Continuing Education Activity
Production of cerumen (earwax) is a normal and naturally occurring process. It protects the ear from infection and provides a barrier to insects and water. Cerumen is typically expelled from the ear canal spontaneously via natural jaw movement. However, this self-cleaning mechanism fails in certain individuals, and cerumen can become impacted. Excessive buildup of cerumen is likely underdiagnosed and undertreated. It is most often diagnosed by direct visualization by a trained clinician using an otoscope but may require more complex equipment, such as an operating microscope, for removal. This activity describes the pathophysiology of cerumen impaction, reviews the technique involved in cerumen removal, and highlights the interprofessional team's role in managing affected patients.
Objectives:
- Describe the pathophysiology of cerumen impaction.
- Summarize the techniques available to remove cerumen.
- Outline the complications associated with the removal of cerumen.
- Explain the role of the interprofessional team in improving outcomes for patients with cerumen impactions.
Introduction
Production of cerumen (earwax) is a normal biological process in humans and many other mammals. Cerumen moisturizes the skin of the external auditory canal and protects it from infection, providing a barrier against the intrusion of water, foreign bodies, and even insects and other arthropods. Cerumen is typically expelled from the ear canal spontaneously as a result of normal jaw movement. However, this automatic clearing mechanism fails in specific individuals, and cerumen can become caught and impacted.[1]
Cerumen impaction can occlude the external auditory canal or press against the tympanic membrane, potentially causing ear fullness, conductive hearing loss, itching, and pain. Cerumen impaction is the most common ear complaint of patients to clinicians in the United States, occurring in up to 6% of the general population, affecting 10% of children and greater than 30% of the elderly and cognitively impaired. It is often seen in patients who routinely wear hearing aids or earplugs and those with exostoses or anatomic abnormalities of the external ear canal.[1][2]
Excessive buildup of cerumen is likely underdiagnosed and undertreated. In the United States, it leads to 12 million patient visits and eight million cerumen removal procedures each year. It can interfere with tympanic membrane examination as well as audiometry and hearing aid fitting. It is most often diagnosed by direct visualization by a trained clinician using an otoscope but may require more complex equipment, such as an operating microscope, for removal.[1][3]
Anatomy and Physiology
Keratin from shed skin cells accounts for roughly 60% of cerumen's mass, with the remainder composed of lipids and peptides secreted by the sebaceous and ceruminous glands of the lateral third of the external auditory canal.[1] More specifically, long-chain saturated and unsaturated fatty acids, alcohols, squalene, and cholesterol make up the acellular component.[4] The composition varies somewhat, with harder cerumen containing relatively more keratin than softer cerumen. Impacted cerumen may also contain neutrophils and has a much higher likelihood of bacterial or fungal colonization.[5]
In one study, every sample of cerumen from patients with recurrent impactions showed evidence of fungal growth, most commonly Aspergillus terreus; when bacteria are present, Staphylococcus aureus is most common.[5] While there is a certain baseline rate of cerumen production, frequent insertion of foreign objects into the external auditory canal, such as cotton swabs and certain types of hearing aids or earbuds, will often accelerate the production of cerumen and potentially change its composition. Similarly, placing cotton swabs into the ear canals to address pruritus is liable to increase cerumen production and exacerbate the itching.
Indications
Although excessive accumulation of cerumen is typically asymptomatic, patients should be treated if they present with hearing loss, ear fullness, pruritus, dizziness, tinnitus, or otalgia. The inability to examine an ear by otoscopy, particularly an ear with other symptomatology, such as hearing loss, tinnitus, pain, or vertigo, due to cerumen impaction is also an indication for cerumen removal.[1] Another common reason to remove cerumen is to facilitate audiometric examination, which often includes immittance tympanometry, and this cannot be performed in the presence of complete external auditory canal occlusion because it involves using air pressure pulses to calculate the volume of the external auditory canal and the compliance of the tympanic membrane. Cerumen impactions may make routine surveillance of otologic conditions, like cholesteatoma, more challenging as well; some patients with chronic otologic conditions, such as open mastoid bowls after surgery for cholesteatoma, will require routine cerumen removal for regular surveillance examinations, and this is best performed by the surgeon who performed the original operation.
