[1]
Dalmau J, Gleichman AJ, Hughes EG, Rossi JE, Peng X, Lai M, Dessain SK, Rosenfeld MR, Balice-Gordon R, Lynch DR. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. The Lancet. Neurology. 2008 Dec:7(12):1091-8. doi: 10.1016/S1474-4422(08)70224-2. Epub 2008 Oct 11
[PubMed PMID: 18851928]
Level 2 (mid-level) evidence
[2]
Hughes EG, Peng X, Gleichman AJ, Lai M, Zhou L, Tsou R, Parsons TD, Lynch DR, Dalmau J, Balice-Gordon RJ. Cellular and synaptic mechanisms of anti-NMDA receptor encephalitis. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2010 Apr 28:30(17):5866-75. doi: 10.1523/JNEUROSCI.0167-10.2010. Epub
[PubMed PMID: 20427647]
[3]
Armangue T, Spatola M, Vlagea A, Mattozzi S, Cárceles-Cordon M, Martinez-Heras E, Llufriu S, Muchart J, Erro ME, Abraira L, Moris G, Monros-Giménez L, Corral-Corral Í, Montejo C, Toledo M, Bataller L, Secondi G, Ariño H, Martínez-Hernández E, Juan M, Marcos MA, Alsina L, Saiz A, Rosenfeld MR, Graus F, Dalmau J, Spanish Herpes Simplex Encephalitis Study Group. Frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: a prospective observational study and retrospective analysis. The Lancet. Neurology. 2018 Sep:17(9):760-772. doi: 10.1016/S1474-4422(18)30244-8. Epub 2018 Jul 23
[PubMed PMID: 30049614]
Level 2 (mid-level) evidence
[4]
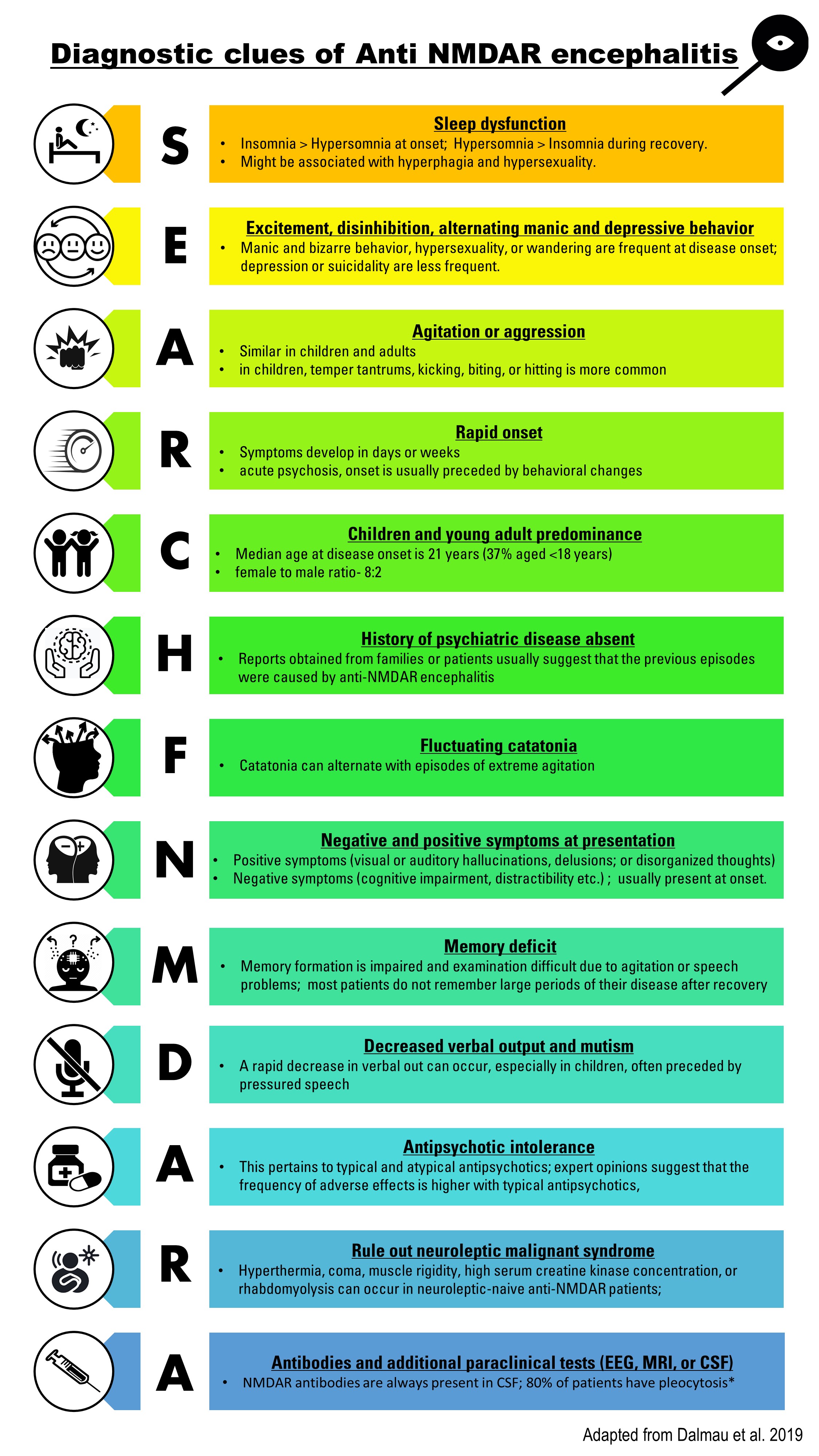
Dalmau J, Armangué T, Planagumà J, Radosevic M, Mannara F, Leypoldt F, Geis C, Lancaster E, Titulaer MJ, Rosenfeld MR, Graus F. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. The Lancet. Neurology. 2019 Nov:18(11):1045-1057. doi: 10.1016/S1474-4422(19)30244-3. Epub 2019 Jul 17
[PubMed PMID: 31326280]
[5]
Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA. The frequency of autoimmune N-methyl-D-aspartate receptor encephalitis surpasses that of individual viral etiologies in young individuals enrolled in the California Encephalitis Project. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 Apr:54(7):899-904. doi: 10.1093/cid/cir1038. Epub 2012 Jan 26
[PubMed PMID: 22281844]
[6]
