Continuing Education Activity
There is a continued increase in the prevalence of congenital heart diseases. The anesthesiologist involved in the perioperative management of patients with congenital heart disease faces a myriad of challenges. This activity outlines certain basic principles subject to each patient. Although, during these present times, sicker and younger patients present for complex and innovative surgical procedures, however, the morbidity and mortality associated with it have impressively declined. This activity reviews the perioperative management of patients with congenital heart diseases and highlights the role of the interprofessional team in evaluating and treating this condition.
Objectives:
- Summarize the classification of congenital heart defects and the physiology of fetal circulation.
- Explain the importance of careful history and assessment during the perioperative management of patients with congenital heart diseases.
- Outline the anesthetic management of patients with congenital heart diseases for surgery.
- Review the role of team effort and good communication between the healthcare practitioners involved in the perioperative management of patients with congenital heart diseases.
Introduction
Congenital heart disease comprises structural and functional disease of the heart. The incidence of congenital heart disease (CHD) is relatively uncommon. Nearly 1% of births are affected each year in the United States. The leading cause of death between 1999 and 2006 was CHD in 27,960 people; 48% of fatalities were infants due to complex surgeries and prolonged intensive care unit (ICU) stay.[1]
There is fetal wastage due to congenital heart defects incompatible with life and some heart lesions that remain asymptomatic (e.g., bicuspid aortic valve and patent ductus arteriosus) in early life, thus making the true incidence unknown. The different population shows a different pattern of CHD. For instance, there is an increased prevalence of congenital disabilities in premature and small for gestational age infants compared to full-term newborns.[2]
It is a unique challenge for an anesthesiologist caring for children with congenital heart defects undergoing surgery. There has been significant improvement in diagnostics, cardiopulmonary bypass techniques, perioperative monitoring, cardiac catheterization techniques, and minimally invasive procedures for sicker children.[3]
Tailoring the anesthetic plans is crucial for each child with unique requirements, special considerations, and pathophysiological concerns. In this regard, the anesthetist must be innovative and flexible, as rigid protocols are never appropriate in stressful situations. For the success of a pediatric surgical program, good team effort and communication among the team members are essential. Early repair of congenital cardiac defects with advancement prevents progression to congestive heart failure and unrepairable complications. Some children may benefit from cardiac transplantation with unsuccessful surgical repair.[4] A thorough individualized plan with meticulous attention is imperative for all the options to be successful.
Function
Congenital heart defects of the cardiac architecture interfere with the separation of the cardiac segments, venous drainage, and function of the valve apparatus.[5] The American Heart Association classifies congenital cardiac defects into three categories, namely, septal, obstructive, and cyanotic defects.
The septum separates the right and left sides of the heart. After birth, if there is communication between the two sides, one of the following defects may occur, e.g., patent foramen ovale, atrial septal defect, ventricular septal defect, or complete atrioventricular defect. The obstructive cardiac anomalies include aortic stenosis, pulmonary stenosis, and coarctation of the aorta.
The cyanotic defects have a characteristic feature of cyanosis because of the inadequate oxygenation of the blood. It includes tetralogy of Fallot, transposition of the great vessels, tricuspid atresia, pulmonary atresia, truncus arteriosus, total anomalous pulmonary venous connection, and hypoplastic left heart syndrome.[6] The table summarizes cyanotic and non-cyanotic congenital heart defects.
| Cyanotic Heart Diseases |
Non-cyanotic Heart Diseases |
| Tetralogy of Fallot |
Atrial septal defect |
| Tricuspid atresia |
Ventricular septal defect |
| Other univentricular hearts with pulmonary stenosis |
Atrio-ventricular septal defect |
| Transposition of great arteries |
Patent ductus artriosus |
| Total anomalous pulmonary venous return |
Aortic stenosis |
| Ebstein's anomaly |
Pulmonary Valve stenosis |
| Hypoplastic left heart syndrome |
Coarctation of the aorta |
Issues of Concern
Physiology of Fetal Circulation
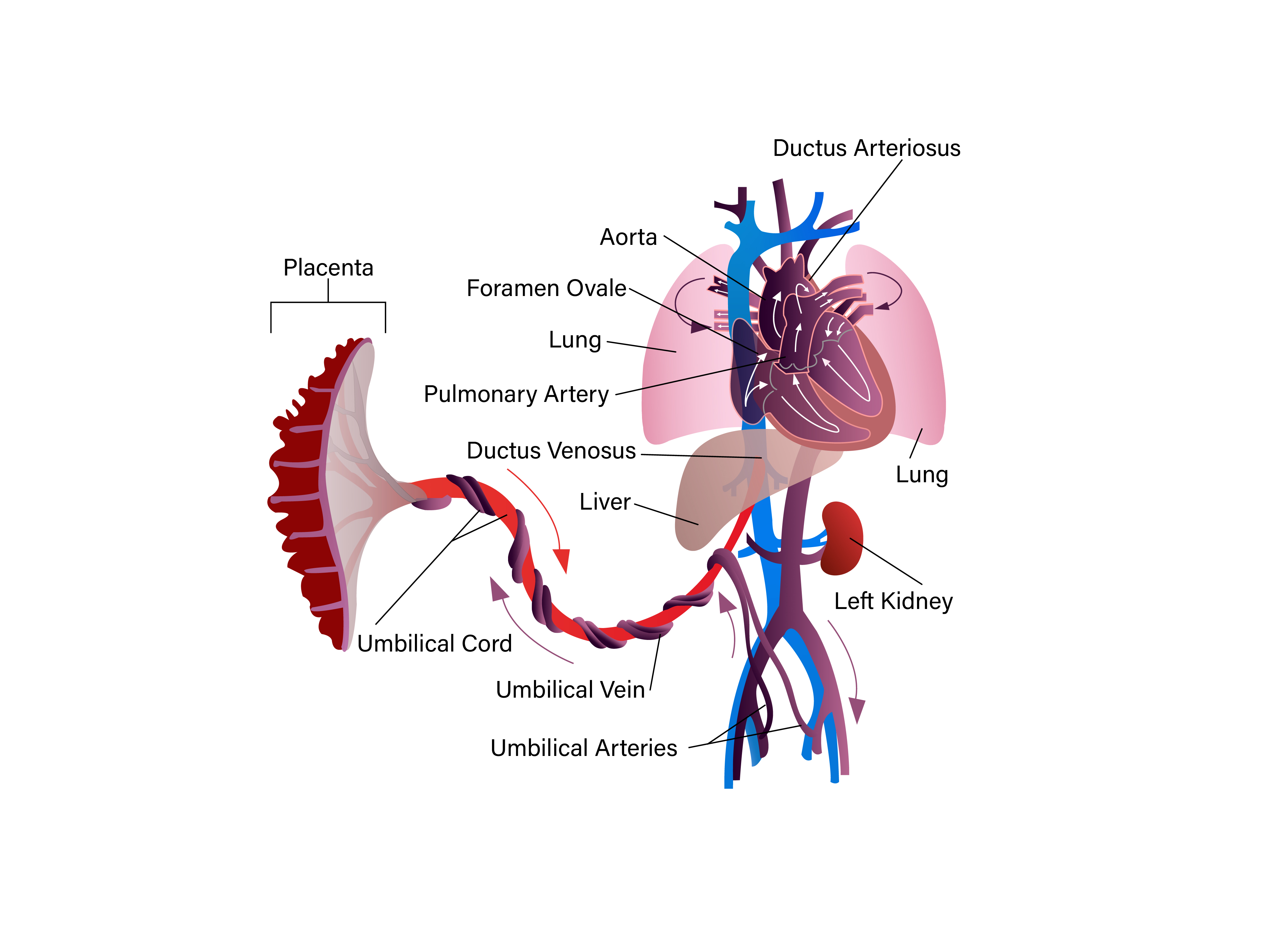
A comprehensive understanding of fetal and adult circulation is mandatory to grasp clinical and anesthetic considerations of congenital heart diseases (CHD). Fetal circulation has channels that shunt blood away from the lungs and the ventricles, which contribute to the systemic system by pumping blood into circulation. This parallel circuit permits fetal growth and development even in cardiac malformations. Three in-utero channels of the circulation shunt blood: ductus arteriosus, foramen ovale, and ductus venosus.
