Continuing Education Activity
Colostomy care, as the name suggests, is an all-encompassing term referring to colostomy management, from its creation to peristomal skin management, to colostomy appliance application and mental health management while dealing with a colostomy. The purpose of colostomy care is for skin protection and care for patient acceptance and to prevent stoma related complications. This activity outlines colostomy creation and care and highlights the role of the interprofessional team in evaluating and treating patients with this condition.
Objectives:
- Identify the indications for colostomy and the different types of colostomies.
- Explain the importance of colostomy care and the steps in colostomy care.
- Summarize the risks associated with a colostomy.
- Explain the importance of improving care coordination among the interprofessional team to enhance the delivery of care for patients with a colostomy.
Introduction
A stoma is the exteriorization of a loop of bowel from the anterior abdominal wall, done during a surgical procedure. It is done for diversion or decompression of the remaining bowel.
A colostomy is a type of stoma in which the colon (ascending/transverse/descending/sigmoid) is exteriorized. This may be done to treat disease or to relieve an obstruction or to prevent the remaining bowel from contamination by fecal matter.
It may be temporary or permanent, depending on the indication for which it was performed. Most stomas are incontinent, which means that there is no voluntary control over the passage of flatus and feces from the stoma.
This makes colostomy care a mandatory procedure after colostomy creation. Colostomy care, as the name suggests, is an all-encompassing term referring to colostomy management, from its creation to peristomal skin management, to colostomy appliance application and mental health management while dealing with a colostomy.
The purpose of colostomy care is for skin protection and care for patient acceptance and to prevent stoma related complications.[1][2]
Anatomy and Physiology
The large bowel starts at the cecum, moves up to the ascending colon with the hepatic flexure, the transverse colon with the splenic flexure, the descending colon, and the sigmoid colon. As the content moves through the colon, it gets firmer in consistency as a result of water and electrolyte absorption in the large bowel.
The most common type of colostomy is the sigmoid colostomy followed by the transverse colostomy, while ascending and descending colostomies are rare and hardly performed.
There are different types of colostomies, including loop colostomy, double-barrel colostomy, and end colostomy. The different types of colostomies are created depending on the indication, length of the mesocolon, and amount of diseased and remaining normal bowel.
The content of effluent in the different types of colostomies varies from soft and loose, foul-smelling, oatmeal-like stool in the ascending and transverse colostomies to firmer, paste-like stool from the transverse and descending colostomies, to output resembling normal stool from a sigmoid colostomy. As the stool gets firmer along the colon, the output becomes easier to manage.
Colostomies are generally made in the anterior abdominal wall over the rectus abdominis muscle to either side of the linea alba, generally inferior to the umbilicus. Occasionally the site is cephalad to the umbilicus, particularly in obese patients, as the anterior abdominal wall has less subcutaneous fat in the upper part. During the procedure, a circular incision is created over the pre-identified stoma site. It needs a flat surface on the abdomen of at least 2 to 3 inches and should be away from the beltline, any scars, as well as bony prominences to ensure a secure seal of the stoma appliance. The incision is deepened onto the anterior rectus sheath, which is incised in a cruciate fashion.
The rectus muscle is retracted sideways, without cutting into the muscle itself, and the posterior rectus sheath is again incised in a cruciate manner. The loop of bowel that is identified for the stoma creation is pulled through the incision and exteriorized onto the skin. The identification of the bowel is aided by performing a diagnostic laparoscopy to ensure good mobility and reach the anterior abdominal wall without tension. However, the stoma can also be created in a trephine manner without a laparoscopic approach. It is important to consult cross-sectional imaging to pre-identify the most mobile segment of the bowel and mark the colostomy site in accordance. A transverse colostomy should be fashioned in the left upper quadrant, a sigmoid colostomy in the left iliac fossa.
Once it is exteriorized, a stoma rod can be eased through the mesocolon to reduce the risk of retraction into the abdominal cavity. The colon is incised three-quarters of the circumference and the bowel edges fixed to the skin with interrupted sutures using an absorbable suture material and raising the stoma above the skin level slightly. In contrast to an ileostomy, colostomies generally do not require eversion and 3-point fixation, owing to the content having less enzymatic action.[1]
Indications
The indications of a colostomy are divided on the basis of the type of colostomy:
A double-barrel colostomy is a type of colostomy done after bowel resections involving the mesentery and is done in conditions like colorectal cancers, after resection of gangrenous bowel segments, inflammatory bowel disease, penetrating bowel injuries or after resection of gangrenous sigmoid volvulus.
