Continuing Education Activity
Individuals with an intellectual disability have neurodevelopmental deficits characterized by limitations in intellectual functioning and adaptive behavior. This activity reviews the evaluation and management of intellectual disability, including the genetic and environmental etiologies of intellectual disability, various disease manifestations, and appropriate evaluation strategies. This activity also highlights the needs of individuals with intellectual disabilities and suggests an interprofessional approach to the management of intellectual disability, and recognizes the interprofessional team element in managing these cases.
Objectives:
- Summarize the epidemiology of intellectual disability.
- Outline the etiology of intellectual disability.
- Explain the treatment considerations for patients with intellectual disabilities.
- Review the importance of improving care coordination amongst the interprofessional team to enhance the delivery of care for patients affected by intellectual disability.
Introduction
Individuals with an intellectual disability have neurodevelopmental deficits characterized by limitations in intellectual functioning and adaptive behavior. These disabilities originate at birth and manifest before the age of 18 and can be associated with a considerable number of related and co-occurring problems, including mental health (e.g., depression and anxiety), neurodevelopmental (e.g., autism spectrum disorders, and attention deficit hyperactivity disorder), as well as neurological (e.g., infantile cerebral palsy) and medical conditions (e.g., meningitis).
Intellectual Functioning
Intellectual functioning is generally called intelligence and includes a wide range of mental activities such as the ability of logical reasoning and practical intelligence (problem-solving), ability in learning, verbal skills, and so on. It manifests and expresses itself through numerous sets of capabilities, behaviors, thoughts, and emotions. In other words, intellectual functioning is definable as the global ability that allows the individual to understand reality and interact with it.
Intellectual functioning is commonly measured by the intelligence quotient (IQ), which represents a total score obtained from standardized tests (IQ tests) developed for evaluating human intelligence. IQ test score has a median of 100 and a standard deviation of 15. A score of 70 or below (two standard deviations below the median) indicates intellectual limitations.
Adaptive Behavior
These disabilities express as lacking competence in social, conceptual, and practical skills. Social skills include interpersonal skills, social responsibility, self-esteem, gullibility, naivety, resolution of social problems, and the ability to follow the rules of society and obey the laws. Conceptual skills include the ability to understand time, finance, and language. Practical skills include the ability to use tools, carry out activities of daily living, and interact with other people. All these skills are learned throughout development and performed in response to common problems and simple/complex tasks, as well as expectations from our community and society. Obviously, these behavioral responses become progressively more complex with age. Several validated tools are useful for assessing limitations in adaptive behavior.
Etiology
While many causes of intellectual disability are not known, the etiology of intellectual disability mainly divides into genetic abnormalities and environmental exposure. Genetic abnormality can be a single gene mutation, copy number variation, or chromosomal abnormality that causes an inborn error of metabolism, neurodevelopmental defect, and neurodegeneration. Environment exposure can be maternal exposure to toxin/infectious agents, uncontrolled maternal medical conditions, delivery complications, and post-natal trauma and exposure to toxin/infectious agents. The most common known preventable or environmental cause of intellectual disability is fetal alcohol syndrome, the most common chromosomal cause is Down syndrome, and the most common genetic cause is Fragile X syndrome.
