Introduction
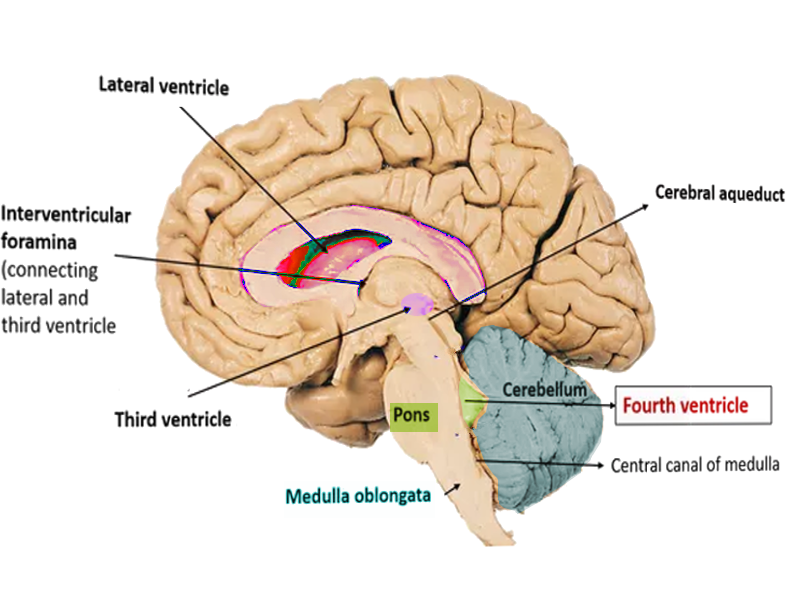
The ventricles of the brain are the sites of cerebrospinal fluid (CSF) production. The lateral ventricles are the largest, and most proximal, ventricles in the central nervous system (CNS). CSF produced in the lateral ventricles goes into the interventricular foramen of Monro. The interventricular foramen of Monro connects the lateral ventricles to the third ventricle. The third ventricle connects to the fourth ventricle through the cerebral aqueduct of Sylvius. CSF flows through this entire pathway and then exits the fourth ventricle into the surrounding CNS tissue or the central spinal canal. This article will focus on the anatomy, function, and clinical relevance of the fourth ventricle.[1]
Structure and Function
The function of the ventricles of the brain is to produce and transmit CSF fluid into the spinal canal, ventricular system, and the subarachnoid space. The choroid plexus produces the majority of CSF, along with the ependymal cell layer of the ventricles and cells lining the subarachnoid space.[2][3] Although the lateral ventricles produce the most CSF due to their larger surface area, CSF gets produced in all of the ventricles. CSF provides physical support to the brain, absorbs shock during trauma, keeps neurons in homeostasis, provides nutrition, and contains immune cells to help fight off infections of the nervous system.[1]
The fourth ventricle is the most inferiorly located ventricle, draining directly into the central canal of the spinal cord. Superiorly, it connects to the third ventricle through a thin canal called the cerebral aqueduct of Sylvius. It is surrounded anteriorly by the pons and medulla, posteriorly by the cerebellum, and inferiorly by the spinal canal and spinal cord. At its superolateral portions, two channels drain CSF into the surrounding neural tissue. These are called the lateral apertures, or the foramina of Luschka. Inferomedially is the median aperture or the foramen of Magendie. These apertures help spread CSF around the spinal cord and the surrounding neural structures. All of the CSF that does not drain out of these apertures goes into the central canal of the spinal cord.
The lateral wall of the fourth ventricle is surrounded inferolaterally by the cuneate and gracile tubercules, along with the inferior cerebellar peduncles. The lateral wall is also surrounded superolaterally by the superior cerebellar peduncle. The dorsal wall, or roof of the fourth ventricle, is formed by two cerebellar peduncles that are bridged together by a thin sheet of white matter called the superior medullary velum. The floor of the fourth ventricle forms from the posterior surface of the pons and the superior medulla.[4]
Embryology
In neuroembryology, the neural tube forms around the fourth week of gestation. The center, hollow portion of the neural tube eventually develops into the ventricular system. Three dilations, called the prosencephalon, mesencephalon, and rhombencephalon, form from the neural tube. The prosencephalon, or the forebrain, develops into the telencephalon (cerebral hemisphere) and the diencephalon. The mesencephalon becomes the midbrain, while the rhombencephalon grows into the metencephalon (pons and cerebellum) and the myelencephalon (medulla). Within each of these dilations that develop from the neural tube are cavities that become the ventricles. The cavity located in the rhombencephalon becomes the fourth ventricle.[4]
Blood Supply and Lymphatics
The choroid plexuses are highly vascularized epithelial tissue masses that contain fenestrated blood vessels. Besides producing CSF, they are the main structural components of the blood-brain barrier. Along with providing structural support to the blood-brain barrier, they also offer a biochemical barrier, releasing toxins and drugs taken up by cells in the blood-CSF barrier.[3]
The arteries that supply the choroid plexus of the fourth ventricle originate from multiple areas of the cerebellar arteries and pass by the pons and medulla. One study showed that the posterior inferior cerebellar artery (PICA), anterior inferior cerebellar artery (AICA), and the superior cerebellar artery (SCA) supplied the majority of blood flow to the fourth ventricle choroid plexus. The AICA was responsible for supplying the plexus near the cerebellopontine angles, as well as a portion of the lateral recess of the fourth ventricle into the lateral apertures. The PICA supplied the choroid plexus in the median aperture and roof of the fourth ventricle.[5]
Surgical Considerations
As discussed earlier, many important structures surround the fourth ventricle, namely the pons and medulla of the brainstem, as well as the cerebellum. This anatomic arrangement makes accessing the fourth ventricle very difficult, especially when trying to remove a tumor without severely impacting the rest of the surrounding brain.