A loop colostomy may be done in case of penetrating abdominal injury, colorectal cancer, intraoperative bowel injury, perineal injury, a diverticular disease with obstruction, blunt abdominal injury, protection of a distal anastomosis, anal incontinence or perineal injury, Fournier gangrene involving the perianal region and perianal fistulas. They may also be done in case of anorectal malformations or Hirschsprung disease in the neonatal population as a temporary emergency measure before correction surgery can be performed.
An end colostomy, after Hartmann procedure, is the most common type of colostomy worldwide. It is done in case of gangrenous sigmoid volvulus, colorectal cancer after abdominoperineal resection, ileo-sigmoid knotting, penetrating abdominal injury, ulcerative colitis, intussusception, anastomotic leak, anorectal cancer, and perineal injury. It involves the closure of the distal segment with fixation to the abdominal wall. Stomal closure, in this case, requires midline exploration and is hence least preferred in case colostomy is planned as a temporary measure, when there is an adequate distal segment, but this is a rare scenario.[1][2][3]
Contraindications
There are no contraindications to colostomy creation. They are often required when anastomosis cannot be achieved due to the emergency nature of the surgery or when the patient is not adequately nourished with inadequate serum albumin and protein levels. Likewise, when there is an inadequate length of bowel or mesentery after resection or the possibility of excessive tension at the anastomosis site.
Colostomy care must be done in all cases of colostomy. Some procedures like irrigation or enema should be avoided in case of stoma prolapse, chemotherapy, pelvic or abdominal radiation treatments, diarrhea-producing medication, or in case of an irregular functioning stoma and may lead to dependence.[4][5]
Equipment
Managing a colostomy is generally done by a nurse or an entero-stomal therapist, but providers should be aware of the condition of the stoma in case intervention may be required.
There are different types of colostomy bags or appliances available, depending on the type of stoma. The 2-piece system consists of a base-plate attached to the skin with a removable ostomy bag. Although it is very durable and long-lasting, it requires an amount of skill to use and has a weaker adhesive and does not fit very well. The one-piece system consists of a single unit wherein the skin barrier and the pouch are joined. It is simpler to use but must be replaced every 1 to 3 days. The closed pouch system is generally used by patients who have a constant elimination pattern and have to be discarded after a single-use.
The open-ended pouches are also commonly used and consist of a single piece attached to the skin around the stoma with a drainable pouch and can be left attached to the skin while removing stomal content. Generally in a colostomy, as compared to an ileostomy, a closed bag must be required, unless the content is excessively fluid, when a drainable bag may also be used. In an end colostomy, like after a Hartmann procedure, a colostomy plug can also be used.
Differently sized bags are available, and they may be used by different people or by the same person at different times during the day or during different activities. For example, a larger sized bag may be used while sleeping at night, whereas a smaller sized bag may be used during sexual activity or while exercising. Pediatric sized stoma bags are also available.
Stoma caps are like lids applied over the stoma. They may be worn by certain people like those with continent ileostomies or those who require stomal irrigation for movement at their discretion, for short intervals during the day.[6]
Personnel
Stoma care begins in the elective setting before the actual surgery and stomal creation. It begins when the patient is diagnosed and informed about the possibility of stoma creation. It requires mental health and guidance counselors to address any concerns the patient may have about their self-image and societal status. It also requires an entero-stomal therapist to discuss with the surgeon the location of the possible creation of the stoma and to go on and mark the colostomy site in the preoperative period.
In the immediate postoperative period, the colostomy may need dilatation and application of hyperosmotic agents like glycerine by the nursing staff so as to reduce stomal edema.
When the stoma becomes functional, generally between postoperative days 2 and 4, the colostomy will need a colostomy bag or appliance application. In the initial days, it is either done by the nursing staff or in larger hospitals, by an entero-stomal therapist. This is done with a view to teaching patients or in case of children, their guardians, how to do it themselves at home. They are informed about the various devices available, about the functioning of these devices, about their own colostomy and the kind of effluent that would be seen, about the complications of the stoma and the colostomy bags.