Well-oxygenated blood with a partial pressure of 33 mmHg enters the liver via the umbilical vein from the placenta. From there, ductus venosus shunts almost half of the blood into the inferior vena cava. Foramen ovale shunts one-third of the blood entering the right atrium into the left atrium. On the other hand, poorly oxygenated blood in the superior vena cava enters the right ventricle with only 2 or 3% blood crossing the foramen ovale. The right ventricle shunts blood into the descending aorta through the ductus arteriosus.
The fetal circulation structure allows the well-oxygenated blood from the inferior vena cava to perfuse the brain, coronary circulation, and upper extremities. The perfusion of the lower part occurs with less oxygenated blood from the ductus arteriosus. Hence, in fetal circulation, pulmonary and systemic circulation works in parallel. On the other hand, in adult circulation, the two circulations work in series that constitute the entire cardiac output.[7]
At the time of birth, fetal circulation undergoes a remarkable transition that helps the infant adapt to the stresses of extrauterine life.[8] This transitional stage is temporary and unstable. Depending on the stresses, it may exist for a few hours to many weeks. Factors that may contribute to the instability of transitional circulation include the state of the ductus arteriosus, foramen ovale, ductus venosus, pulmonary vasculature as well as the immaturity of the neonatal heart. Certain conditions like prematurity, hypoxia, hypothermia, hypercarbia, acidosis, sepsis, and congenital heart defects may prolong transitional circulation.[7]
The ductus arteriosus functionally closes within a few hours of birth; however, anatomic closure occurs after several weeks. Those infants born with cyanotic heart disease, until the repair of palliative procedure, the ductus arteriosus is patent. The foramen ovale closes when the left atrial pressure exceeds the right atrial pressure within the few that occur after birth. The anatomic closure occurs after many months, and 30% of the adults may demonstrate probe patency of the foramen ovale.[9]
The umbilical arteries and veins close right after birth and ductus venosus. There is a significant change in pulmonary vascular resistance, which is high in utero but decreases after birth. In the first 24 hours, it is lower than the systemic circulation, then gradually decreases over the next five to six weeks and more over the next two to three years. During the transition period, the pulmonary vasculature is very sensitive to hypoxemia, acidosis, or bronchospasm. It may result in elevated pulmonary artery pressure causing shunting of blood across the foramen ovale or ductus arteriosus.
Preoperative Evaluation
The age group presenting for surgical repair of congenital heart disease includes infants and children and is a diverse clinical population that varies considerably in anatomy, physiology, and size. A summary of preoperative evaluation is mentioned in the table below.
| Clinical History |
Palpitations or syncopeSigns and symptoms of congestive cardiac failureOther congenital abnormalities (e.g., airway, genito-urinary, skeletal, etc.)Recent hospital admissions and current medicationsPast surgical and interventional historyMost recent follow-up
|
| Physical Examination |
Cardiac murmur, thrill, bruit, arrhythmiasTachypnea, rales, increased work of breathingPoor peripheral pulses, delayed capillary refill, bounding, or diminished pulses.Cold extremities, sweating, skin mottlingHepatomegaly, splenomegalyDependent edema
|
| Laboratory Data |
Complete blood count; erythrocytosis, anemiaSerum electrolytes; hypokalemia, hyponatremiaCoagulation profile |
| Imaging and Additional Tests |
Chest X-ray; cardiomegaly, pulmonary edema, infiltratesECG; rhythm, signs of atrial or ventricular hypertrophyEchocardiography; anatomy and function |
|
Specific Studies
|
Cardiac catheterization; anatomy, pressure gradients, shunts, saturations, resistancesCardiac MRI; anatomy, right ventricle and left ventricle function, pulmonary blood flow |
| Preoperative Preparation |
The general rule of 2,4,6,8 for NPO intervals in neonates, infants, and children with congenital heart disease, e.g., 2 hours for clear liquids, 4 hours for breast milk, 6 hours for formula milk, and 8 hours for solid foodIntravenous maintenance fluidPremedication |
Clinical History
The pediatric population most commonly presents for the correction of congenital heart defects. The current definition of pediatric patients by their age; is neonates ( birth to 28 days), infants (one month to one year), toddlers (one year to four years), and children (four to thirteen years).[7]
All these patients undergo complete and detailed preoperative assessment. It should include current medications, allergies, past hospitalizations due to pulmonary infections, and any surgery, including previous anesthetic experience. The cardiac function and reserve evaluation is done by inquiring about age-appropriate activities. A crucial clinical indicator is a parent's observation of the worsening symptoms of cardiac failure, inability to keep pace with other siblings, sweating, tiring quickly, and failure to thrive.
Physical Examination
A physical examination is critical in assessing all the symptoms and ruling out the possibility of any issue that can delay the procedure. It includes age-specific vital signs, growth charts, and age-appropriate weight, head circumference, and height. Essential points in the physical examination include cyanosis, clubbing, symptoms of congestive cardiac failure, monitoring sites, and limitations to vascular access.
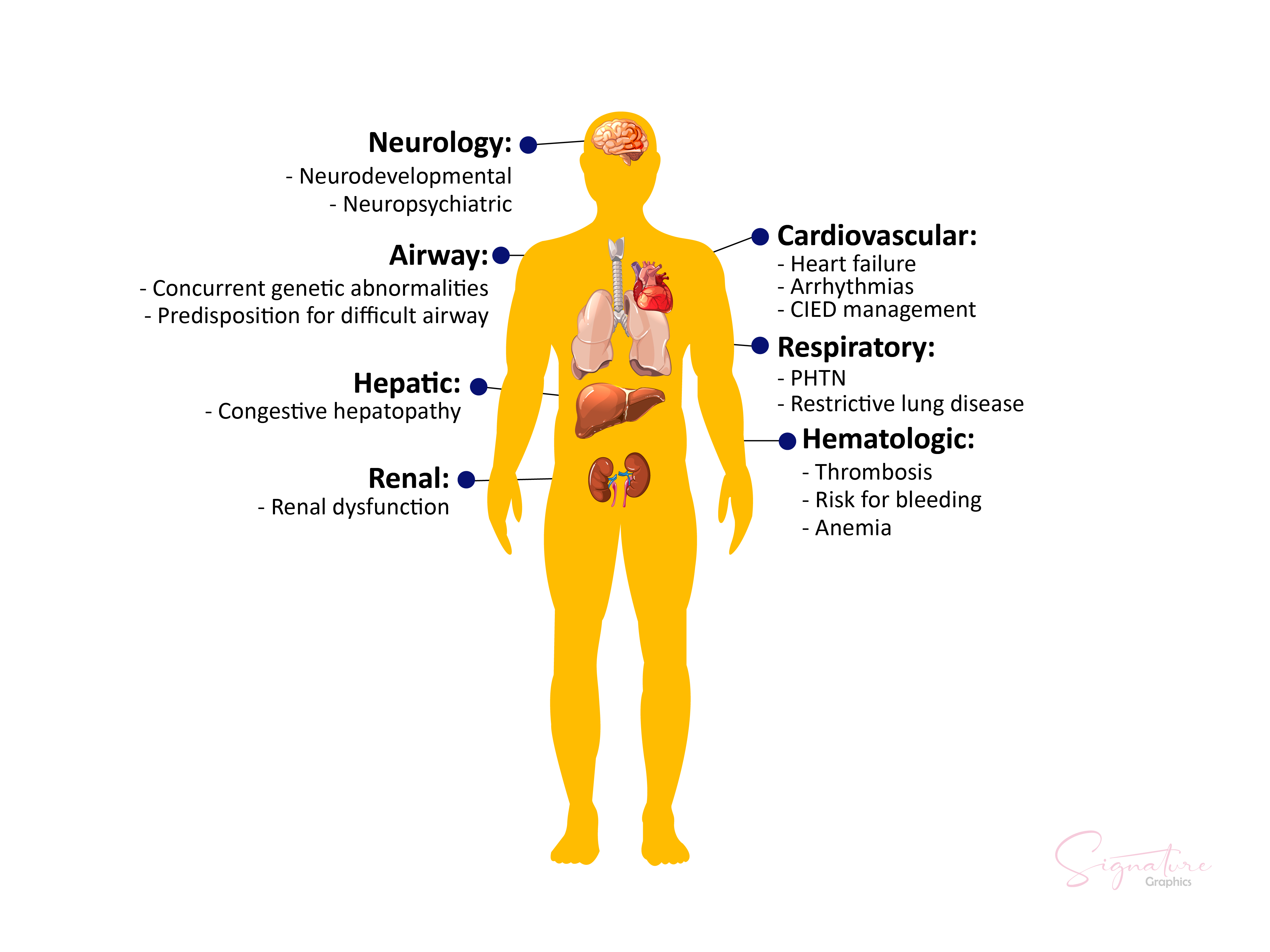
Almost 8% of children with congenital cardiac defects often have other congenital abnormalities. One must consider the likelihood of airway abnormalities in patients with congenital heart disease, especially premature and with a weight of fewer than 10 kilograms.[10] For example, patients with Trisomy 21 have a 50% incidence of congenital heart defects, so physical examination is crucial in defining these defects.[11]
Laboratory Data
A correlation between laboratory data and clinical findings is pertinent. A child presenting with congestive cardiac failure may have iron deficiency anemia. A cyanotic patient may have erythrocytosis due to the blood's degree of desaturated hemoglobin. A high hematocrit level requires an exchange transfusion before surgery to prevent neurological sequelae associated with excessive blood viscosity. One may find prolongation of prothrombin time (PT) and partial thromboplastin time (PTT) in cyanosis. An anesthesiologist should be vigilant and in direct communication with the surgeon for the arrangement of blood and its blood products in case of extensive dissection with re-operation.
