer DR, Katz B. Pegaptanib sodium for neovascular age-related macular degeneration: two-year safety results of the two prospective, multicenter, controlled clinical trials. Ophthalmology. 2006 Jun:113(6):992-1001.e6
[PubMed PMID: 16647134]
Level 1 (high-level) evidence
[47]
CATT Research Group, Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. The New England journal of medicine. 2011 May 19:364(20):1897-908. doi: 10.1056/NEJMoa1102673. Epub 2011 Apr 28
[PubMed PMID: 21526923]
[48]
Brown DM, Kaiser PK, Michels M, Soubrane G, Heier JS, Kim RY, Sy JP, Schneider S, ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. The New England journal of medicine. 2006 Oct 5:355(14):1432-44
[PubMed PMID: 17021319]
[49]
Heier JS, Brown DM, Chong V, Korobelnik JF, Kaiser PK, Nguyen QD, Kirchhof B, Ho A, Ogura Y, Yancopoulos GD, Stahl N, Vitti R, Berliner AJ, Soo Y, Anderesi M, Groetzbach G, Sommerauer B, Sandbrink R, Simader C, Schmidt-Erfurth U, VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012 Dec:119(12):2537-48. doi: 10.1016/j.ophtha.2012.09.006. Epub 2012 Oct 17
[PubMed PMID: 23084240]
[50]
Gragoudas ES, Adamis AP, Cunningham ET Jr, Feinsod M, Guyer DR, VEGF Inhibition Study in Ocular Neovascularization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. The New England journal of medicine. 2004 Dec 30:351(27):2805-16
[PubMed PMID: 15625332]
[51]
Rosenfeld PJ, Brown DM, Heier JS, Boyer DS, Kaiser PK, Chung CY, Kim RY, MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. The New England journal of medicine. 2006 Oct 5:355(14):1419-31
[PubMed PMID: 17021318]
[52]
Kumar A,Tripathy K,Chawla R, Intraocular use of bevacizumab in India: An issue resolved? The National medical journal of India. 2017 Nov-Dec;
[PubMed PMID: 30117450]
[53]
Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, Toth C, Redford M, Ferris FL 3rd. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012 Jul:119(7):1388-98. doi: 10.1016/j.ophtha.2012.03.053. Epub 2012 May 1
[PubMed PMID: 22555112]
[54]
IVAN Study Investigators, Chakravarthy U, Harding SP, Rogers CA, Downes SM, Lotery AJ, Wordsworth S, Reeves BC. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: one-year findings from the IVAN randomized trial. Ophthalmology. 2012 Jul:119(7):1399-411. doi: 10.1016/j.ophtha.2012.04.015. Epub 2012 May 11
[PubMed PMID: 22578446]
Level 1 (high-level) evidence
[55]
Kodjikian L, Souied EH, Mimoun G, Mauget-Faÿsse M, Behar-Cohen F, Decullier E, Huot L, Aulagner G, GEFAL Study Group. Ranibizumab versus Bevacizumab for Neovascular Age-related Macular Degeneration: Results from the GEFAL Noninferiority Randomized Trial. Ophthalmology. 2013 Nov:120(11):2300-9. doi: 10.1016/j.ophtha.2013.06.020. Epub 2013 Aug 2
[PubMed PMID: 23916488]
Level 1 (high-level) evidence
[56]
Berg K, Pedersen TR, Sandvik L, Bragadóttir R. Comparison of ranibizumab and bevacizumab for neovascular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology. 2015 Jan:122(1):146-52. doi: 10.1016/j.ophtha.2014.07.041. Epub 2014 Sep 13
[PubMed PMID: 25227499]
[57]
Schauwvlieghe AM, Dijkman G, Hooymans JM, Verbraak FD, Hoyng CB, Dijkgraaf MG, Peto T, Vingerling JR, Schlingemann RO. Comparing the Effectiveness of Bevacizumab to Ranibizumab in Patients with Exudative Age-Related Macular Degeneration. The BRAMD Study. PloS one. 2016:11(5):e0153052. doi: 10.1371/journal.pone.0153052. Epub 2016 May 20