Genetic
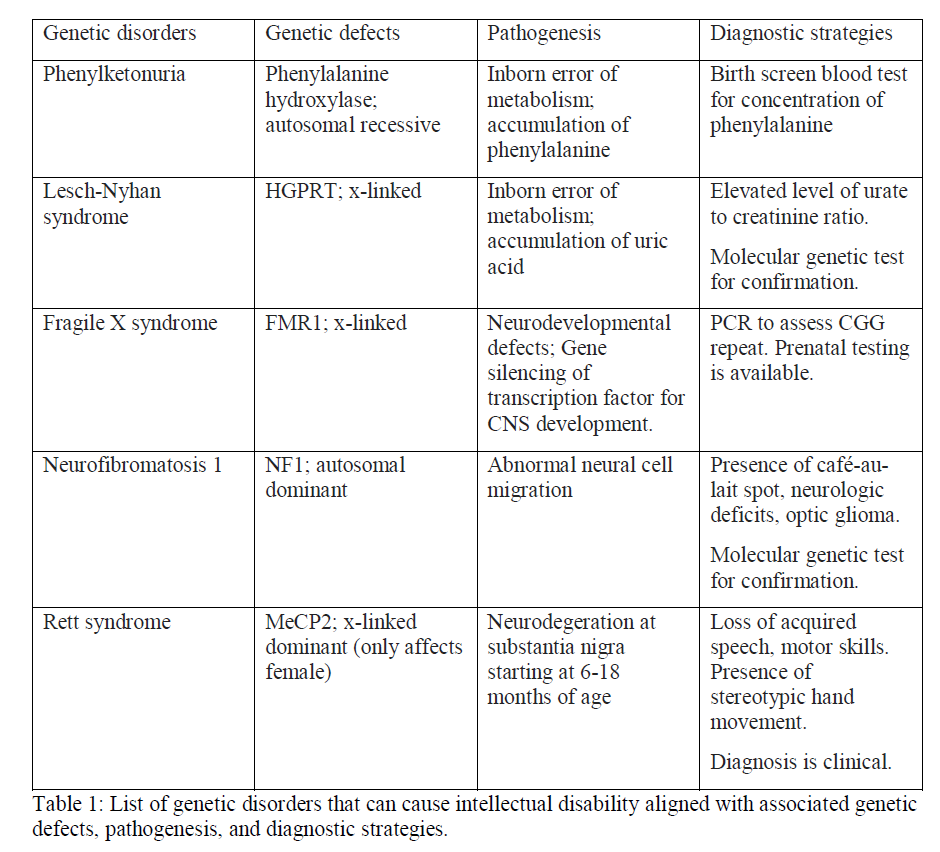
The genetic abnormality may cause an inborn error of metabolism, neurodevelopmental defect, or neurodegeneration. With an inborn error of metabolism, toxic by-products accumulate, causing intellectual disability and other behavioral problems. Phenylketonuria (PKU) is one of the inborn errors of metabolism that occurs in approximately 0.01% of newborns. PKU most commonly results from phenylalanine hydroxylase defect inherited in an autosomal recessive fashion. The defect disables the liver from converting phenylalanine to para-tyrosine. The consequent accumulation of phenylalanine is the culprit of intellectual disability. Neurological damage from PKU is irreversible but preventable. Therefore, newborn screening for PKU is mandatory in the U.S. and other countries. Early screening followed by prompt initiation of a low phenylalanine diet before the age of 3 may prevent intellectual disability.[1] Recently, different rare types of hyperphenylalaninemia were described, including the deficiency of the enzyme dihydropyridine reductase and a deficiency of a cofactor, biopterin.[2]
Lesch-Nyhan syndrome is an X-linked inborn error of metabolism caused by purine metabolism enzyme deficiency. This condition results from a mutation in HGPRT.[3] This mutation leads to a buildup of uric acid, which causes severe self-mutilating behavior of biting mouth and finger as well as intellectual disability.[4] Other known inborn errors of metabolism that result in intellectual disability are Niemann-Pick disease, Hunter disease, Hurler disease, maple syrup urine disease, Hartnup disease, homocystinuria, and galactosemia.