A preoperative detailed renal function evaluation is critical as acute kidney injury may occur in these patients during the perioperative period. Renal ultrasound rules out anatomical lesions and baseline serum creatinine and glomerular filtration rate for monitoring and preparation beforehand if the need for postoperative dialysis arises.[12]
A chest radiograph as a screening tool provides anatomical and functional information. An organized approach to a chest radiograph includes seven steps; technique, situs, heart and chamber size, pericardium, excellent vessel anatomy, and pulmonary vascularity. It shows accuracy and reproducibility in identifying abnormal pulmonary vascularity in congenital heart disease. However, 24 to 68 % low sensitivity has decreased the ability to detect pulmonary vascularity.[13]
A 12-lead electrocardiogram (ECG) is the gold standard for arrhythmia evaluation and the presence of sinus rhythm.
Cardiac catheterization and echocardiography data are crucial in understanding the pathophysiology and devising a surgical and anesthetic plan.[14][15] The information derived from cardiac catheterization includes;
- Anatomical defects
- Saturation data to calculate the ratio of pulmonary to systemic blood flow (Qp: Qs), shunting, and V/Q mismatch
- Pressure data to compare right and left cardiac and systemic and pulmonary arterial pressures. Measure pressure gradients across valves and shunts.
- Angiographic data assess ventricular wall motion and blood flow patterns through great vessels and cardiac chambers.
- Study the current functional status of the heart and prior surgical interventions.
- Monitor the effect of interventions on the patients and assessment of reversible pulmonary artery hypertension.[16]
Echocardiography is a critical non-invasive tool essential in diagnosing pediatric congenital heart defects. It helps define both the morphological and functional characteristics of a congenital heart defect. Compared with adults, echocardiography in pediatric patients provides information on the heart position in the thorax, the atrial situs viscerum, the vein-atrial, and the atrioventricular connections between the ventricles and ventriculoatrial connection, and the relationship of the great arteries.[17]
Nowadays, assessments of congenital heart defects utilize MRI. It quantifies ventricle volumes, valve regurgitation, and blood flow through the heart and great vessels. It also highlights better delineation of extracardiac vascular anatomy and an assessment of previous scar tissue.[18][19]
Preoperative Preparation
The routine preoperative preparation for surgery is rarely different for pediatrics and adults. It is crucial to have complete anesthesia equipment with various-sized airway equipment. Appropriate emergency medications in doses consistent with the patient's weight should be available. The anesthetist technician/ nurse prepares selected infusions in advance for critically ill patients. Using appropriate intravenous (IV) catheters and air-trap filters are recommended.
Routine preoperative intravenous fluids and nil-per-os (NPO) orders are according to age-specific requirements. The general rule of 2,4,6,8 is for NPO intervals in neonates, infants, and children with congenital heart disease, e.g., 2 hours for clear liquids, 4 hours for breast milk, 6 hours for formula milk, and 8 hours for solid food.[20]
The anesthetist should avoid dehydration in these patients as this harms the hemodynamics or viscosity of blood in erythrocytosis patients. The neonates and infants also require glucose to prevent detrimental effects on the neurological outcome during the deep hypothermic circulatory arrest. It is given along with maintenance fluid in the perioperative period with 10% dextrose at 2ml/kg/hr.[21] Maintenance of blood sugar levels is crucial as these patients on total parenteral and intra-lipid therapy are prone to hyperglycemia.
As patients with congenital heart defects are psychosocially affected due to multiple surgeries and critical illness, premedication before induction alleviates anxiety in older children and adults. It helps in child separation from the parents and placement of an IV catheter. A benzodiazepine such as midazolam at a dose of 1mg/kg may be helpful in older children and adults with no history of cardiac surgery.[22]
In patients with previous surgeries, midazolam alone may not be sufficient. Usually, an anesthetist utilizes another adjunct, such as oral or intranasal ketamine or intranasal dexmedetomidine.[23][24]
One must individualize the premedication dose to the patient's need to avoid untoward side effects such as respiratory depression and hemodynamic instability. An anesthesiologist's presence is necessary for administering and assessing these patients. These patients are usually on routine use of diuretics, digoxin, and angiotensin-converting enzyme (ACE)-inhibitors. These medications should be withheld on the day of surgery to avoid exaggerated responses intraoperatively due to anesthetic agents. Those patients on prostaglandin and ionotropic infusions continue intraoperatively.
Intraoperative Monitoring
Multiple monitors can hinder a smooth induction as a child or infant awakens or minimally sedates, divided into pre and post-induction monitoring. Pre-induction monitoring includes a non-invasive automated blood pressure cuff, electrocardiogram, pulse oximeter, and end-tidal carbon dioxide monitor. After induction of anesthesia, the anesthetist places invasive arterial catheters in either radial or femoral arteries. In newborns, an umbilical artery may be cannulated, but it is later replaced with a peripheral arterial catheter.
In these patients, invasive blood pressure monitoring along with upper and lower extremity blood pressure monitoring is vital for detecting residual coarctation of the aorta or aortic arch/isthmus obstruction. Special considerations are given to previous cardiac procedures such as Blalock-Taussig shunt, subclavian artery patch repair or aortic coarctation, or sacrifice of an aberrant subclavian artery that compromise the ipsilateral intra-arterial pressure monitoring.
Percutaneous central venous access is a requirement in almost all cardiac surgeries.[25] It offers many advantages, including measurement of central venous pressure, infusions of vasoactive agents, ionotropic, and blood products, measurement of mixed venous oxygenation saturation to determine cardiac output(CO), and Qp: Qs assessment of superior vena cava drainage during cardiopulmonary bypass. Some patients may require a pulmonary artery catheter for postoperative pulmonary artery pressure monitoring, but its preoperative use is relatively uncommon.