When encountered in an asymptomatic patient, it is not always necessary to treat a cerumen impaction. It is important to explain to patients that cerumen does not always need to be removed, as cerumen naturally has bacteriocidal, protective, and emollient properties. Unless symptomatic, patients should be encouraged to leave their cerumen alone. Observation should be offered as a management strategy, if appropriate.
In young children, the elderly, schizophrenic, or cognitively impaired individuals, treatment is a reasonable option because these patients may not be able to verbalize, perceive, or attend to concerning symptoms, significantly worsening their quality of life.[6][7][8]
Contraindications
There are no absolute contraindications to cerumen removal. Clinicians should exercise caution when removing cerumen in patients with certain immunosuppressive illnesses (HIV, diabetes mellitus, transplant patients, etc.), chronic anticoagulation, or anatomical anomalies that narrow the canal, as they may be prone to complications from manual removal. In patients with diabetes mellitus, a higher pH is typically present in the cerumen, making superimposed bacterial infections more common. Immunosuppressed patients are at higher risk of infection after even minor trauma, so meticulous atraumatic technique should be used during cerumen removal. Additionally, this population is at higher risk for malignant otitis externa, which can mimic cerumen impaction or aural polyps to the inexperienced examiner. Caution should be exercised in chronically anticoagulated patients who are at a higher risk for hemorrhage or hematomas. Irrigation should not be utilized as a method for cerumen removal unless the tympanic membrane can be visualized first to rule out perforation.[9][10]
Use of cerumenolytics (see below) is safe, but contraindications include a perforated tympanic membrane or a history of ear surgery, including tympanostomy tube placement. Common reactions include local irritation and a rash. With prolonged use, a superinfection may occur.[11]
Equipment
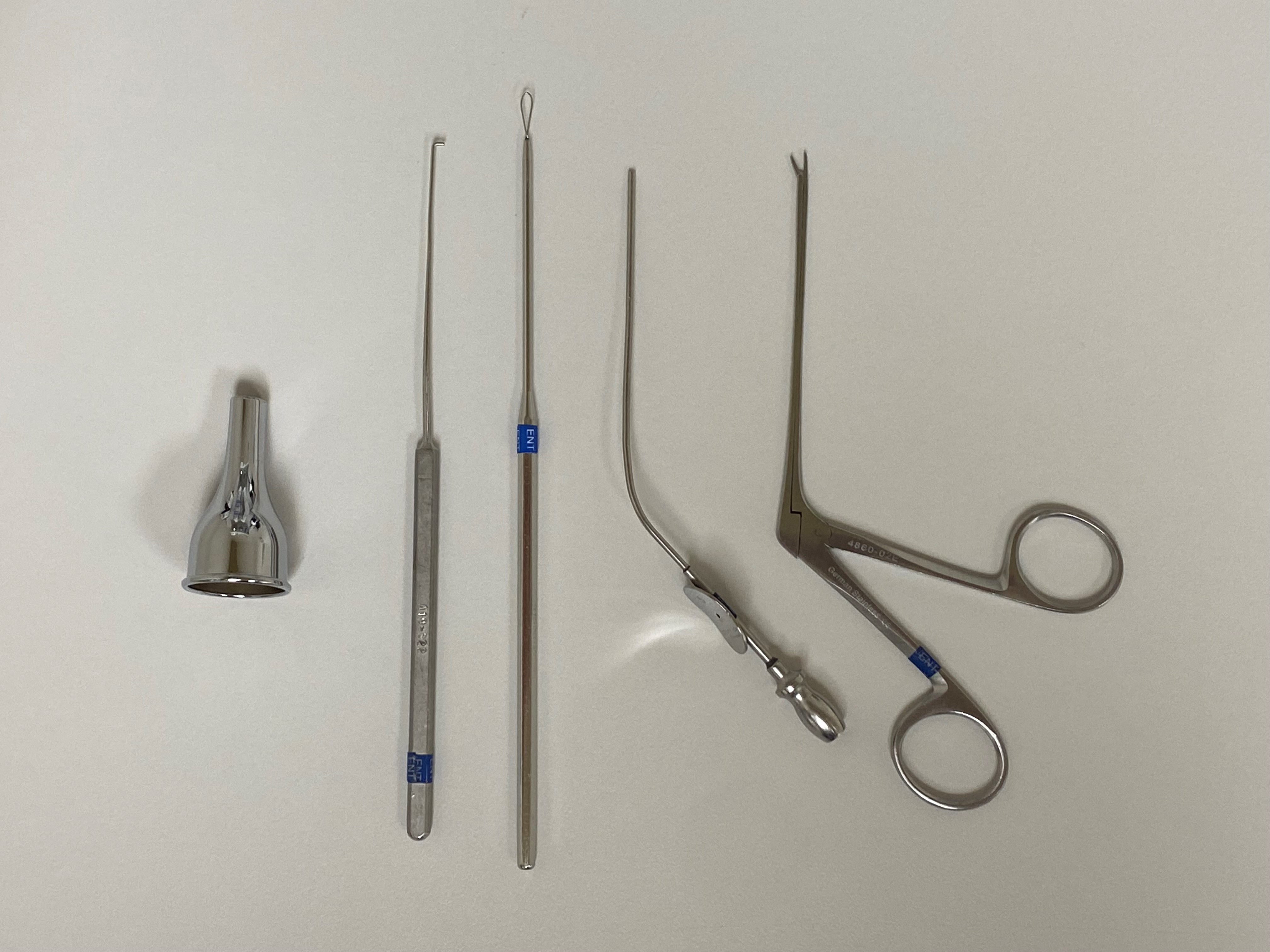
For the removal of cerumen in a cooperative patient without an anatomic abnormality, a cerumen curette and an otoscope are usually sufficient, and gentle irrigation with saline in a syringe may prove to be a useful adjunct. Cerumen that is particularly soft or hard may require additional instrumentation, such as a fine suction tip (5 Fr Frazier tip or similar), right-angle hook, or alligator forceps. When advanced instrumentation is required, an operating microscope and an otologic speculum will facilitate the procedure; at this point, cerumen removal will typically require an otolaryngologist or an otolaryngology technician.