A neurodevelopmental defect presents in Fragile X syndrome, a leading genetic cause of intellectual disability. It results from a single gene mutation in the FMR1 (Xq27.3) gene. In most cases, CGG repeat of the FMR1 gene expands to over 200 times. The expansion leads to a phosphorylated CG pattern, causing methylation imprinting of the gene, thereby silencing FMR1 gene expression. FMR1 is a transcription factor of hundreds of genes expressed in the central nervous system, and its disruption causes intellectual disability as well as behavioral disturbance, and seizure.[5] Neurodevelopment defect also presents in neurofibromatosis type 1, also known as von Recklinghausen syndrome, an autosomal dominant condition caused by mutations of NF1. Its characteristic presentation is abnormal neural cell migration leading to cafe au lait spot, movement disorder, and intellectual disability.[6]
Neurodegeneration leading to intellectual disability presents in Rett syndrome (RS), an X-linked dominant degenerative condition only seen in females secondary to mutation of the MeCP2 gene. In patients with RS, cerebral atrophy occurs at the substantia nigra, causing defects in the dopaminergic nigrostriatal pathway, starting at 6 to 18 months of age.[7]
IQ alterations can also occur as part of a clinical picture in other genetic syndromes. In many cases, the intellectual deficit appears to be limited and can occur at different stages of neurodevelopment, also in terms of cognitive decline. For example, in chromosome 22q11.2 deletion syndrome, DiGeorge syndrome, or velocardiofacial syndrome, which is one of the most common multiple anomaly syndromes in humans, is usually described as a cognitive decline rather than an early onset intellectual disability.[8]
Environmental
Environmental exposure during pregnancy may lead to intellectual disability, which can be caused by maternal exposure to a toxin, infectious agent, uncontrolled maternal condition, and birth complications.
One common toxic substance that leads to an intellectual disability during pregnancy includes alcohol. Alcohol exposure, indeed, commonly causes intellectual disability along with other developmental abnormalities, in a condition known as fetal alcohol syndrome.[9] Fetal exposure to alcohol inhibits the production of retinoic acid, which is an essential signaling molecule for the development of the nervous system. Even a small amount of alcohol in any trimester of pregnancy may cause fetal alcohol syndrome.[10]. Exposure to opioids, cocaine, and teratogenic medications may also lead to intellectual disability.
Common, well-known infectious agent that causes intellectual disability are rubella and HIV. Maternal rubella infection in the initial trimester of pregnancy leads to intellectual disability approximately 10 to 15% of the time; it can rise to above 50% with infection during the first month. Immunization may prevent the mother from rubella infection.[11] HIV may be transferred vertically from mother to infant. Infants with HIV may develop encephalopathy, seizures, and intellectual disability within the first year of life secondary to microcephaly, immunosuppression, and Pneumocystis jiroveci pneumonitis (PCP) infection.[12] Excessive neuro-inflammation causes overstimulation of the N-methyl-D-aspartate type receptor (NMDAR) system, which leads to neuronal injury. Antiretroviral therapy for the mother and prophylactic treatment with zidovudine for newborn exposed to HIV has significantly reduced the transmission.[12] Other known infectious exposures to mothers that may cause intellectual disability in the newborn are cytomegalic inclusion disease, syphilis, and toxoplasmosis.
Uncontrolled maternal medical conditions may lead to intellectual disability. Pregnancy hypertension, asthma, urinary tract infection, pre-pregnancy obesity, and pre-gestational diabetes were shown to increase the risk significantly.[13] Furthermore, uncontrolled maternal diabetes, malnutrition, and obstetrical complications causing anoxia (placenta previa, placenta abruption, and umbilical cord prolapse) may also cause intellectual disability.[14]
An intellectual disability is acquirable during early childhood. Causes include infection (notably encephalitis and meningitis), head trauma, asphyxia, intracranial tumor (either directly or indirectly through seizure, surgery, and chemotherapy), malnutrition, and exposure to toxic substances.[15]
Epidemiology
The prevalence of intellectual disability in developing countries is estimated to range from 10 to 15 per 1000 children; of those, about 85% have a mild intellectual disability. From 1 to 3% of the Western population is estimated to have an intellectual disability. Incidence is challenging to accurately calculate as mild disabilities may be under-recognized until later in childhood. Intellectual disability is reported to peak at the ages of 10 to 14 years and is 1.5 times more prevalent in males than females.[16]
History and Physical
Keeping up with daily functions is often challenging for individuals with different degrees of intellectual disability. They may have difficulty feeding themselves, going to the bathroom, and dressing. They also may have difficulty getting along with their family and friends because of a problem with communication as well as poor impulse control. They may have trouble excelling academically and socially at school.