Temperature monitoring intraoperatively occurs with either rectal, oesophageal, or nasopharyngeal temperature probe for all cardiopulmonary bypass cases.[26] Other monitoring types include near-infrared spectroscopy, transcranial doppler, and transesophageal echocardiography (TEE). The near-infrared spectroscopy (NIRS) enables the monitoring of continuous regional tissue oxygenation. It monitors cerebral oxygenation as well as somatic oxygenation.[27]
The recent use of transcranial doppler in neonates and infants has evolved, allowing the measurement of cerebral blood flow velocity and detecting microemboli in the cerebral circulation.[28] It is being utilized to refine the post-cardiopulmonary bypass de-airing routines and decrease iatrogenic embolic events. Intraoperative transesophageal echocardiography has dramatically impacted the repair of the semilunar valve or atrioventricular valve, complex left ventricular outflow reconstructions, and detailed anatomy delineation. TEE has a significant role in the detection of residual ventricle septal defects.[29]
Airway Management
Good airway management is fundamental to the anesthetic care of patients with congenital heart disease. As pulmonary vascular resistance is greatly affected by ventilatory pattern, PaO2, PaCO2, and pH, prompt control of the airway and ventilation will allow optimal pulmonary blood flow in these patients. Children with interstitial pulmonary edema have poor lung compliance and high peaked airway pressures.[30]
During mask ventilation, care must be taken to as not to insufflate the stomach. As neonates and infants have a large tongue, the placement of an oral airway will pull the tongue away from the pharyngeal wall facilitating mask ventilation. Nasal endotracheal tubes are generally utilized for children under 2 or 3 years of age, as they provide better stability and TEE intraoperatively. However, it must be passed cautiously in patients with a bidirectional Glenn shunt or Fontan because of higher venous pressures. All patients before induction should be de-nitrogenated, even those affected by higher O2 concentrations that may compromise peripheral vascular resistance.
Anesthesia Induction and Maintenance
No one anesthetic induction technique is superior to others in patients with CHD. The patient's age, cardiopulmonary state, cyanosis, and emotional state all play a vital role in choosing an anesthetic technique. In patients with ventricular systolic function severely impaired, intravenous induction is the choice of anesthetic technique. A combination of sevoflurane with midazolam/fentanyl has no significant effect on the myocardium in patients with a single ventricle. Likewise, volatile anesthetics sevoflurane, halothane, isoflurane, and fentanyl/midazolam do not affect Qp: Qs in patients with atrial septal defect and ventricle septal defects when given with 100% oxygen.[31]
Mask induction is safe with volatile anesthetics in patients with less severe cardiorespiratory compromise. However, the duration of induction is significantly prolonged in cyanotic patients with reduced pulmonary blood flow. In this regard, the airway is partially controlled and may result in obstruction or hypoventilation, leading to hypoxemia. The inhalational agent of choice is sevoflurane. Due to the pungent odor of isoflurane and desflurane, anesthesia induction with these agents is relatively unsuitable.
Intravenous induction is the most suitable technique accomplished with a combination of synthetic opioids and a muscle relaxant. In patients with low aortic diastolic volume, muscle relaxants, including rocuronium, vecuronium, or cis-atracurium, can be used without affecting the heart rate. In children with depressed systolic function, a combination of opioids with etomidate is often used. Ketamine is a beneficial intravenous induction agent as it causes a minimal increase in pulmonary artery pressure by preserving peripheral vascular resistance.[32]
As thiopental and propofol depress the myocardial activity, their use in the induction of anesthesia makes them less favorable agents. These are only used in shunt lesions with preserved cardiovascular function.[33]
For those patients with difficult peripheral vascular access, induction of anesthesia can be carried out through intramuscular induction with ketamine, succinylcholine, and glycopyrrolate. This technique provides rapid induction with reasonable airway control for tracheal intubation. Though it only provides a brief period for a patient's mobility.
The maintenance of anesthesia is generally done with synthetic opioid infusions such as fentanyl or sufentanil alone or in combination with sevoflurane or isoflurane. The maintenance of anesthesia during cardiopulmonary bypass holds unique considerations. Maintenance of the depth of anesthesia is crucial to avoid untoward actions during cooling and rewarding.
Cardiopulmonary Bypass Circuit
Surgical procedures are often challenging for congenital heart defects. Safe cardiopulmonary bypass is crucial to a successful outcome in patients with a narrow margin of safety. Implementation of safety protocols and checklists is vital to the successful conduct of open heart procedures. A firm hold of the principles of CPB is essential for better surgical outcomes.[34] The cardiopulmonary bypass circuit (CPB) isolates the cardiopulmonary system to obtain better surgical exposure for operating on the heart and great vessels. The CPB must have the following features;
- Perform the functions of the cardiopulmonary system
- Have the ability to add oxygen and remove carbon dioxide
- Provision of adequate perfusion to all organs
- Fulfillment of the requirements mentioned above without causing damage
Infection Prophylaxis
As CBP weakens the immune system to act against bacterial infections, postoperative antibiotic prophylaxis is necessary for children after cardiac surgery.[35] There is controversy about the use and duration of antibiotics used for prophylaxis. Frequently used antibiotics are first or second-generation cephalosporins, e.g., cefazolin 30mg/kg given eight hours per day. For an uncomplicated course, antibiotics are given for 2 to 3 days in specific centers. No evidence-based data is available for this; however, antibiotic prophylaxis usually continues 24 hours post chest closure or ECMO/ PD removal.[36]
Postoperative Intensive Care Management
A multidisciplinary team involves coordinating multiple healthcare professionals (cardiac surgeon, cardiologist, intensivist, anesthetist, pediatrician, respiratory therapist, and cardiac critical care-trained nurse). The successful outcome in the postoperative critical care management of any cardiac surgical patient who has undergone a palliative or corrective procedure for congenital heart disease is due to effective postoperative care of such patients, and it includes;
- Continuous monitoring of cardiac hemodynamic functions, pulmonary, and other vital organs such as the kidney, liver, and central nervous system is necessary.
- The prompt appropriate action to restore normal function whenever deviations from normal are identified.
Postoperative Problems and their Causes
The most common postoperative problems and their causes are summarised in the table below.
| Problems |
Causes |
| High Blood Pressure |
Fear, anxiety, pain, hypervolemia, abrupt discontinuation of certain drugs (beta-blockers, ACE inhibitors), coarctation of aorta repair, rarely cerebral seizures, and hypoglycemia. |
| Low Blood Pressure |
hypovolemia, low cardiac output due to myocardial insufficiency, pericardial effusion, arrhythmias, excessive blood loss, vasodilators, diuresis, pneumothorax, sepsis, and shock. |
| High Central venous pressure |
Tense or light patient (inadequate sedation in ventilation patients); reduced right ventricle function, tamponade, pneumothorax; a high CVP indicates poor systemic ventricular in univentricular heart or atrioventricular valve regurgitation.
