Continuing Education Activity
Viral meningitis is the inflammation of the meninges caused by a virus. It is most common in young children but is seen across all age groups. This activity reviews the evaluation and management of viral meningitis and explains the role of the interprofessional team in evaluating and treating patients with viral meningitis.
Objectives:
- Identify the common etiologies of viral meningitis.
- Review the typical presentation of patients with viral meningitis.
- Outline the treatment and management options available for viral meningitis.
- Describe interprofessional team strategies for improving care coordination and communication to advance the management of viral meningitis and improve outcomes.
Introduction
Meningitis is the inflammation of the meninges with an associated abnormal cell count in the cerebrospinal fluid (CSF).[1] Aseptic meningitis, defined by the lack of bacterial growth in cultures, is the most common form, with viruses being a frequent cause.[2] Viral causes of meningitis have become more common as the prevalence of bacterial meningitis has decreased due to vaccinations, and viral meningitis is the most common form of meningitis in many countries.[3] Viral meningitis typically presents with the acute onset of fever, headache, photophobia, neck stiffness, and often nausea and vomiting, although younger children may not show signs of meningeal irritation.[1][4] Appropriate and timely evaluation is critical as there are no reliable initial clinical indicators to differentiate bacterial and viral etiologies of meningitis. Viral meningitis is usually a self-limiting illness with a good prognosis.[1]
Etiology
Enteroviruses (Coxsackie or Echovirus groups) are the most common cause of viral meningitis across all age groups; parechoviruses are also common in children.[5][6] Herpesviruses that cause meningitis include herpes simplex virus (HSV) 1 and 2, varicella-zoster virus (VZV), cytomegalovirus, Epstein-Barr virus, and human herpesvirus 6. Other viral causes include adenovirus, lymphocytic choriomeningitis virus (LCMV), influenza, parainfluenza, and mumps.[3][6] Arboviruses that can cause viral meningitis include West Nile virus (WNV), Zika, chikungunya, dengue, LaCross, Saint Louise encephalitis, Powassan, and eastern equine encephalitis virus.[4]
Epidemiology
Viral meningitis most commonly occurs in young children, with the incidence decreasing with age.[1] In countries with high rates of immunization coverage, viral meningitis is more common than bacterial meningitis, with an estimated 3 to 18% of childhood meningitis being bacterial in origin. Vaccinations for Haemophilus influenza type B, Streptococcus pneumoniae, and Neisseria meningitidis have significantly decreased cases of bacterial meningitis.[6] The incidence of viral meningitis has been estimated to range from 0.26 to 17 cases per 100000 people. In the United States, there are up to 75000 cases of enteroviral meningitis annually.[3] In temperate climates, viral meningitis is most common in the summer and autumn months, while it is present year-round in tropical and subtropical areas.[4]
Enteroviruses rank as the most common cause of viral meningitis in many places in the world, with up to 12 to 19 cases per 100000 population annually in some high-income countries.[7] WNV, which is spread by mosquitoes, can cause meningitis and encephalitis. It is now endemic in North America and carries a 4 to 13% fatality rate. Mortality is higher in patients who are elderly, immunosuppressed, or have diabetes.