Concerning clinical history, symptoms of intellectual disability usually begin during childhood or adolescence. Moreover, delays in language or motor skills may be observed by age two. Nevertheless, a significant number of children with mild levels of intellectual disability may not get identified until school age.
A comprehensive history of patients with intellectual disability must include the following:
- Information about the mother’s pregnancy, labor, and delivery
- Mother’s use of substances or medications during pregnancy
- Mother suffered any uncontrolled medical condition
- Was delivery pre-term?
- Was there any issue with delivery?
- Patient’s sensory, social, language, and motor developments to detect any developmental delay
- Patient’s exposure to infection, trauma, and toxin
- Patient’s medical conditions
- Patient’s psychiatric conditions
- Medications that the patient is taking
- Patient’s family history of psychiatric and medical conditions
- Patient’s living situation, caretaker
- Patient’s behavior toward caretaker, parents, and siblings
- Patient’s academic performance at school
- Patient’s behavioral disturbance reported at school
Physical examination is vital to differentiate intellectual disorders from other conditions. A full neurological exam should be performed to identify any deficit that may mimic intellectual disability and comorbid symptoms. Visual and hearing tests are particularly important as abnormal vision or hearing causes difficulty with communication, leading to a delay in developing language and social skills, closely mimicking intellectual disability. Motor dysfunctions such as spasticity, hypotonia, hyperreflexia, and involuntary movements are commonly present in individuals with intellectual disabilities.[17]
Some physical characteristics are closely associated with a specific diagnosis as follows:
- Down syndrome: slanted eyes, flat nasal bridge, protruding tongue, small chin, and single crease palm
- Fragile X syndrome: long and narrow face, prominent forehead and jaw, large ears, and large testicles in male
- Fetal alcohol syndrome: smooth philtrum, thin vermilion, and small palpebral fissures
- Prader-Willi: obesity secondary to compulsive eating behavior, hypogonadism, small hands, and feet
- Cat’s cry (Cri-du-chat) syndrome: microcephaly, hypertelorism, low-set ears, and micrognathia
- Phenylketonuria: bizarre movements such as twisting hand mannerisms, poor motor coordination, and perceptual difficulties
Evaluation
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), the diagnosis of intellectual disability requires deficits in intellectual function, deficits in adaptive function, and onset before the age of 18. The IQ test is widely used to assess the intellectual function of individuals. IQ test derives from Stanford-Binet Intelligence Scales, used for school placement in France. Lewis Terman adapted the test to measure general intelligence. Scores were reported as “mental age” divided by chronological age, multiplied by 100. The current version of the IQ test is standardized, and two standard deviations below the test taker’s group calculate as an IQ of 70. An IQ of 70 or below suggests an intellectual disability diagnosis. Based on the IQ score, the severity grading appears below.
- IQ 50 to 70: mild intellectual disability (85% of cases)
- IQ 35 to 50: moderate intellectual disability (10% of cases)
- IQ 20 to 35: severe intellectual disability (4% of cases)
- IQ below 20: Profound intellectual disability (1% of cases)
However, it is no longer a standard to classify intellectual disability by IQ score alone. For instance, if an individual has IQ below 70 but has a good adaptive function, the subject does not have an intellectual disability. On the other side, individuals with a normal or even higher than normal IQ may manifest severe deficits in adaptive functions and are, therefore, classified as having an intellectual disability. In turn, the current diagnosis of intellectual disability also considers a person’s adaptive function.[18] The Adaptive Behaviour Assessment System can measure adaptive function.[19] It encompasses the social and practical domains. Adaptive function measures ability in communication, social participation, and independent living.
The DSM-5 also has “Unspecified Intellectual Disability” (Intellectual Developmental Disorder) to describe individuals over the age of 5 suspected of having an intellectual disability who has difficulty completing required tests, usually because of limitations resulting from blindness, deafness, or concurrent mental illness.