|
| Low Central venous Pressure |
Hypovolemia may be due to fluid deficit, excessive drain output, hemorrhage, increased diuresis, and decreased volume intake. |
| High Arterial Saturation |
In univentricular hearts, an arterial saturation over 85% suggests an imbalance between pulmonary and systemic perfusion. |
| Low Arterial Saturation |
Basal lung atelectasis, hypoventilation, technical problems with the ventilation device, disconnected/obstructed tube, pneumothorax, pleural effusion, pneumonia, pulmonary edema, pulmonary hemorrhage, secretion, right to left shunt. |
| Tachycardia |
Tachyarrhythmias with Narrow QRS complexes: sinus tachycardia, supraventricular tachycardia, or Wide QRS complexes: ventricular tachycardia |
| Bradycardia |
Bradyarrhythmias, Sinus Bradycardia, atrioventricular block. |
| High Lactate |
Decreased systemic perfusion, cerebral seizures, and mesenteric ischemia |
Clinical Significance
Specific Cardiac Lesions and Management
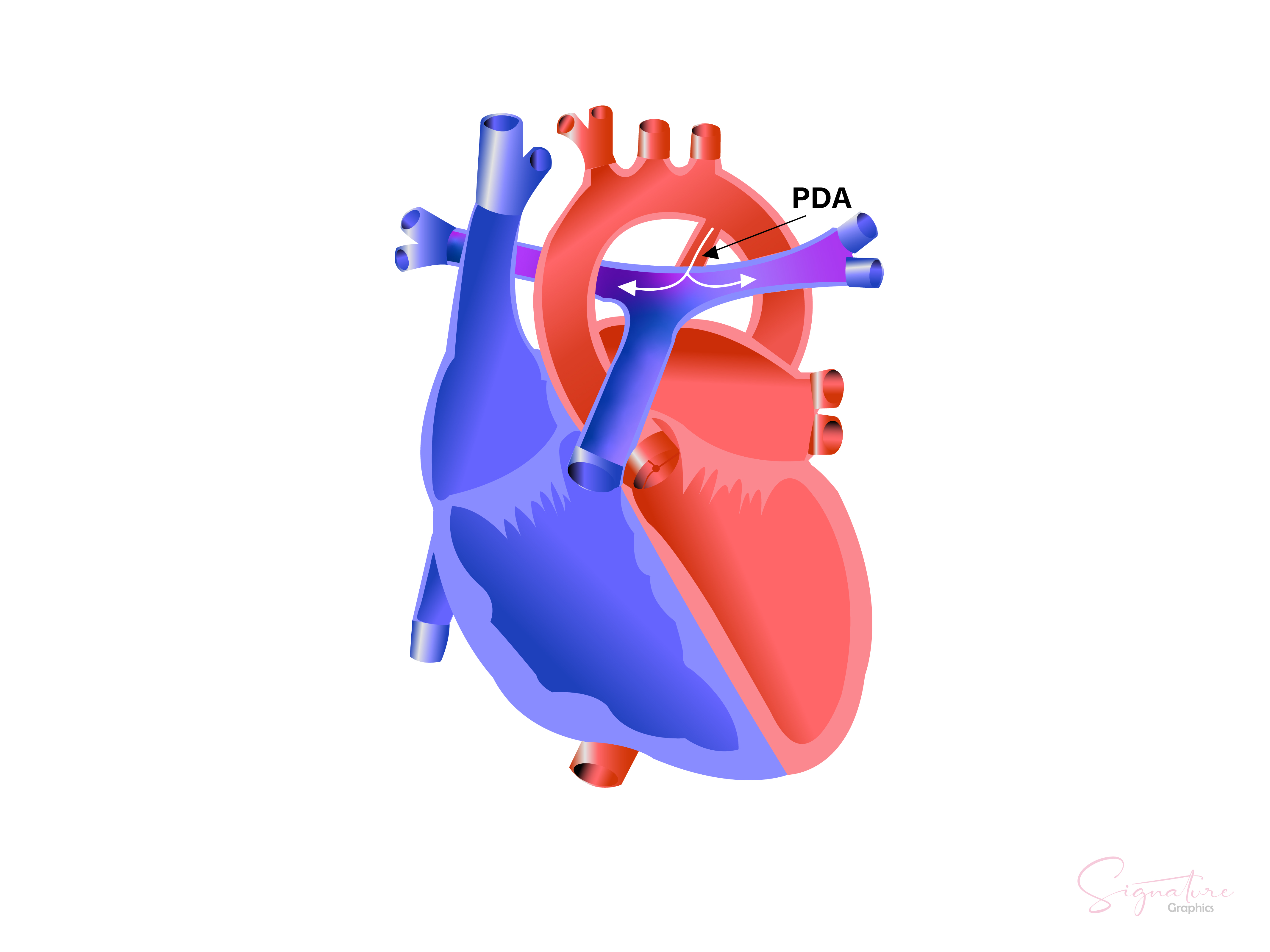
Patent Ductus Arteriosus (PDA)
It connects the pulmonary trunk with the descending aorta distal to the left subclavian artery. It is a simple shunt with very little or no pressure gradient across the duct. The shunting of blood depends upon the ratio of pulmonary vascular resistance to systemic vascular resistance. Initially, PDA is managed conservatively by modest fluid restriction and the use of positive end-expiratory pressure. Pharmacological treatment with indomethacin is recommended if conservative measures fail during the first week of life.[37]
Surgically PDA is closed either by left thoracotomy or video-assisted thoracoscopic surgery (VATS). PDA closure devices are being employed and approved by Food and Drug Administration. A patient's immobility dramatically facilitates this procedure, usually done under general anesthesia in uncooperative children. If the repair is delayed, the patients may present with pulmonary hypertension and ventricular dysfunction.[38]
The anesthetic management goals for a patient with patent ductus arteriosus are summarised in the table below.
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) maintain heart rate, contractility, and preload |
| 2) Avoid a decrease in pulmonary vascular resistance |
| 3) Avoid increase in pulmonary vascular resistance |
| 4) Bubble precautions |
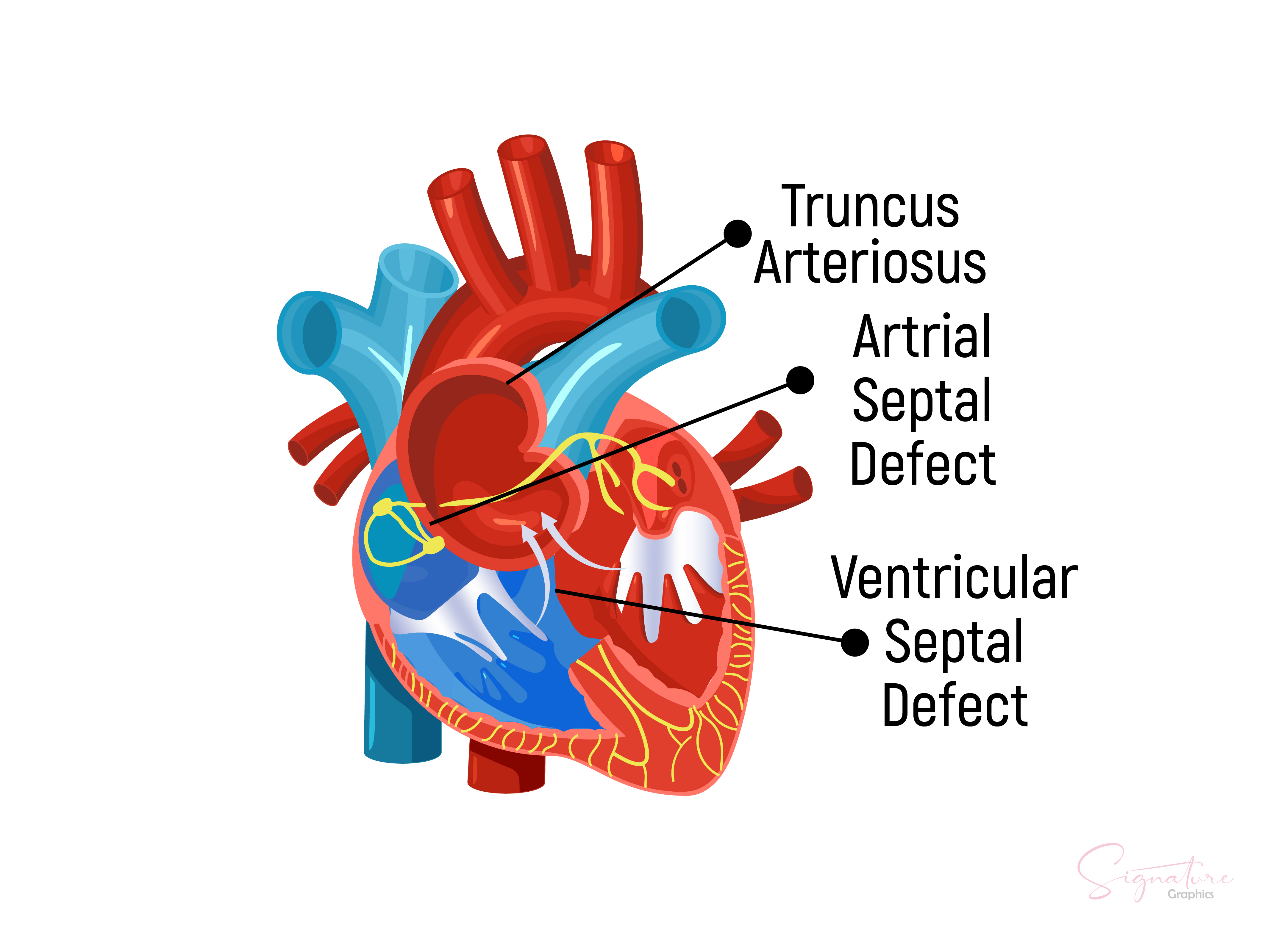
Atrial Septal Defect
A complete atrioventricular septal defect is the absence of ventricular and atrial septum segments. It is present in the region of the absent atrioventricular(AV) valves, and the development of the AV valves is also impaired. This cardiac defect results in a sizeable left-to-right shunt—the shunt increases in the first week of life when the pulmonary resistance drops.[39]
There is a risk of heart failure when the pulmonary resistance drops after 2–8 weeks of life. The situation is complicated due to (mainly systemic) AV valve insufficiency. AVSD is frequently associated with Trisomy 21 and is initially treated with avoidance of excess oxygen and pharmacological treatment of heart failure. The patient undergoes corrective surgery at 4-6 months, possibly earlier, if conservative treatment remains unsuccessful.
| Anesthetic and Hemodynamics Intraoperative Management Goals for Atrial and Ventricle Septal defect |
| 1) Maintain heart rate, contractility, and preload |
| 2) Maintain PVR: SVR ratio as an increase will cause the right-to-left shunt |
| 3) Avoid a decrease in PVR: SVR ratio as it may cause left-to-right shunt, decrease systemic perfusion and increase pulmonary blood flow |
Ventricular Septal Defect
Among all congenital heart defects, VSD is the most common. It has an incidence of 1.5 to 3 per 1000 term infants and 4.5-7 per 1000 pre-term infants. It is usually associated with chromosomal syndromes, which include trisomy 13, 18, and 21. Anatomically a ventricular septal defect (VSD) is an opening in the ventricular septum that allows communication between the right and left ventricle.