In the past, access to lesions of the fourth ventricle was through the cerebellar cortex by opening the cerebellar vermis; this was called the transvermian approach. However, this was shown to lead to disturbances of equilibrium and cerebellar mutism, most likely from damaging the median and paramedian cerebellar structures.[6]
Now, a method called the telovelar approach is gaining favor; this is performed by accessing the fourth ventricle through the cerebellomedullary fissure, a space between the cerebellum and medulla oblongata. This functions as a natural track into the ventricular cavity. The tela choroidea and the inferior medullary velum, which make up part of the roof of the fourth ventricle, come into visualization and can be opened after elevating the cerebellar tonsils. This approach allows surgeons to access the fourth ventricle without dissecting through neural tissue, thus causing less damage.[6] It is important that after these types of surgeries, an external ventricular drainage (EVD) device is kept in for 2 to 3 days to check on intracranial pressures and facilitate wound closure. After this, the EVD is closed for 2 days, and then a CT scan of the head is performed to measure ventricle size and assess if there is hydrocephalus or leakage into the brain.[7][8][7]
Clinical Significance
When considering clinical pathologies of the fourth ventricle, they will usually present due to increased amounts of CSF fluid in that ventricle. This state can occur due to increased production of CSF fluid from the fourth ventricle choroid plexus, or an obstruction of CSF flow out of the ventricle. The majority of the clinical significance of the fourth ventricle relates to these phenomena and how they will impact the nervous system around it. It is imperative to rule out fourth ventricle compression/obstruction in patients with a sudden loss of consciousness.
Ependymomas are the third most common pediatric brain tumors but only account for 1.9% of adult primary brain tumors. They are CNS malignancies that originate from the ependymal cell lining of the ventricles. Many different types of ependymomas differ in location and histopathology. Subependymomas, also known as WHO grade I ependymomas, mostly occur within the fourth ventricle or the lateral ventricles. They are characterized histologically by a nodular pattern with zones of increased nuclear density or fibrillary stroma.[9] Although these tumors are very treatable, there are often lasting morbidities from surgery to remove these tumors.[10]
Hydrocephalus is the presence of too much CSF in the brain, which often results from a problem with CSF absorption that occurs after an insult has impaired the arachnoid granulations from correctly reabsorbing fluid. This condition is called “communicating hydrocephalus” because CSF is still able to flow throughout the ventricular system, but it is not getting absorbed as efficiently as it needs to be. Conversely, a blockage in the ventricular system by a tumor or cyst will cause “obstructive hydrocephalus,” or noncommunicating hydrocephalus. This means that there is obstruction of the flow of CSF, so it becomes trapped in the ventricles causing swelling of the ventricles proximal to the lesion.[11]
A condition called fourth ventricle outlet obstruction (FVOO) is a type of noncommunicating hydrocephalus that occurs when there is a disconnect between the subarachnoid space and the ventricular system. This can result from a tumor or cyst blocking the lateral or median apertures and will cause enlargement of the entire ventricular system since this is the distal-most ventricle. It is also often caused by inflammatory processes following hemorrhage, infectious disease, or congenital anomalies of the fourth ventricle. To diagnose FVOO, additional studies such as those on a three-dimensional constructive interface in steady-state (3D-CISS) are often necessary.[12]
Dandy-Walker malformation (DWM) or syndrome characteristically demonstrates a cystic enlargement of the fourth ventricle and agenesis or hypoplasia of the cerebellar vermis. Most patients will present with hydrocephalus, but it often remains clinically asymptomatic for years. It can either be isolated or associated with Mendelian disorders, syndromic malformations, chromosomal abnormalities, and congenital infections. CNS disorders associated with DWM include holoprosencephaly, neural tube defects, and dysgenesis of the corpus callosum.[13][13][13]