Personnel
Simple cerumen removal may be performed by an emergency physician, a primary care provider, a nurse, or a technician. When anatomical abnormalities - congenital, post-traumatic, post-operative, or neoplastic - make removal more complicated, the expertise of an otolaryngologist or otolaryngology technician may be required. For some patients, such as children and the cognitively impaired, general anesthesia may be necessary in order to prevent movement during the procedure and limit the risk of damage to the external auditory canal and middle ear structures. Lastly, smaller children that require cerumen removal may be able to be placed in a papoose for restraint rather than requiring general anesthesia or sedation. Even so, holding these patients still will often require the efforts of a parent and/or an assistant to the clinician.
Preparation
Counseling the patient before cerumen removal is important, primarily to secure cooperation during the procedure to limit movement and subsequent injury to the external auditory canal, tympanic membrane, and middle ear structures. Patients should be aware of the risk of pain, bleeding, and damage to the aforementioned structures, with the potential loss of hearing. Some patients are very sensitive, and the sensitivity of the external auditory canal skin typically increases closer to the tympanic membrane, which is itself very sensitive to pain with only minimal contact. Due to the presence of terminal branches of Arnold's nerve (a branch of the vagus nerve) supplying sensation to parts of the external auditory canal, some patients may cough or even gag; the clinician should be prepared to remove the instruments from the ear canal swiftly if this occurs, and the patients should be made aware that it is a possibility.[12]
Technique or Treatment
When treatment is appropriate, there are three recommended removal methods: cerumenolytic agents, irrigation, and manual removal.[11]
Cerumenolytic agents are liquid solutions that help thin, soften, break up, and/or dissolve ear wax. These are typically water- or oil-based compounds, with water-based solutions being the most commonly used. Typical ingredients found in water-based cerumenolytics include hydrogen peroxide, acetic acid, docusate sodium, and sodium bicarbonate. Docusate sodium appears to be the most effective, particularly when used as a pre-treatment before irrigation.[13] Common ingredients in oil-based cerumenolytics include peanut, olive, and almond oils. Most drops are available over the counter. Typically, up to five drops are used per dose, one to two times daily for three to seven days.