Its location classifies it into a subpulmonary or supracristal defect, membranous or perimembranous defect, conoventricular defect, inlet or canal type defect, and muscular defect. Physiologically it is a simple shunt, and the size of the defect determines the magnitude of shunting. Minor defects may be closed with cardiac catheterization; however, significant defects are usually closed with a patch surgically.[40]
Patients with unrepaired VSD may present for non-cardiac surgery with pulmonary hypertension and ventricular dysfunction later in life.[41] The anesthetic management goals are the same as those mentioned for the atrial septal defect.
Truncus Arteriosus
This cardiac defect comprises only one single vessel arising from the heart. It supplies systemic and pulmonary circulation and the coronaries. These neonates already have clinical signs of heart failure at birth due to excessive blood flow into the pulmonary circulation. The goals of initial management are;
- Restrictive use of oxygen administration as it lowers pulmonary resistance and increases blood flow to the pulmonary circulation
- Heart failure treatment: diuretics, possibly catecholamines (dobutamine) or phosphodiesterase inhibitor (milrinone), afterload reducer (ACE inhibitor, possibly sodium nitroprusside)
- Prostaglandin E1 infusion: initial dose 50 to 100 ng/kg/min[42]
The definitive corrective procedure is the Rastelli procedure, generally performed within the first weeks of life.[43]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain heart rate, contractility, and preload to maintain cardiac output |
| 2) Without pulmonary hypertension, avoid a reduction in PVR: SVR ratio. Ventilation with reduced FiO2 (<30%) and keep PCO2 between 35 to 40 mmHg. |
| 3) Use of inotropic support in patients with congestive cardiac failure. |
| 4) Use of ventilatory strategies to reduce PVR in patients with pulmonary hypertension. |
Total Anomalous Pulmonary Venous Return
This cardiac defect is characterized by drainage of all pulmonary veins into the systemic venous system, and the oxygenated blood reaches the right atrium. A right-to-left shunt at the atrial level is necessary for survival for perfusion of the systemic circulation.[44]
The condition with a total anomalous pulmonary venous return without obstruction has a hemodynamic situation similar to a significant atrial septal defect. It is initially managed by;
- Oxygen administration
- Intubation and ventilation
- Attempts to lower peripheral vascular resistance with hyperventilation, target pH 7.45 to 7.5, increase oxygen administration and inhale NO or prostacyclin IV.
- Diuretics and catecholamines for low cardiac output
This is an absolute cardiac surgery emergency without any delay. Sometimes dilatation with or without stent implantation can relieve the stenosis of the pulmonary vein in some instances so that the surgical repair can be performed after the patient is stabilized.[45]
If surgical correction is not possible immediately, the Rashkind maneuver, an interventional catheter balloon atrial septostomy, may be considered.
Left Ventricular Outflow Tract Obstruction
The neonates born with left ventricular outflow tract obstruction may have either critical aortic stenosis, coarctation of the aorta, or an interrupted aortic arch. Their initial management is standard:
- Shock management, including intubation and ventilation
-
Prostaglandin E1: initial dose 50 to 100 ng/kg/min
-
Oxygen: avoid excessive administration; use PEEP to improve oxygenation
-
Use diuretics to lower preload and pulmonary edema
-
Use catecholamines depending on blood pressure and myocardial function.
-
Assess by ECHO and reduce afterload
-
Aim for moderate metabolic acidosis (target pH 7.35)
-
Restrictive fluid therapy
Further management is prompt transfer to a pediatric congenital heart disease center and stabilizing the patient. Later palliative and surgical correction surgery is planned accordingly.[46]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain a sinus rhythm |
| 2) Maintain heart rate at baseline |
| 3) Maintain pulmonary artery occlusion pressure to maintain adequate left ventricular end-diastolic volume. |
| 4) Maintain afterload |
| 5) Maintain contractility |
Coarctation of Aorta
In coarctation of the aorta, the patient's lower half body is supplied with deoxygenated blood via the patent ductus arteriosus by the pulmonary artery. With the closure of the ductus arteriosus, there is dramatic hypoperfusion of the body distal to the aortic isthmus. The left ventricle suddenly contracts against the obstruction, followed by decompensation. There is an association with other cardiac defects, e.g., bicuspid aortic valve or VSD. These patients with critical coarctation of the aorta are immediately transferred to a pediatric cardiac center for surgical repair after stabilizing the hemodynamics.[47]
In unique case scenarios, balloon dilation by primary interventional catheterization or a coronary stent is performed to stabilize the patient due to poor condition or necrotizing enterocolitis.[48]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain heart rate, contractility, and preload. |
| 2) Continuation of prostaglandin E1 (0.01-0.05 microgram per min) to maintain ductal patency in neonates and infants. |
| 3) Reduction in PVR: SVR ratio in case of associated VSD or ASD. |
| 4) Avoid an increase in SVR. |
| 5) Cross-clamping of the aorta may produce proximal hypertension and left ventricular dysfunction |
| 6) Arterial line in the right arm. A pulse oximeter probe and non-invasive blood pressure monitor should also be applied to the lower extremity. |
| 7) Permissive hypothermia between 34 to 35 degrees centigrade |
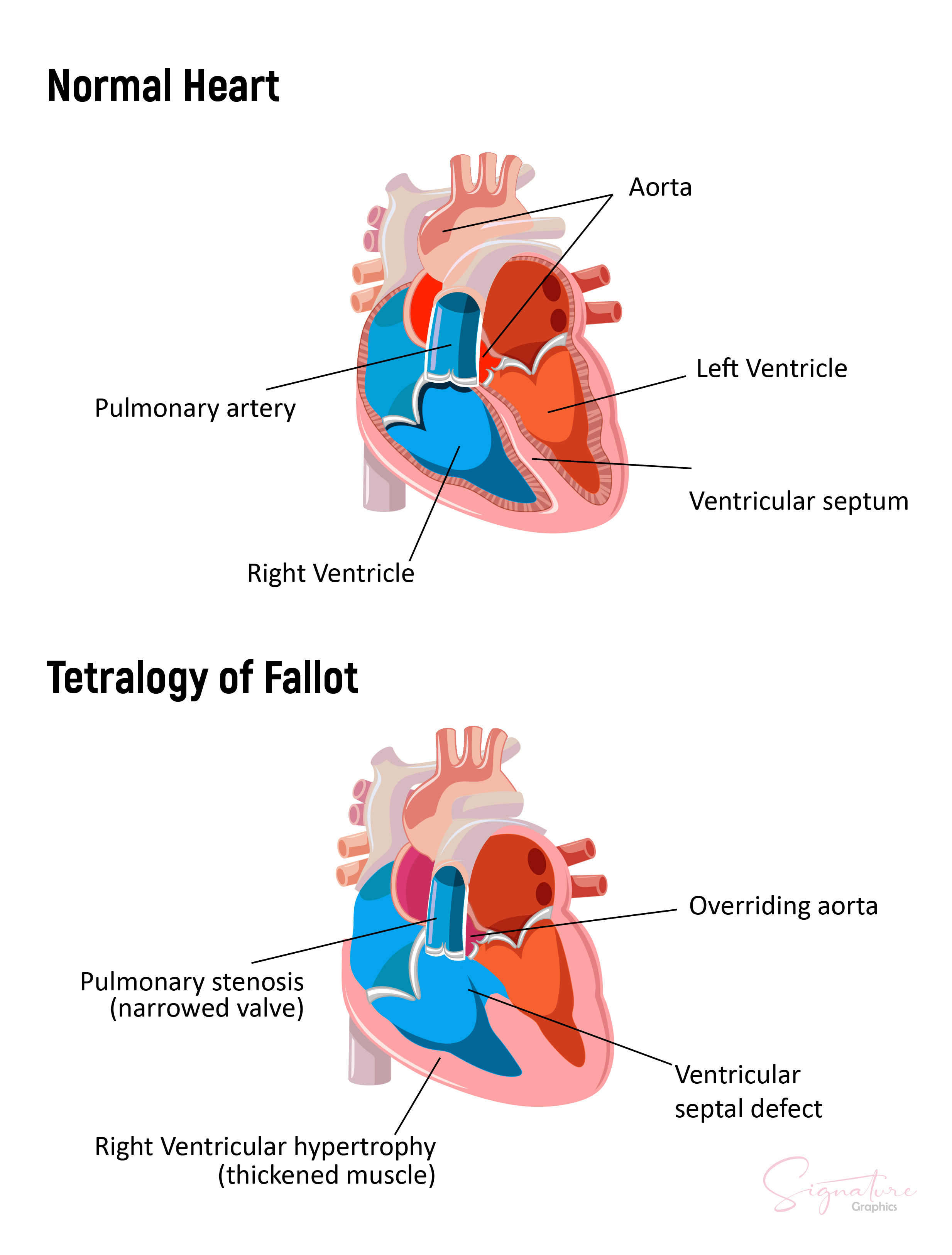
Tetralogy of Fallot
This cardiac defect combines a large VSD, an overriding aorta, pulmonary stenosis, and right ventricle hypertrophy. The grade of cyanosis depends on the extent of the right ventricle outflow obstruction. In most cases, the right outflow obstruction is mild at birth but becomes significant during the first weeks of life.