[PubMed PMID: 27203434]
[58]
Krebs I, Schmetterer L, Boltz A, Told R, Vécsei-Marlovits V, Egger S, Schönherr U, Haas A, Ansari-Shahrezaei S, Binder S, MANTA Research Group. A randomised double-masked trial comparing the visual outcome after treatment with ranibizumab or bevacizumab in patients with neovascular age-related macular degeneration. The British journal of ophthalmology. 2013 Mar:97(3):266-71. doi: 10.1136/bjophthalmol-2012-302391. Epub 2013 Jan 3
[PubMed PMID: 23292928]
Level 1 (high-level) evidence
[59]
Wu B, Wu H, Liu X, Lin H, Li J. Ranibizumab versus bevacizumab for ophthalmic diseases related to neovascularisation: a meta-analysis of randomised controlled trials. PloS one. 2014:9(7):e101253. doi: 10.1371/journal.pone.0101253. Epub 2014 Jul 1
[PubMed PMID: 24983855]
Level 1 (high-level) evidence
[60]
Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, Brown DM, Chong V, Nguyen QD, Ho AC, Ogura Y, Simader C, Jaffe GJ, Slakter JS, Yancopoulos GD, Stahl N, Vitti R, Berliner AJ, Soo Y, Anderesi M, Sowade O, Zeitz O, Norenberg C, Sandbrink R, Heier JS. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014 Jan:121(1):193-201. doi: 10.1016/j.ophtha.2013.08.011. Epub 2013 Sep 29
[PubMed PMID: 24084500]
[61]
Dixon JA, Oliver SC, Olson JL, Mandava N. VEGF Trap-Eye for the treatment of neovascular age-related macular degeneration. Expert opinion on investigational drugs. 2009 Oct:18(10):1573-80. doi: 10.1517/13543780903201684. Epub
[PubMed PMID: 19694600]
Level 3 (low-level) evidence
[62]
Heier JS, Boyer D, Nguyen QD, Marcus D, Roth DB, Yancopoulos G, Stahl N, Ingerman A, Vitti R, Berliner AJ, Yang K, Brown DM, CLEAR-IT 2 Investigators. The 1-year results of CLEAR-IT 2, a phase 2 study of vascular endothelial growth factor trap-eye dosed as-needed after 12-week fixed dosing. Ophthalmology. 2011 Jun:118(6):1098-106. doi: 10.1016/j.ophtha.2011.03.020. Epub
[PubMed PMID: 21640258]
[63]
Kim E, Han J, Chae Y, Park H, Kim S, Kim S, Lee J, Kim BC. Evaluation of the Structural, Physicochemical, and Biological Characteristics of SB11, as Lucentis(®) (Ranibizumab) Biosimilar. Ophthalmology and therapy. 2022 Apr:11(2):639-652. doi: 10.1007/s40123-022-00453-7. Epub 2022 Jan 27
[PubMed PMID: 35084693]
[64]
Sharma A, Kondo M, Iwahashi C, Parachuri N, Kumar N, Bandello F, Loewenstein A, Kuppermann BD. Approved biosimilar ranibizumab-a global update. Eye (London, England). 2023 Feb:37(2):200-202. doi: 10.1038/s41433-022-02246-5. Epub 2022 Sep 16
[PubMed PMID: 36114290]
[65]
Dugel PU, Koh A, Ogura Y, Jaffe GJ, Schmidt-Erfurth U, Brown DM, Gomes AV, Warburton J, Weichselberger A, Holz FG, HAWK and HARRIER Study Investigators. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2020 Jan:127(1):72-84. doi: 10.1016/j.ophtha.2019.04.017. Epub 2019 Apr 12
[PubMed PMID: 30986442]
Level 1 (high-level) evidence
[66]
Baumal CR, Spaide RF, Vajzovic L, Freund KB, Walter SD, John V, Rich R, Chaudhry N, Lakhanpal RR, Oellers PR, Leveque TK, Rutledge BK, Chittum M, Bacci T, Enriquez AB, Sund NJ, Subong ENP, Albini TA. Retinal Vasculitis and Intraocular Inflammation after Intravitreal Injection of Brolucizumab. Ophthalmology. 2020 Oct:127(10):1345-1359. doi: 10.1016/j.ophtha.2020.04.017. Epub 2020 Apr 25