A commonly prescribed cerumenolytic is carbamide peroxide. Five to 10 drops are placed twice daily for up to four days. The drops work by releasing oxygen to soften and encourage spontaneous extrusion of cerumen and also have a weak antibacterial effect.
Irrigation is another method to safely and effectively remove unwanted cerumen, provided the tympanic membrane can be visualized first. Several irrigation methods may be used in the clinical setting. Commonly, warm water alone or a 50/50 mix of water and hydrogen peroxide is placed into a syringe and discharged into the ear canal with a basin underneath. It is important to use water that is similar to the patient's body temperature because overly warm or overly cool fluid can cause a convection current in the semicircular canals and result in vertigo, particularly if there are pressure equalization tubes or a tympanic membrane perforation present; this is the mechanism behind caloric testing of the vestibular system.
An alternative to using a syringe is a standard oral jet irrigator, with or without a modified tip. Although these methods are inexpensive and generally safe, they can be potential causes of trauma, including perforation of the tympanic membrane. Electronic irrigators are also available; however, there are no controlled trials to compare the different irrigation methods. Regardless, it appears that ear irrigation is less effective than manual removal under visualization in patients over the age of 70 years.[13]
Manual removal is the final method recommended by the American Academy of Otolaryngology-Head and Neck Surgery to remove unwanted cerumen. Manual removal often requires specialized instrumentation for better visualization, such as a binocular microscope and a handheld speculum. Cerumen removal may involve a metal or plastic loop or spoon, curette, or alligator forceps. Some products have illuminated tips to improve visualization during the procedure. The advantage of this method is a decreased risk of infection because the ear canal is not exposed to moisture. However, it does pose a small risk of perforation and local trauma, especially if the patient is uncooperative or the clinician is inexperienced. This method requires more clinical skills and greater cooperation from the patient, especially when anatomical anomalies are present, such as exostoses or a mastoid bowl.
To prevent further accumulation of cerumen in patients with recurrent cerumen impactions more often than once per year, patients may apply mineral oil to the external canal for 10 to 20 minutes weekly. Patients with hearing aids should remove them for eight hours daily to reduce cerumen buildup.[14][15]
Complications
There are several over-the-counter devices to remove cerumen that patients should be advised not to purchase. Cotton swabs are commonly used but should be avoided, as they may worsen the impaction or cause a perforation of the tympanic membrane. Another common home remedy is ear candling. This involves a hollow tube coated in beeswax; one end is inserted into the ear canal, and the other is ignited. It is falsely claimed to have a "chimney effect," created by the pull of air from the ignited candle. The United States Food and Drug Administration strongly recommends against using this device because it has not been shown to be effective in scientific studies but does carry the potential for injury.[3][14]
Clinical Significance
It is crucial to ensure symptoms of other conditions are not falsely attributed to the cerumen in patients treated for cerumen impaction. The list of common presenting complaints of cerumen impaction is long and somewhat nonspecific, including symptoms with many different causes, such as otalgia, tinnitus, dizziness, hearing loss, aural fullness, ear itching, and foreign-body sensation. Once the cerumen impaction is removed, it is important to rule out comorbid conditions, such as Eustachian tube dysfunction, otitis media, otosclerosis, sensorineural hearing loss, temporomandibular joint syndrome, and upper respiratory tract infections, etc., via further examination and testing if symptoms persist.[1]
Enhancing Healthcare Team Outcomes
Cerumen impaction is rarely challenging to treat but requires a coherent and cooperative patient to be successful. If the patient is unwilling or unable to participate and cooperate in treatment, removing impacted cerumen and otologic examination can be performed under general anesthesia or conscious sedation. Anesthesia is typically only necessary in the very young or in those patients whose neurocognitive and neurobehavioral status prevents safe treatment while fully awake.[16]
This procedure, while straightforward, still requires the efforts of an interprofessional team, including family clinicians, otolaryngologists, and nursing staff, depending on the complexity of the specific case. Every interprofessional team member must maintain open communication with other team members and maintain accurate records of their interactions and inventions with the patient. This interprofessional approach will yield optimal results with the fewest adverse events. [Level 5]