These children may develop hypercyanotic spells, also known as tet spells, due to a sudden increase in the obstruction of the right outflow tract either due to agitation or a sharp drop in peripheral vascular resistance, which may occur after feeding.[49]
Management of a hypoxic-hypercyanotic spell includes:
- Sedation with ketamine or opiates, benzodiazepines
- Oxygen application
- Increase peripheral systemic resistance by
- Jack-knife position- pressing the child's flexed knee against the chest
- Infusion of vasoconstrictors to increase peripheral vascular resistance
- generous volume bolus (e.g., 20 to 50 ml/kg)
- Compensation for metabolic acidosis by buffering
- Beta-blockers[50]
The patient should be transferred to a pediatric cardiac center as soon as the diagnosis is made. In most cases, patients undergo interventional procedures, including balloon dilatation of the pulmonary valve, stenting of the right ventricle outflow tract, and stenting of PDA that can improve the hemodynamic situation, except for a few cases where early surgical correction is required today.[51]
In certain exceptional conditions, a palliative procedure of an aortopulmonary shunt is first placed to ensure lung perfusion.[52]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain heart rate, contractility, and preload to maintain adequate cardiac output |
| 2) Avoid increase in PVR:SVR ratio |
| 3) Use of ventilatory interventions to reduce the pulmonary vascular resistance |
| 4) Maintain or increase the systemic vascular resistance |
| 5) Aggressive management of hypercyanosis episodes |
Transposition of Great Arteries
The transposition of great arteries (TGA) consists of a parallel connection between pulmonary and systemic circulation. The systemic blood is pumped back into the aorta, and the pulmonary blood is pumped back to the pulmonary artery. Survival is possible if there are shunts between the two circulatory systems, at the atrial level, e.g., patent foramen ovale or atrial septal defect, and at the ventricular level, presence of ventricle septal defect.
The patent ductus arteriosus has a favorable effect as it increases lung perfusion leading to increased left atrial pressure and volume load, causing an increase in a left-right shunt so that oxygenated blood can reach the systemic circulation.[53]
Patients with TGA are often treated with oxygen application that indirectly reduces pulmonary resistance and thus increases pulmonary perfusion. It increases atrial pressure and volume load. An attempt to improve mixed venous saturation should be made in "poor mixers." Cyanosis is usually less pronounced with a significant ventricular septal defect (VSD). The initial management of TGA includes
- Prostaglandin E1 infusion: initial starting dosage 50 ng/kg/min
- Volume therapy
- Mild metabolic alkalosis (pH 7.45 to 7.5, lowers pulmonary resistance)
- Oxygen application for severe cyanosis in neonates (caution: induces closure of the ductus arteriosus)
- Avoid intubation, mechanical ventilation, and muscle relaxation
- Consider using milrinone to improve cardiac output and thus mixed venous saturation
- Treat anemia to improve oxygenation
A bedside Rashkind maneuver, an interventional catheter balloon atrial septostomy, is done for a restricted atrial shunt as soon as possible.[54] The surgical standard repair is the Jantene Procedure, an arterial switch operation performed within the first two weeks of life.[55]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain heart rate, contraction, and preload. |
| 2) Maintenance of ductal patency with prostaglandin in ductal-dependent patients. |
| 3) Avoid increases in PVR relative to SVR. |
| 4) Avoid decreases in SVR relative to PVR. |
Tricuspid Atresia
In this cardiac defect, there is no continuity between the right atrium and right ventricle; instead, the right atrium drains into the left atrium through a right-to-left shunt at the atrial level. The tricuspid atresia has various forms that depend on obstructing the right ventricle outflow tract or pulmonary valve. The right ventricle is hypoplastic and is perfused by the left ventricle through a VSD. The oxygen saturation is the same in the aorta and the pulmonary artery because of the complete mixing of the blood.
In the case of high-grade stenosis or atresia of the pulmonary artery, perfusion of the lungs is dependent on patent ductus arteriosus. In the absence of pulmonary artery stenosis or atresia, congestive heart failure may develop later, which is much less common.[56] Initial management of heart failure with no pulmonary stenosis is
- Anticongestive treatment with diuretics, milrinone, and rarely catecholamines
- Restrictive oxygen therapy
- Restrictive volume therapy
Early transfer to a pediatric cardiac center for further management should be done. For a restrictive atrial shunt, the Rashkind maneuver is performed. For inadequate pulmonary perfusion, a palliative aortopulmonary shunt is usually placed. The separation of circulations is performed later by performing the Fontan procedure.[57]
| Anesthetic and Hemodynamics intraoperative Management Goals |
| 1) Continous infusion of PGE1 for ductal patency with ductal-dependent blood flow. |
| 2) Ventilatory targets of PaO2of 40-45mmHg and SaO2 of 70-80% for adequate systemic oxygen delivery. |
| 3) Use of ventilatory strategies to control and manipulate PVR. |
| 4) Hypercarbia (PaCO2 40-45 mmHg) |
| 5) Avoidance of high FiO2. |
| 6) Increase cardiac output with the use of inotropes. |
| 7) In un-intubated patients, denitrogenation with 100% oxygen prior to laryngoscopy and tracheal intubation. |
Ebstein's Anomaly
It is characterized by apical displacement of the tricuspid valve into the right ventricle with moderate to severe tricuspid regurgitation. It also causes decreased blood flow from the right ventricle into the pulmonary artery leading to the right atrium dilatation. It is usually asymptomatic in the neonatal period, and cyanosis occurs due to a right-to-left shunt at the atrial level. In addition to this, pulmonary function is grossly affected due to lung compression. This cardiac defect is often associated with Wolf-Parkinson-White syndrome (WPW). The initial management includes
- Management of congestive heart failure with catecholamines and diuretics
- Supraventricular tachycardia is managed with vagal maneuvers, antiarrhythmic, and cardioversion[58]
The surgical repair of the Ebstein anomaly should be done as soon as possible during the neonatal period as the prognosis is poor with congestive heart failure. The goal of surgical repair is a reconstruction of the tricuspid valve and closure of ASD. In case of reduced lung perfusion, an aortopulmonary shunt is placed.[59]
Sometimes, the Fontan procedure is the only option in case of a hypoplastic right ventricle.[60]
| Anesthetic and Hemodynamics Intraoperative Management Goals |
| 1) Maintain sinus rhythm |
| 2) Maintain heart rate at a faster rate |
| 3) Reduction of right ventricular afterload |
| 4) Maintain contractility |
| 5) Avoid hypercarbia, hypoxemia, and acidemia. |
| 6) Maintain cardiac output |
Other Issues
Surgery in Adults with Congenital Heart Disease
Except for the Bicuspid aortic valve, many patients with congenital heart defects, if they remain untreated, die in infancy or early childhood.[61] The survival of these patients to adulthood has only been made possible by recent advances in prenatal diagnosis, interventional cardiology, advanced pediatric cardiac surgery, anesthesia, and intensive care.[62] At some point in life, these patients may require either palliative or corrective surgeries or noncardiac surgeries during adulthood. Such patients with CHD present with complex and specific anatomy and physiology and pose a challenge in perioperative management.