The most important person involved in colostomy care is the patient himself. Once the patient is discharged from the hospital, they are in charge of their own colostomy care. The patient must regularly change their colostomy bag as required and should visit the provider regularly to assess the stoma in the normal run, or in case of any complications. As a rule, the stoma bag should be emptied when it is filled up to 1/3rd to prevent peeling off of the baseplate from the skin and leaks.[7]
Preparation
Marking of the stoma preoperatively by an entero-stomal therapist helps to place the stoma in an appropriate location away from the beltline and away from folds of skin on the anterior abdominal wall to prevent repeated colostomy bag peel-off and leak.
A nasogastric tube may be placed in the pre or intraoperative period for bowel decompression, and a Foley catheter must also be placed to keep the bladder empty to prevent intraoperative injury and also to monitor urine output, especially during emergency procedures.
Mechanical bowel preparation may or may not be done, depending on the indication and the surgeon’s preference.
Antibiotics must be given just prior to the surgery.
For colostomy care preparation, a nurse or attendant is equipped with all the required equipment, including the appliance, the paste, and the scissors. A Macintosh sheet is placed under the patient, and gloves are worn.
Technique or Treatment
The colostomy appliance should be changed every 5-7 days, depending on the appliance. Patients generally do this themselves or with the help of the primary caregiver, or parent in case of children. Any case of skin breakdown or skin irritation or difference in stomal appearance should be seen by a health worker.
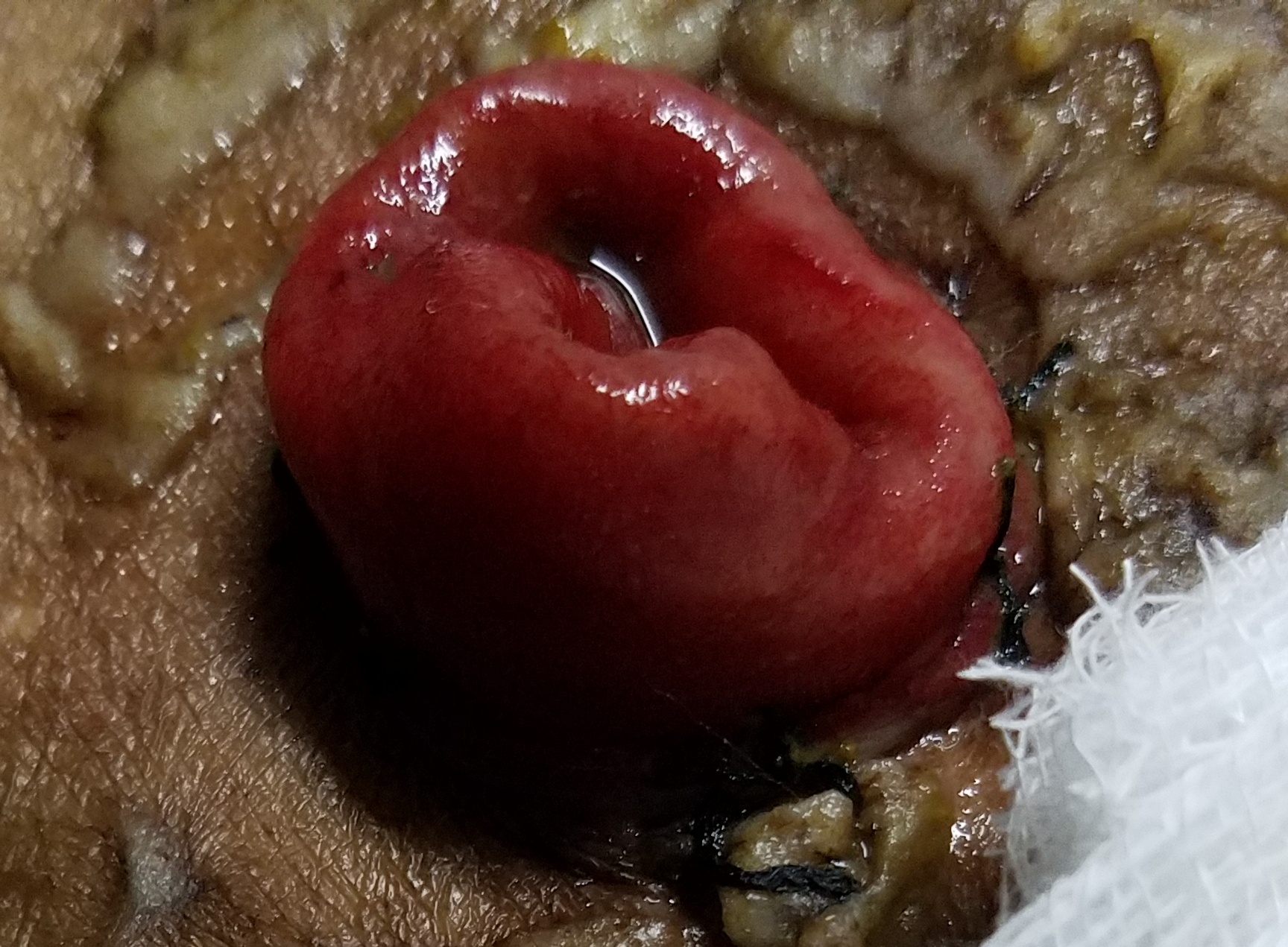
Before starting the procedure, all supplies should be arranged, and handwashing and donning of gloves should be done. The used stoma bag should be first emptied of all content, and then the flange removed by gentle traction on the bag or flange towards the stoma with counter-traction on the skin. An adhesive remover may also be used. The stoma and parastomal area should be gently cleaned with water, dabbed rather than scrubbed, without using soap. The stoma should be assessed and must be moist, above skin level, and pink to red in color, and the peristomal skin should be normal. Any deviation from this should be notified to the surgeon. The stoma should be measured, or the previous measurement remembered and size should not be more than 1/16-1/8.