[PubMed PMID: 32344075]
[67]
Dugel PU, Singh RP, Koh A, Ogura Y, Weissgerber G, Gedif K, Jaffe GJ, Tadayoni R, Schmidt-Erfurth U, Holz FG. HAWK and HARRIER: Ninety-Six-Week Outcomes from the Phase 3 Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2021 Jan:128(1):89-99. doi: 10.1016/j.ophtha.2020.06.028. Epub 2020 Jun 20
[PubMed PMID: 32574761]
[68]
Nicolò M, Ferro Desideri L, Vagge A, Traverso CE. Faricimab: an investigational agent targeting the Tie-2/angiopoietin pathway and VEGF-A for the treatment of retinal diseases. Expert opinion on investigational drugs. 2021 Mar:30(3):193-200. doi: 10.1080/13543784.2021.1879791. Epub 2021 Feb 4
[PubMed PMID: 33471572]
Level 3 (low-level) evidence
[69]
Heier JS, Khanani AM, Quezada Ruiz C, Basu K, Ferrone PJ, Brittain C, Figueroa MS, Lin H, Holz FG, Patel V, Lai TYY, Silverman D, Regillo C, Swaminathan B, Viola F, Cheung CMG, Wong TY, TENAYA and LUCERNE Investigators. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet (London, England). 2022 Feb 19:399(10326):729-740. doi: 10.1016/S0140-6736(22)00010-1. Epub 2022 Jan 24
[PubMed PMID: 35085502]
Level 1 (high-level) evidence
[70]
Sahni J, Dugel PU, Patel SS, Chittum ME, Berger B, Del Valle Rubido M, Sadikhov S, Szczesny P, Schwab D, Nogoceke E, Weikert R, Fauser S. Safety and Efficacy of Different Doses and Regimens of Faricimab vs Ranibizumab in Neovascular Age-Related Macular Degeneration: The AVENUE Phase 2 Randomized Clinical Trial. JAMA ophthalmology. 2020 Sep 1:138(9):955-963. doi: 10.1001/jamaophthalmol.2020.2685. Epub
[PubMed PMID: 32729888]
Level 1 (high-level) evidence
[71]
Khanani AM, Patel SS, Ferrone PJ, Osborne A, Sahni J, Grzeschik S, Basu K, Ehrlich JS, Haskova Z, Dugel PU. Efficacy of Every Four Monthly and Quarterly Dosing of Faricimab vs Ranibizumab in Neovascular Age-Related Macular Degeneration: The STAIRWAY Phase 2 Randomized Clinical Trial. JAMA ophthalmology. 2020 Sep 1:138(9):964-972. doi: 10.1001/jamaophthalmol.2020.2699. Epub
[PubMed PMID: 32729897]
Level 1 (high-level) evidence
[72]
Lalwani GA, Rosenfeld PJ, Fung AE, Dubovy SR, Michels S, Feuer W, Davis JL, Flynn HW Jr, Esquiabro M. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. American journal of ophthalmology. 2009 Jul:148(1):43-58.e1. doi: 10.1016/j.ajo.2009.01.024. Epub 2009 Apr 18
[PubMed PMID: 19376495]
[73]
Augsburger M, Sarra GM, Imesch P. Treat and extend versus pro re nata regimens of ranibizumab and aflibercept in neovascular age-related macular degeneration: a comparative study. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2019 Sep:257(9):1889-1895. doi: 10.1007/s00417-019-04404-0. Epub 2019 Jun 29
[PubMed PMID: 31256237]
Level 2 (mid-level) evidence
[74]
Kertes PJ, Galic IJ, Greve M, Williams G, Baker J, Lahaie M, Sheidow T. Efficacy of a Treat-and-Extend Regimen With Ranibizumab in Patients With Neovascular Age-Related Macular Disease: A Randomized Clinical Trial. JAMA ophthalmology. 2020 Mar 1:138(3):244-250. doi: 10.1001/jamaophthalmol.2019.5540. Epub
[PubMed PMID: 31917441]
Level 1 (high-level) evidence
[75]