Chromosomal analysis, urine and blood tests, and neuroimaging techniques have been used to elucidate the etiology of intellectual disability.
Traditionally, chromosomal analysis has been done by parents’ choice before the birth of a child via amniocentesis (performed at 15 weeks of gestation) or chorionic villi sampling (8 to 10 weeks of gestation). It is a highly specific test for Down syndrome, and early detection of chromosomal abnormalities allows a decision to terminate the pregnancy. Recently, a cell-free fetal DNA test has appeared as a noninvasive prenatal test for Down syndrome. It has demonstrated a higher detection rate, positive predictive value, and false-positive rate.[20] Another current technique of chromosomal analysis is fluorescent in situ hybridization (FISH), which is useful to identify the microscopic deletion of the chromosome.[21]
Urine and blood analysis allow the evaluation of enzyme activities and detection of inborn errors of metabolism, including PKU, Lesch-Nyhan syndrome, galactosemia, and Hurler syndrome, with the help of advanced techniques such as tandem mass spectroscopy and gas chromatography.[22]
As for neuroimaging techniques, computerized tomography (CT) or magnetic resonance imaging (MRI) has been useful to identify microcephaly, cerebral developmental delay, and cerebral palsy.[23] Functional MRI and diffusion tensor imaging are being researched to identify abnormalities in neural circuit pathways. For example, Fragile X syndrome with aberrant frontal-striatal pathways has been found associated with ADHD symptoms. Electroencephalography (EEG) is used to detect seizures that often accompany intellectual disability, though findings do not direct to specific diagnoses.[24]
Treatment / Management
Management of intellectual disability must begin promptly with the goals to prevent further worsening, minimize the symptoms of disability, and improving the quality of everyday life. When initiating therapy, a healthcare provider must be aware of the various avenues of treating intellectual disability to orchestrate a multidisciplinary and individually tailored treatment appropriately. This section will discuss some examples of the multiple interventions available.
Educational support is a crucial component of intellectual disability management. Upon diagnosis of intellectual disability in children, healthcare providers must contact the school promptly to set up special education arrangements. What special education entails may vary slightly among schools, but it typically aids comprehensively with providing academic modifications as well as transition planning from childhood to adulthood with a focus on promoting self-sufficiency. It also teaches them how to seek assistance, behavioral skills, vocational skills, communication skills, functional living skills, and social skills based on individual needs in the least restrictive environment. Creating the least restrictive environment for students with an intellectual disability means placing them in general classrooms as much as tolerated. While segregated classrooms for special needs may be helpful for those who need them, implementing the least restrictive environment policy has been shown to improve student outcomes. It is important to monitor the patients’ progress in school because education solely from classroom settings may not be sufficient. If an individual with an intellectual disability requires assistance beyond what is available at school, the family can meet the need at home through family education or other outside resources. For example, a disabled student who needs extra attention with social skills may be referred to participate in the Special Olympics programs that have been shown to improve social competence in intellectual disability subjects. Lastly, other causes of learning difficulties need to be ruled out, and appropriate hearing and vision screenings are necessary for individuals with intellectual disabilities.
Behavioral intervention is another important aspect of intellectual disability management, and it can occur in a few different ways. Behavioral therapy aims to encourage positive behaviors while discouraging undesirable behaviors. Providing positive reinforcement and benign punishments (e.g., time-outs) is an effective method of behavioral training. Other supplemental methods may include avoiding triggers of negative demeanor, shunning misconduct, and redirecting to prevent or curtail any troublesome behavior. Cognitive therapy is another mode of behavioral training that has been effective for eligible intellectual disability patients. Cognitive therapy has its basis on the principle that one’s behavior, emotions, and cognitions are connected, and it aims to correct one’s negative behaviors by identifying and adjusting negative thoughts and emotional stress. Although many other approaches to behavioral intervention exist, the implementation of behavioral therapy, cognitive therapy, or a combination of the two is the most widely used method that has been shown to be an effective means of behavioral intervention for intellectual disability patients.