Half of the patients with WNV encephalitis have long-term neurological or psychological sequelae.[8]
Human immunodeficiency virus (HIV) meningitis can be present during seroconversion, occurring in 10 to 17% of symptomatic seroconversion illnesses, with a small number progressing to chronic meningitis.[1][8]
VZV can cause viral meningitis, more commonly with reactivation than in primary infection. Varicella meningitis can occur without cutaneous lesions.[1]
HSV 1 and 2 can cause viral meningitis. HSV-1 is more commonly associated with sporadic encephalitis, while HSV-2 can cause a benign recurrent viral meningitis; meningitis usually occurs in the absence of genital lesions or a history of prior genital herpes infection.[4] HSV reaches the central nervous system via the cranial nerves.[8] LCMV is a rodent-borne virus, usually spread via inhalation of aerosolized urine or droppings, through vertical transmission and transmission via infected corneal, liver, and kidney transplants is also possible. It is more common in winter and early spring.[4] Mumps was previously a common cause of viral meningitis in the United States but has decreased recently due to the widespread use of measles, mumps, and rubella (MMR) vaccination. It is more common in male patients.[1][9]
Pathophysiology
Meningitis is an inflammatory pathology of the meninges surrounding the brain.[3] Viruses can reach the meninges in a variety of ways, including spread via the bloodstream, retrograde spread from nerve endings, and reactivation from a dormant state within the nervous system.[3][4] As a virus reaches the central nervous system (CNS) and spreads through the subarachnoid space, it causes an inflammatory response resulting in meningitis.[8] Encephalitis occurs when there is inflammation of the brain parenchyma and is associated with a worse prognosis.[1][3] The mumps virus is highly neurotropic and can directly infect the epithelium of the choroid plexus.[4] Enteroviruses replicate outside the CNS and reach the CNS via hematogenous spread.[8]
History and Physical
The clinical findings of viral meningitis can vary by age and immune status.[9] Viral meningitis typically presents with acute onset of fever, headache, photophobia, neck stiffness, and nausea/vomiting. Young children may present with fever and irritability without evidence of meningeal irritation. In the initial presentation, there are no reliable clinical indicators to differentiate viral versus bacterial meningitis.[1] Neonates with enteroviral meningitis can present similarly to bacterial sepsis and may also have systemic involvement such as hepatic necrosis, myocarditis, necrotizing enterocolitis, seizures, or focal neurologic findings.[9]
Older infants and children may have a biphasic fever, first peaking with systemic constitutional symptoms and a second febrile phase with the onset of neurological signs.[9][7] Viral meningitis in adults is more likely to present with meningeal symptoms and a higher CSF protein. Children with viral meningitis are more likely to have a fever, respiratory symptoms, and leukocytosis.[10] Consider WNV meningitis in adults presenting with CSF pleocytosis and lower motor neuron involvement; WNV is more common in adults than children.[9][10]
It is important to obtain a travel history in patients with suspected viral meningitis, as many viruses have specific geographical distributions.[8]
Evaluation
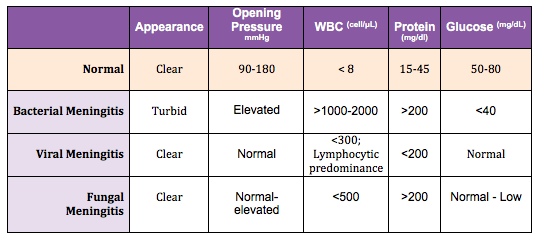
A lumbar puncture is necessary unless there are contraindications such as focal neurologic deficits, papilledema, recent seizures, age 60 or greater.[1][11] Indications for imaging before performing a lumbar puncture include focal neurological signs, papilledema, continuous or uncontrolled seizures, or a Glasgow Coma Score less than 12.[12] Cerebrospinal fluid (CSF) analysis, including cell count and differential, glucose, protein, culture, and molecular diagnostics as available, should be performed. Viral meningitis characteristically has a CSF mononuclear pleocytosis, although there may initially be a neutrophilic predominance.[1] This neutrophilic predominance is not limited to the first 24 hours of illness and is not a reliable indicator between viral and bacterial meningitis.[1][13] Polymerase chain reaction (PCR) tests can be used to diagnose some causes of viral meningitis, such as enterovirus, VZV, and HSV. Serum white blood cell count and C-reactive protein do not reliably distinguish viral and bacterial meningitis.[1] CSF C-reactive protein and procalcitonin have not been shown to differentiate viral vs. bacterial meningitis compared to serum levels.[14]
Because of the lack of clinical findings to help distinguish between viral and bacterial meningitis and the risk of untreated bacterial meningitis, there has been much interest in identifying predictors of bacterial meningitis. The bacterial meningitis score (BMS) was originally developed for and validated in children with meningitis. The score is comprised of four laboratory predictors (positive Gram stain, CSF protein over 80 mg/dL, peripheral absolute neutrophil count greater than 10000 cells/mm3, CSF absolute neutrophil count over 1000 cells/mm3) and one clinical predictor (seizure at or before the presentation). A positive Gram stain is worth 2 points, and the other predictors are worth 1 point each if present. The negative predictive value for a score of 0 was 100%; a score of more than 2 predicted bacterial meningitis with 87% sensitivity.[15] The BMS has also undergone validation in adults with meningitis.[16]
In adults, researchers have studied individual predictors of bacterial rather than viral meningitis. In one study, these predictors included CSF glucose less than 34 mg/dL, CSF WBC over 2000 cells/mm3, CSF neutrophils greater than 1180, CSF protein over 220 mg/dL, and a ratio of CSF to blood glucose less than 0.23.15.[17] CSF lactate has been shown to be a good indicator to differentiate bacterial from aseptic meningitis.[18][19] The combination of CSF results, such as enterovirus and lactate, with the BMS, can increase sensitivity and specificity.[20][21]
Treatment / Management
Most viruses causing meningitis have no specific treatment other than supportive care.[3][4][9] Fluid and electrolyte management and pain control are the mainstays of management of viral meningitis. Patients should undergo observation for neurological and neuroendocrine complications, including seizures, cerebral edema, and SIADH.