Adrean SD, Chaili S, Grant S, Pirouz A. Recurrence Rate of Choroidal Neovascularization in Neovascular Age-Related Macular Degeneration Managed with a Treat-Extend-Stop Protocol. Ophthalmology. Retina. 2018 Mar:2(3):225-230. doi: 10.1016/j.oret.2017.07.009. Epub 2017 Sep 28
[PubMed PMID: 31047590]
[76]
Cao X, Sanchez JC, Dinabandhu A, Guo C, Patel TP, Yang Z, Hu MW, Chen L, Wang Y, Malik D, Jee K, Daoud YJ, Handa JT, Zhang H, Qian J, Montaner S, Sodhi A. Aqueous proteins help predict the response of patients with neovascular age-related macular degeneration to anti-VEGF therapy. The Journal of clinical investigation. 2022 Jan 18:132(2):. doi: 10.1172/JCI144469. Epub
[PubMed PMID: 34874918]
Level 2 (mid-level) evidence
[77]
Li E, Donati S, Lindsley KB, Krzystolik MG, Virgili G. Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. The Cochrane database of systematic reviews. 2020 May 5:5(5):CD012208. doi: 10.1002/14651858.CD012208.pub2. Epub 2020 May 5
[PubMed PMID: 32374423]
Level 1 (high-level) evidence
[78]
Bakri SJ, Thorne JE, Ho AC, Ehlers JP, Schoenberger SD, Yeh S, Kim SJ. Safety and Efficacy of Anti-Vascular Endothelial Growth Factor Therapies for Neovascular Age-Related Macular Degeneration: A Report by the American Academy of Ophthalmology. Ophthalmology. 2019 Jan:126(1):55-63. doi: 10.1016/j.ophtha.2018.07.028. Epub 2018 Aug 2
[PubMed PMID: 30077616]
[79]
Moja L, Lucenteforte E, Kwag KH, Bertele V, Campomori A, Chakravarthy U, D'Amico R, Dickersin K, Kodjikian L, Lindsley K, Loke Y, Maguire M, Martin DF, Mugelli A, Mühlbauer B, Püntmann I, Reeves B, Rogers C, Schmucker C, Subramanian ML, Virgili G. Systemic safety of bevacizumab versus ranibizumab for neovascular age-related macular degeneration. The Cochrane database of systematic reviews. 2014 Sep 15:9(9):CD011230. doi: 10.1002/14651858.CD011230.pub2. Epub 2014 Sep 15
[PubMed PMID: 25220133]
Level 1 (high-level) evidence
[80]
Sharma A, Kumar N, Kuppermann BD, Bandello F. Abicipar pegol: the non-monoclonal antibody anti-VEGF. Eye (London, England). 2020 May:34(5):797-801. doi: 10.1038/s41433-019-0607-8. Epub 2019 Sep 30
[PubMed PMID: 31570812]
[81]
Kunimoto D, Yoon YH, Wykoff CC, Chang A, Khurana RN, Maturi RK, Agostini H, Souied E, Chow DR, Lotery AJ, Ohji M, Bandello F, Belfort R Jr, Li XY, Jiao J, Le G, Schmidt W, Hashad Y, CEDAR and SEQUOIA Study Groups. Efficacy and Safety of Abicipar in Neovascular Age-Related Macular Degeneration: 52-Week Results of Phase 3 Randomized Controlled Study. Ophthalmology. 2020 Oct:127(10):1331-1344. doi: 10.1016/j.ophtha.2020.03.035. Epub 2020 Apr 9
[PubMed PMID: 32471729]
Level 1 (high-level) evidence
[82]
Khurana RN, Kunimoto D, Yoon YH, Wykoff CC, Chang A, Maturi RK, Agostini H, Souied E, Chow DR, Lotery AJ, Ohji M, Bandello F, Belfort R Jr, Li XY, Jiao J, Le G, Kim K, Schmidt W, Hashad Y, CEDAR and SEQUOIA Study Groups. Two-Year Results of the Phase 3 Randomized Controlled Study of Abicipar in Neovascular Age-Related Macular Degeneration. Ophthalmology. 2021 Jul:128(7):1027-1038. doi: 10.1016/j.ophtha.2020.11.017. Epub 2020 Nov 19
[PubMed PMID: 33221326]
Level 1 (high-level) evidence
[83]