Vocational training helps teenagers and young adults to obtain the necessary skills to enter the labor market. In vocational training, patients carry out pre-scheduled activities under the supervision of a multi-disciplinary team consisting of a social worker, occupational therapist, teacher, counselor, and psychologist. Patients learn to keep themselves clean, wear appropriate clothes, and carry out their responsibilities. A study has shown that patients who underwent vocational training had reduced support requirements compared to their peers.
Family education is an essential service provided by healthcare providers for family members of intellectually disabled patients. The first part of this is assisting the family members in understanding intellectual disability: definition, management, and prognosis. Then, healthcare providers can help the family through placement decisions, refer them to appropriate services and equipment, and provide caregiver training. In addition to preparing the family for the patient, physicians must recognize that family members also often bear a significant amount of stress as well. The medical team must support the whole family through psychosocial problems such as the need for respect, feeling helpless, depression, and anxiety. There are also outside resources to which the family can obtain a referral. American Association on Intellectual and Developmental Disabilities (AAIDD), The Arc of the United States, and Family-to-family Health Information and Education Centers are some of the nationally available resources, and social workers can help with connecting the families with local resources. Establishing strong support for the family, in turn, creates a caring home environment for the patient.
Government resources are available for patients with intellectual disabilities and their families. Patients with intellectual disabilities are eligible to benefit from social security income. Patients also may benefit from various community services that provide housing and food delivery. The government also provides education and employment opportunities as outlined under the "Disability Resources" section of the US Department of Labor website.
Psychopharmacologic interventions may not be the main component of intellectual disability treatment, but they play a significant role in treating behavioral abnormalities associated with intellectual disorders and comorbid conditions. Aggressive behavior is not uncommon among individuals with intellectual disabilities and causes admission to institutional settings. Risperidone is well-documented to treat disruptive, aggressive, and self-injurious behaviors in children with intellectual disabilities with good safety and tolerability profile.[25] Risperidone is an atypical antipsychotic that is less likely to cause tardive dyskinesia, which commonly results in a typical antipsychotic. Aripiprazole is another atypical antipsychotic that is used to manage aggression.
Treatment of comorbid conditions is an important aspect of adequate therapy. Attention-deficit/hyperactivity disorder (ADHD), depression, and movement disorders are some of the comorbid conditions accompanying intellectual disability that require evaluation and treatment. Methylphenidate, clonidine, and atomoxetine are shown in randomized control trials to reduce ADHD symptoms. Methylphenidate significantly improved the maintenance of attention to complete a task; however, there was no long-term improvement in learning and social skills.
Depressive symptoms can be easily overlooked in individuals with intellectual disabilities when other behavioral problems are prominent; this requires careful evaluation. Selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, paroxetine, and sertraline were shown in multiple studies to help with depressive symptoms in this patient population.
Involuntary movements, repetitive self-stimulatory behaviors, and obsessive-compulsive symptoms may be harmful to the patients. Antipsychotic medications have been anecdotally reported to diminish these symptoms, although there was no observation of improvement in adaptive behavior.[26] SSRIs are useful in treating obsessive-compulsive symptoms and stereotyped motor movements.[27]
Studies have shown that patients with intellectual disabilities are at risk for polypharmacy, and providers should be cautious when prescribing medications as some patients may be at a higher risk of side effects and may need lower dosages.
Differential Diagnosis
Several diseases or conditions can be mistaken for intellectual disability:
- Child abuse: childhood abuse may cause developmental delays in language and socialization, causing a defect in adaptive function. The child may have difficulty communicating her needs and developing trust and social responsibility. Unlike intellectual disability, symptoms are often reversible when the environment improves.
- Debilitating medical disease: Individuals with normal intelligence may experience depression and delay in the development of chronic, debilitating medical illnesses.