van Coevorden-Hameete MH, Titulaer MJ, Schreurs MW, de Graaff E, Sillevis Smitt PA, Hoogenraad CC. Detection and Characterization of Autoantibodies to Neuronal Cell-Surface Antigens in the Central Nervous System. Frontiers in molecular neuroscience. 2016:9():37. doi: 10.3389/fnmol.2016.00037. Epub 2016 May 31
[PubMed PMID: 27303263]
[7]
Iizuka T, Sakai F, Ide T, Monzen T, Yoshii S, Iigaya M, Suzuki K, Lynch DR, Suzuki N, Hata T, Dalmau J. Anti-NMDA receptor encephalitis in Japan: long-term outcome without tumor removal. Neurology. 2008 Feb 12:70(7):504-11
[PubMed PMID: 17898324]
[8]
Titulaer MJ, Höftberger R, Iizuka T, Leypoldt F, McCracken L, Cellucci T, Benson LA, Shu H, Irioka T, Hirano M, Singh G, Cobo Calvo A, Kaida K, Morales PS, Wirtz PW, Yamamoto T, Reindl M, Rosenfeld MR, Graus F, Saiz A, Dalmau J. Overlapping demyelinating syndromes and anti–N-methyl-D-aspartate receptor encephalitis. Annals of neurology. 2014 Mar:75(3):411-28
[PubMed PMID: 24700511]
[9]
Iizuka T, Kaneko J, Tominaga N, Someko H, Nakamura M, Ishima D, Kitamura E, Masuda R, Oguni E, Yanagisawa T, Kanazawa N, Dalmau J, Nishiyama K. Association of Progressive Cerebellar Atrophy With Long-term Outcome in Patients With Anti-N-Methyl-d-Aspartate Receptor Encephalitis. JAMA neurology. 2016 Jun 1:73(6):706-13. doi: 10.1001/jamaneurol.2016.0232. Epub
[PubMed PMID: 27111481]
[10]
Lagarde S, Lepine A, Caietta E, Pelletier F, Boucraut J, Chabrol B, Milh M, Guedj E. Cerebral (18)FluoroDeoxy-Glucose Positron Emission Tomography in paediatric anti N-methyl-D-aspartate receptor encephalitis: A case series. Brain & development. 2016 May:38(5):461-70. doi: 10.1016/j.braindev.2015.10.013. Epub 2015 Nov 2
[PubMed PMID: 26542469]
Level 2 (mid-level) evidence
[11]
Staley EM, Jamy R, Phan AQ, Figge DA, Pham HP. N-Methyl-d-aspartate Receptor Antibody Encephalitis: A Concise Review of the Disorder, Diagnosis, and Management. ACS chemical neuroscience. 2019 Jan 16:10(1):132-142. doi: 10.1021/acschemneuro.8b00304. Epub 2018 Aug 31
[PubMed PMID: 30134661]
[12]
Breese EH, Dalmau J, Lennon VA, Apiwattanakul M, Sokol DK. Anti-N-methyl-D-aspartate receptor encephalitis: early treatment is beneficial. Pediatric neurology. 2010 Mar:42(3):213-4. doi: 10.1016/j.pediatrneurol.2009.10.003. Epub