Kunimoto D, Ohji M, Maturi RK, Sekiryu T, Wang Y, Pan G, Li XY, Schneider S, BAMBOO and CYPRESS Study Groups. Evaluation of Abicipar Pegol (an Anti-VEGF DARPin Therapeutic) in Patients With Neovascular Age-Related Macular Degeneration: Studies in Japan and the United States. Ophthalmic surgery, lasers & imaging retina. 2019 Feb 1:50(2):e10-e22. doi: 10.3928/23258160-20190129-13. Epub
[PubMed PMID: 30768224]
[84]
Ferro Desideri L, Traverso CE, Nicolò M. An update on conbercept to treat wet age-related macular degeneration. Drugs of today (Barcelona, Spain : 1998). 2020 May:56(5):311-320. doi: 10.1358/dot.2020.56.5.3137164. Epub
[PubMed PMID: 32406878]
[85]
Chen ER, Kaiser PK. Therapeutic Potential of the Ranibizumab Port Delivery System in the Treatment of AMD: Evidence to Date. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1349-1355. doi: 10.2147/OPTH.S194234. Epub 2020 May 19
[PubMed PMID: 32546942]
[86]
Holekamp NM, Campochiaro PA, Chang MA, Miller D, Pieramici D, Adamis AP, Brittain C, Evans E, Kaufman D, Maass KF, Patel S, Ranade S, Singh N, Barteselli G, Regillo C, all Archway Investigators. Archway Randomized Phase 3 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2022 Mar:129(3):295-307. doi: 10.1016/j.ophtha.2021.09.016. Epub 2021 Sep 29
[PubMed PMID: 34597713]
Level 1 (high-level) evidence
[87]
Arepalli S, Kaiser PK. Pipeline therapies for neovascular age related macular degeneration. International journal of retina and vitreous. 2021 Oct 1:7(1):55. doi: 10.1186/s40942-021-00325-5. Epub 2021 Oct 1
[PubMed PMID: 34598731]
[88]
. The influence of treatment extent on the visual acuity of eyes treated with Krypton laser for juxtafoveal choroidal neovascularization. Macular Photocoagulation Study Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1995 Feb:113(2):190-4
[PubMed PMID: 7532395]
[89]
Schmidt-Erfurth U, Miller JW, Sickenberg M, Laqua H, Barbazetto I, Gragoudas ES, Zografos L, Piguet B, Pournaras CJ, Donati G, Lane AM, Birngruber R, van den Berg H, Strong HA, Manjuris U, Gray T, Fsadni M, Bressler NM. Photodynamic therapy with verteporfin for choroidal neovascularization caused by age-related macular degeneration: results of retreatments in a phase 1 and 2 study. Archives of ophthalmology (Chicago, Ill. : 1960). 1999 Sep:117(9):1177-87
[PubMed PMID: 10496389]
[90]
Giansanti F, Eandi CM, Virgili G. Submacular surgery for choroidal neovascularisation secondary to age-related macular degeneration. The Cochrane database of systematic reviews. 2009 Apr 15:(2):CD006931. doi: 10.1002/14651858.CD006931.pub2. Epub 2009 Apr 15
[PubMed PMID: 19370663]
Level 1 (high-level) evidence
[91]
van Romunde SH, Polito A, Bertazzi L, Guerriero M, Pertile G. Long-Term Results of Full Macular Translocation for Choroidal Neovascularization in Age-Related Macular Degeneration. Ophthalmology. 2015 Jul:122(7):1366-74. doi: 10.1016/j.ophtha.2015.03.012. Epub 2015 Apr 14
[PubMed PMID: 25881514]
[92]
Martel JN, Mahmoud TH. Subretinal pneumatic displacement of subretinal hemorrhage. JAMA ophthalmology. 2013 Dec:131(12):1632-5. doi: 10.1001/jamaophthalmol.2013.5464. Epub
[PubMed PMID: 24337559]
[93]
Shienbaum G, Garcia Filho CA, Flynn HW Jr, Nunes RP, Smiddy WE, Rosenfeld PJ. Management of submacular hemorrhage secondary to neovascular age-related macular degeneration with anti-vascular endothelial growth factor monotherapy. American journal of ophthalmology. 2013 Jun:155(6):1009-13. doi: 10.1016/j.ajo.2013.01.012. Epub 2013 Mar 7