- Cerebral palsy: poor muscle coordination, problems with vision, hearing, and speaking may imitate symptoms of intellectual disability.
- Sensory disability: deafness or blindness may lead to a flaw in diagnostic testing, causing a false-positive diagnosis of intellectual disability.
- Speech disorder: expressive and receptive aphasia may be mistaken for intellectual disability.
Prognosis
The cognitive deficit of intellectual disability is permanent damage; thus, the prognosis of intellectual disability depends on the severity of cognitive impairment and the supportive environment provided. If provided adequate support, individuals with mild intellectual disabilities may achieve adequate language and social competency to live independently and raise their own families. Individuals with moderate intellectual disabilities are not likely to achieve academic levels greater than second grade; however, they may acquire language and communicate their needs. They may be able to get a job under supervision. Individuals with severe intellectual disabilities usually have difficulty acquiring language. They may be able to develop alternative communication skills and recognize words that are critical to functioning. Adults with a severe intellectual disability usually require supervised living situations, such as group homes, and supervision to perform any work-related tasks. Individuals with profound intellectual disabilities have significant difficulty with communication and social functioning.
Complications
Most individuals with intellectual disabilities have comorbid psychiatric conditions. Individuals are at higher risk of developing depression because they are prone to developing negative self-images as they have difficulty interacting with others and meeting social expectations. Other psychiatric comorbid symptoms frequently observed in these individuals are hyperactivity, self-injurious behaviors, and repetitive stereotypical behaviors. Management of complications is discussed above in the “Treatment” section.
Deterrence and Patient Education
Among the most challenging aspects of intellectual disability is the patient’s sense of social skill deficit and social isolation. Educating the family for support to improve social competence and self-esteem is critical. Special Olympics International program is an example program that helps with improving social interactions, friendships, and self-esteem.[28] Individuals with a disability need to be continuously encouraged to learn and interact with other people. The family of individuals with intellectual disabilities should understand that they are more prone to experience failures and rejections and make sure to provide a supportive environment that is not discouraging. Family therapy can help with resolving any feeling of guilt, despair, or anger that may occur in the family relationship.
Enhancing Healthcare Team Outcomes
The management of patients with intellectual disabilities is best with an interprofessional team. When treating individuals with intellectual disabilities, a healthcare provider may find communication with the patients difficult and may coerce the treatments. It is important to act professionally and make sure that patients do not get excluded from fundamental rights and are not coerced into specific therapies, as emphasized in the United Nations Convention for Intellectual Disability.[29] Healthcare providers must carefully listen to the patient's needs and provide treatments that are in the patient's best interest. To serve the patient's best interest, an interprofessional, an interprofessional approach is essential; it has been shown to reduce the healthcare cost by decreasing the number of tests for the diagnosis of intellectual disability and the frequency of hospitalization.[30] Core members of the interprofessional team are primary care physicians, psychiatrists, psychologists, neurologists, speech pathologists, special nurse educators, social workers, and pharmacists. To maintain the best collaborative care, communication among the members of the team be effective. Each healthcare provider must promptly and accurately document diagnosis, assessment, services provided, and follow-up plans. In the current healthcare system, it is efficient and effective for primary care physicians and nurse practitioners to refer to specialists based on the patient’s needs, collect evaluations and reports, and coordinate care.
The array of treating physicians will manage the overall case, but they must rely on the input of other team members. Specialty-trained mental health nurses can provide a great deal of valuable information as they engage with the patient. They are also excellent resources for verifying medication and other therapeutic intervention compliance, which can be challenging in such cases, as well as evaluating the effectiveness of the current regimen. Pharmacists must weigh in with medication reconciliation, assist in agent selection for comorbidities, and verify dosing. Pharmacists can also educate patients and/or their families regarding the medications used. Medication adverse events should be reported to the treating physician promptly by either the pharmacist or nursing staff. Thus, an interprofessional approach is the optimal means by which to address patients with intellectual disabilities. [Level 5]