[PubMed PMID: 20159432]
[13]
Titulaer MJ, McCracken L, Gabilondo I, Armangué T, Glaser C, Iizuka T, Honig LS, Benseler SM, Kawachi I, Martinez-Hernandez E, Aguilar E, Gresa-Arribas N, Ryan-Florance N, Torrents A, Saiz A, Rosenfeld MR, Balice-Gordon R, Graus F, Dalmau J. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. The Lancet. Neurology. 2013 Feb:12(2):157-65. doi: 10.1016/S1474-4422(12)70310-1. Epub 2013 Jan 3
[PubMed PMID: 23290630]
[14]
Zhang L, Wu MQ, Hao ZL, Chiang SM, Shuang K, Lin MT, Chi XS, Fang JJ, Zhou D, Li JM. Clinical characteristics, treatments, and outcomes of patients with anti-N-methyl-d-aspartate receptor encephalitis: A systematic review of reported cases. Epilepsy & behavior : E&B. 2017 Mar:68():57-65. doi: 10.1016/j.yebeh.2016.12.019. Epub 2017 Jan 19
[PubMed PMID: 28109991]
Level 3 (low-level) evidence
[15]
de Bruijn MAAM, van Sonderen A, van Coevorden-Hameete MH, Bastiaansen AEM, Schreurs MWJ, Rouhl RPW, van Donselaar CA, Majoie MHJM, Neuteboom RF, Sillevis Smitt PAE, Thijs RD, Titulaer MJ. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABA(B)R encephalitis. Neurology. 2019 May 7:92(19):e2185-e2196. doi: 10.1212/WNL.0000000000007475. Epub 2019 Apr 12
[PubMed PMID: 30979857]
[16]
Wang HY, Li T, Li XL, Zhang XX, Yan ZR, Xu Y. Anti-N-methyl-D-aspartate receptor encephalitis mimics neuroleptic malignant syndrome: case report and literature review. Neuropsychiatric disease and treatment. 2019:15():773-778. doi: 10.2147/NDT.S195706. Epub 2019 Apr 2
[PubMed PMID: 31040676]
Level 3 (low-level) evidence
[17]
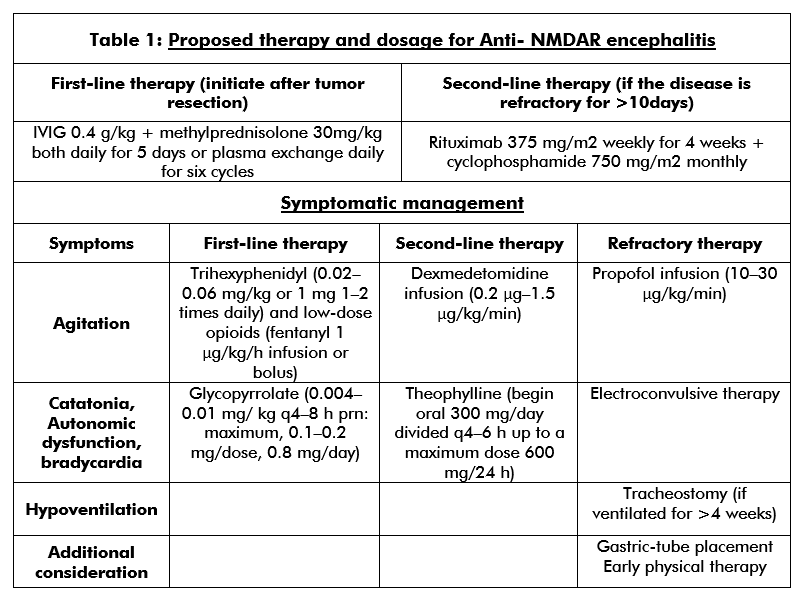
Neyens RR, Gaskill GE, Chalela JA. Critical Care Management of Anti-N-Methyl-D-Aspartate Receptor Encephalitis. Critical care medicine. 2018 Sep:46(9):1514-1521. doi: 10.1097/CCM.0000000000003268. Epub
[PubMed PMID: 29927776]
[18]
Balu R, McCracken L, Lancaster E, Graus F, Dalmau J, Titulaer MJ. A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis. Neurology. 2019 Jan 15:92(3):e244-e252. doi: 10.1212/WNL.0000000000006783. Epub 2018 Dec 21
[PubMed PMID: 30578370]