[PubMed PMID: 23465269]
[94]
Kishikova L, Saad AAA, Vaideanu-Collins D, Isac M, Hamada D, El-Haig WM. Comparison between different techniques for treatment of submacular haemorrhage due to Age-Related Macular Degeneration. European journal of ophthalmology. 2021 Sep:31(5):2621-2624. doi: 10.1177/1120672120959551. Epub 2020 Sep 29
[PubMed PMID: 32993349]
[95]
Evans JR, Igwe C, Jackson TL, Chong V. Radiotherapy for neovascular age-related macular degeneration. The Cochrane database of systematic reviews. 2020 Aug 26:8(8):CD004004. doi: 10.1002/14651858.CD004004.pub4. Epub 2020 Aug 26
[PubMed PMID: 32844399]
Level 1 (high-level) evidence
[96]
Liu Y, Fortmann SD, Shen J, Wielechowski E, Tretiakova A, Yoo S, Kozarsky K, Wang J, Wilson JM, Campochiaro PA. AAV8-antiVEGFfab Ocular Gene Transfer for Neovascular Age-Related Macular Degeneration. Molecular therapy : the journal of the American Society of Gene Therapy. 2018 Feb 7:26(2):542-549. doi: 10.1016/j.ymthe.2017.12.002. Epub 2017 Dec 8
[PubMed PMID: 29292162]
[98]
Tripathy K. Choroidal neovascular membrane in intraocular tuberculosis. GMS ophthalmology cases. 2017:7():Doc24. doi: 10.3205/oc000075. Epub 2017 Sep 1
[PubMed PMID: 28944155]
Level 3 (low-level) evidence
[99]
Tripathy K, Chawla R, Sharma YR. Intravitreal Bevacizumab for Choroidal Neovascular Membrane at the Edge of a Healed Choroidal Tuberculoma. Ocular immunology and inflammation. 2018:26(2):239-241. doi: 10.1080/09273948.2016.1206205. Epub 2016 Aug 19
[PubMed PMID: 27541084]
[100]
Wadekar B, Tripathy K, Chawla R, Venkatesh P, Sharma YR, Vohra R. An 18-year-old female with unilateral painless vision loss. Oman journal of ophthalmology. 2016 Sep-Dec:9(3):193
[PubMed PMID: 27843243]
[101]
Chi SC, Kang YN, Huang YM. Systematic review with network meta-analysis of antivascular endothelial growth factor use in managing polypoidal choroidal vasculopathy. Scientific reports. 2021 Feb 2:11(1):2735. doi: 10.1038/s41598-021-82316-y. Epub 2021 Feb 2
[PubMed PMID: 33531615]
Level 1 (high-level) evidence
[102]
Arda H, Haritoglou C. [PEHCR-Peripheral exudative hemorrhagic chorioretinopathy: Diagnosis and treatment]. Die Ophthalmologie. 2022 Aug:119(8):868-871. doi: 10.1007/s00347-022-01658-8. Epub 2022 May 31
[PubMed PMID: 35925329]
[103]
Vandefonteyne S, Caujolle JP, Rosier L, Conrath J, Quentel G, Tadayoni R, Maschi C, Le Mer Y, Dot C, Aknin I, Thariat J, Baillif S. Diagnosis and treatment of peripheral exudative haemorrhagic chorioretinopathy. The British journal of ophthalmology. 2020 Jun:104(6):874-878. doi: 10.1136/bjophthalmol-2018-313307. Epub 2019 Oct 23
[PubMed PMID: 31645320]
[104]
Shields CL, Salazar PF, Mashayekhi A, Shields JA. Peripheral exudative hemorrhagic chorioretinopathy simulating choroidal melanoma in 173 eyes. Ophthalmology. 2009 Mar:116(3):529-35. doi: 10.1016/j.ophtha.2008.10.015. Epub 2009 Jan 20
[PubMed PMID: 19157563]
[105]
Yannuzzi LA, Negrão S, Iida T, Carvalho C, Rodriguez-Coleman H, Slakter J, Freund KB, Sorenson J, Orlock D, Borodoker N. Retinal angiomatous proliferation in age–related macular degeneration. 2001. Retina (Philadelphia, Pa.). 2012 Feb:32 Suppl 1():416-34