A multidisciplinary approach is the essence of The preoperative evaluation of patients with CHD undergoing noncardiac surgery. The latest guidelines of the task force for safe delivery systems for patients with CHD recommend that the management of these patients should occur in an adult congenital heart disease center.[63] Adults with CHD risk perioperative complications, especially those with congestive heart failure, pulmonary hypertension, and cyanosis. Helpful information from echocardiography and cardiac catheterization helps the anesthesiologist anticipate intraoperative events and their prompt management.
Adults with CHD are usually psychologically affected due to previous exposure to anesthesia and complex cardiac surgeries. Premedication with anxiolytics and hypnotics should be done cautiously in the preoperative period. The American Heart Association's recent guidelines state that only patients with cardiac defects or conditions associated with a high risk for fatal outcomes should continue antibiotic prophylaxis before surgery.[64]
Utilizing conventional anesthetic techniques can easily manage adults with CHD if they have complete anatomic repair and have no evidence of functional deterioration. In contrast, patients with complex CHD and palliative or interventional procedures require specific intraoperative management. Anatomical and physiological concerns of specific palliative repairs are essential for choosing appropriate intraoperative monitoring. These patients have difficult vascular access due to previous vessel catheterization, and central venous access can be complicated with complex CHD. Transesophageal echocardiography might be helpful in adults with CHD undergoing noncardiac surgery to monitor intravascular volume status and ventricular function.[65]
The anesthetic management of patients with CHD for noncardiac surgery has no specific recommendations. Due to the enormous scope of CHD abnormalities, it is impossible to propose a single approach that may address each cardiac defect.[66]
The primary goal of intraoperative management is to promote optimal tissue oxygen delivery, the balance between systemic and pulmonary circulations, and the optimization of hematocrit. Knowledge of anesthetic agents is necessary to choose a specific volatile or intravenous anesthetic agent based on the patient's physiology and the overall intraoperative management goals. The use of etomidate and ketamine is well studied in these patients for induction of anesthesia as it maintains peripheral vascular resistance and ventricular performance.[67][68]
Anesthetic management is greatly affected by shunting. Patients with intracardiac shunts are prone to air embolization due to right-to-left shunting, so in that case, all intravenous lines should be de-aired before use. Anesthetic management aims to balance systemic and pulmonary blood flow by meticulously managing the hemodynamic effects of ventilation, positioning, pharmacological agents, and blood loss.
Cardiac intensive care units should postoperatively manage these patients with CHD and high-risk surgery. The significant risks during the postoperative period are bleeding, dysrhythmias, and thromboembolic events.
Enhancing Healthcare Team Outcomes
A healthcare team improves patient outcomes by creating conditions, resources, and a culture where clinicians can endeavor to make safe results. Our leaders must create an organizational climate in the healthcare field that ensures people acknowledge mistakes and inspires clinicians to innovate. Pediatric cardiac care is complex, and a tight coupling across the team in recognizing and responding quickly to appropriate errors and threats is critical in ensuring complete prevention-oriented recovery. The hallmark of providing harmonious performance and high reliability is supporting and building a culture of trust, transparency, and psychological safety.[69]
The primary responsibility of clinicians is to respect their patients and their families, improve safety and quality, and provide pediatric cardiac care by managing processes that optimize, standardize and continuously measure and monitor outcomes. A culture of certainty and collaboration within teams and institutions is essential for warranting data collection and devising mechanisms to report hazards and unsafe conditions.[70]
An essential tool that emerged over the past decade is a heart team; it includes a clinical cardiologist, cardiothoracic surgeon, anesthesiologist, nurse, nutritionist, pharmacist, physiotherapist, psychologist, and welfare service. The institution can modify the heart team with the incorporation of a pediatrician for pediatric cardiac care and a gynecologist/ obstetrician if a pregnant patient with congenital heart disease entails.[71][72] The overlap of expertise among different specialties helps in decision-making.
Improved communication between different healthcare disciplines helps reduce patients' length of stay and decreases morbidity and mortality. A systematic approach can enhance the delivery of quality evidence-based care in managing congenital heart diseases through leadership commitment from the anesthesiologist, cardiologist, and cardiac surgeon. Implementing a heart team for perioperative management of congenital heart diseases helps put numerous problems into perspective for sick patients and their families.
- A cardiologist's role in managing the patient's congenital heart disease is threefold 1) anatomical diagnosis, 2) interventional catheterization, and 3) role in decision-making for corrective surgery.[73]
- An interventional cardiologist performs cardiac catheterization to stabilize the patient and buy ample time for neonates before cardiac surgery.
- The cardiac surgeon in the heart team decides the optimal timing of the surgery and performs the necessary surgery.
- An anesthetist plays a fundamental role in evaluating anesthetic risks in the perioperative management of patients with congenital heart disease.
- A perfusionist manages the cardiopulmonary bypass circuit intraoperatively.
- An interventional radiologist helps diagnose the anatomical cardiac defect using various imaging modalities.
- An intensivist manages post-cardiac surgery period and non-cardiac complications, mechanical ventilator support, antimicrobial regimens, hemodynamic monitoring, and renal replacement.
- A clinical pharmacist's role is to provide evidence-based medication education for patients and healthcare professionals.
- A cardiac nurse has a significant role as a first-care responder and provides immediate care under the clinician's guidance.
- A physiotherapist is a critical member in leading cardiac rehabilitation programs.
- A pediatrician also holds an essential role in managing pediatric patients.
- A gynecologist/obstetrician may be involved when a pregnant patient with congenital heart disease presents.
Nursing, Allied Health, and Interprofessional Team Interventions
There is a clear distinction between a group of individuals working together and a team. Improving patient outcomes revolve around improving teamwork. The effectiveness of team performance in improving outcomes holds a shred of solid evidence in cardiac care. The most frequent contributor to adverse events is a lack of communication and teamwork. Team training and debriefing have been crucial in decreasing mortality to minimize the rate of adverse events.[74]
One of the many interventions ensuring multidisciplinary collaboration is the checklist, which has gained attention for improving patient safety. Substantial evidence supports the implementation of surgery checklists and other specialties.[75] The World Health Organization released the WHO Surgical Safety Checklist in June 2008, significantly decreasing mortality by using a modified version of the safety checklist in different setups.[76]
It is not about utilizing tools to improve quality endeavors but how these tools produce awareness, engage team members, provide feedback and pursue progress. The primary purpose of implementing checklists, safety protocols, and process maps are to help healthcare professionals function as a team and improve patient outcomes.
Nursing, Allied Health, and Interprofessional Team Monitoring
Working in an interprofessional healthcare team requires collaboration, cooperation, commitment, and communication. It should integrate care into teams to provide reliable and continuous care. All healthcare professionals, including nursing and allied, should be monitored for core competencies to meet the needs of the 21st-century healthcare system. They should be encouraged to employ evidence-based practice and participate in research and learning activities.
The institution should engage a monitoring team to apply quality improvement to identify the hazards and errors in care, implement safety protocols, and compose interventions to change care systems. Education is the key to patient-centered care to recognize and respect patients' differences, value their preferences, relieve pain and suffering, help decision-making, advocate disease prevention, and promote a healthy lifestyle.[77]