Because of the difficulty in differentiating viral from bacterial meningitis initially, empiric antibiotic therapy is usually indicated until bacterial meningitis is ruled out.[9] In patients aged one month and older, empiric therapy for bacterial meningitis can be provided with vancomycin in combination with either ceftriaxone or cefotaxime while culture results are pending.[17] If encephalitis is suspected, empiric antiviral treatment with intravenous acyclovir should be a consideration.[1] Acyclovir should be the choice for suspected or proven HSV or VZV infections, although it has been shown to provide benefits in HSV encephalitis, not meningitis.[4][8][12]
Differential Diagnosis
Partially-treated bacterial meningitis should merit consideration scenario if the patient received prior antibiotic exposure.[9] Other infectious etiologies to consider include mycoplasma, spirochetes, mycobacteria, Brucella, and fungal meningitis or encephalitis.[1][9] Noninfectious etiologies include drugs (NSAIDs, trimethoprim-sulfamethoxazole, intravenous immune globulin), heavy metals, neoplasms, neurosarcoidosis, systemic lupus erythematosus, Behcet's syndrome, and vasculitis.[4][9] In children, Kawasaki disease can present similarly to bacterial or viral meningitis.[22]
Prognosis
The prognosis of viral meningitis without associated encephalitis is generally good.[23] Viral meningitis typically has a spontaneous recovery, compared to bacterial meningitis in which progressive mental status deterioration may occur. Older infants and children are often ill for greater than a week but usually, have a full recovery. Adults with enterovirus meningitis can have symptoms for several weeks, but the illness is typically less severe than in children.[9] While viral meningitis is usually self-limiting, there can be morbidity.[1]
Complications
Enterovirus meningitis typically has a benign course, while enterovirus encephalitis can result in long-term neurological sequelae. Significant morbidity and mortality follow enteroviral meningitis in neonates and immunocompromised patients. Some subtypes of enterovirus, such as EV71 and EV68, are associated with more severe neurological disease and worse outcomes. The most common severe complications of enteroviral meningitis are meningoencephalitis, myocarditis, and pericarditis.[7][23] In children, neurologic complications of enteroviral infection can include acute flaccid paralysis and rhombencephalitis.[24][7] Neuropsychological impairments after viral meningitis are measurable but typically not as severe as those sustained after bacterial meningitis.[25] Some studies have noted impaired sleep as a long-term sequela of meningitis.[26]
Deterrence and Patient Education
The spread of pathogens causing viral meningitis is commonly through the fecal-oral route, so good hand hygiene is essential in prevention. Some causes of meningitis are preventable by vaccination.[4]
Pearls and Other Issues
Infants and young children may present with fever, irritability, and non-specific symptoms such as lethargy and decreased oral intake, with a lack of meningeal signs.[1][23]
Utilization of PCR tests to diagnosis viruses such as enterovirus, HSV, and VZV can decrease the length of stay and reduce antibiotic administration.[1]
There are no reliable clinical indicators to distinguish bacterial from viral meningitis, though certain laboratory and clinical predictors can help identify patients at low risk for bacterial meningitis.[15][21]
Enhancing Healthcare Team Outcomes
Viral meningitis can occur at age any but is most common in younger age groups. Because of the lack of apparent distinguishing features between viral and bacterial meningitis on initial presentation, an interprofessional team with strong medical knowledge and open communication is essential in providing appropriate care to these patients. Pharmacists can recommend empiric antibiotic coverage until there is confirmation of a diagnosis of viral meningitis. Nurses who look after patients with viral meningitis should know the disorder, what potential complications can arise, and when to call the clinician. The treatment of viral meningitis, for the most part, is supportive but residual sequelae of the disease are not uncommon; hence follow up with the primary care provider, and nurse practitioner is necessary. Interprofessional collaboration is crucial for optimal results in the management of viral meningitis, as with any condition. [Level 5]