[PubMed PMID: 22451953]
[106]
Bressler NM, Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: two-year results of 2 randomized clinical trials-tap report 2. Archives of ophthalmology (Chicago, Ill. : 1960). 2001 Feb:119(2):198-207
[PubMed PMID: 11176980]
Level 1 (high-level) evidence
[107]
. Laser photocoagulation of subfoveal neovascular lesions in age-related macular degeneration. Results of a randomized clinical trial. Macular Photocoagulation Study Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1991 Sep:109(9):1220-31
[PubMed PMID: 1718250]
Level 1 (high-level) evidence
[108]
. Laser photocoagulation of subfoveal neovascular lesions of age-related macular degeneration. Updated findings from two clinical trials. Macular Photocoagulation Study Group. Archives of ophthalmology (Chicago, Ill. : 1960). 1993 Sep:111(9):1200-9
[PubMed PMID: 7689827]
[109]
Bressler NM, Frost LA, Bressler SB, Murphy RP, Fine SL. Natural course of poorly defined choroidal neovascularization associated with macular degeneration. Archives of ophthalmology (Chicago, Ill. : 1960). 1988 Nov:106(11):1537-42
[PubMed PMID: 2461191]
[110]
Bressler SB, Pieramici DJ, Koester JM, Bressler NM. Natural history of minimally classic subfoveal choroidal neovascular lesions in the treatment of age-related macular degeneration with photodynamic therapy (TAP) investigation: outcomes potentially relevant to management--TAP report No. 6. Archives of ophthalmology (Chicago, Ill. : 1960). 2004 Mar:122(3):325-9
[PubMed PMID: 15006843]
[111]
Hanscom TA, Diddie KR. Early surgical drainage of macular subretinal hemorrhage. Archives of ophthalmology (Chicago, Ill. : 1960). 1987 Dec:105(12):1722-3
[PubMed PMID: 3689195]
[112]
Schoeppner G, Chuang EL, Bird AC. The risk of fellow eye visual loss with unilateral retinal pigment epithelial tears. American journal of ophthalmology. 1989 Dec 15:108(6):683-5
[PubMed PMID: 2596548]
[113]
Mangione CM, Gutierrez PR, Lowe G, Orav EJ, Seddon JM. Influence of age-related maculopathy on visual functioning and health-related quality of life. American journal of ophthalmology. 1999 Jul:128(1):45-53
[PubMed PMID: 10482093]
Level 2 (mid-level) evidence
[114]
Williams RA, Brody BL, Thomas RG, Kaplan RM, Brown SI. The psychosocial impact of macular degeneration. Archives of ophthalmology (Chicago, Ill. : 1960). 1998 Apr:116(4):514-20
[PubMed PMID: 9565052]
[115]
Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Archives of ophthalmology (Chicago, Ill. : 1960). 2001 Oct:119(10):1417-36
[PubMed PMID: 11594942]
Level 1 (high-level) evidence
[116]
Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013 May 15:309(19):2005-15. doi: 10.1001/jama.2013.4997. Epub
[PubMed PMID: 23644932]
Level 1 (high-level) evidence
[117]
Margrain TH. Helping blind and partially sighted people to read: the effectiveness of low vision aids. The British journal of ophthalmology. 2000 Aug:84(8):919-21
[PubMed PMID: 10906105]
[118]
Shuttleworth GN, Dunlop A, Collins JK, James CR. How effective is an integrated approach to low vision rehabilitation? Two year follow up results from south Devon. The British journal of ophthalmology. 1995 Aug:79(8):719-23
[PubMed PMID: 7547780]