The peristomal skin should be dried appropriately to allow good seal formation. Adhesive pastes or powders may also be applied peristomally. The paper cover on the back of the flange is then removed with the border tape in place. It is then placed around the stoma and held in place for 1 to 2 minutes to create an adequate seal. If it is a 2-piece bag, the bag is then clipped on to the flange. A belt may be applied around the abdomen and clipped to the sides of the flange to hold it in place. After this, safe disposal of the stoma bag, handwashing, and documentation of the procedure must be done.
Another integral aspect of colostomy care is mental health support through a thorough assessment of the patients’ psychomotor status as to how they are coping and dealing with the stoma. Poor body image perception, sexual dissatisfaction, and depression are common in patients with colostomies. Reassurance, psychiatric, and behavioral counseling may be needed to alleviate these symptoms.
Complications
Providers and nurses should monitor stomas at regular intervals to look for the multiple complications of colostomies as an integrated team approach. Some complications are extremely troublesome to patients, and they come to the hospital with these presentations, but others may be more occult and have to be looked for.
Minor troublesome complaints of the patient include offensive smell, the repeated requirement of draining the colostomy appliance, or repeated colostomy bag leakage. Offensive smells can be managed by stomal deodorants or deodorized colostomy bags or avoidance of food like fish, eggs, or onions that release such odors. Repeated bag leakage can be prevented by preoperative stoma site marking and reassurance and counseling in the postoperative period.
Moderately severe complaints include pain and skin excoriation around the stomal site, stomal diarrhea, or constipation or requirement for colostomy irrigation or enemas. Pain and skin excoriation may be managed by application of creams around the stomal site, with the application of the right size of the cut end on the back of the baseplate to be not more than 1/16 to 1/8 larger than the diameter of the stoma to prevent contact of fecal matter with the peri-stomal skin. Regular change of stomal appliances should be done, with the removal of the older bag with gentle pressure on the skin towards the abdomen and not with the severe force pulling the colostomy bag.
Colostomy diarrhea may be complained by the patient in case of ascending or transverse colostomies in case they are not fully explained about the nature of content expected, but stomal diarrhea may be the result of extensive resection with failure of bowel adaptation or if associated with short bowel syndrome. It may also be due to infectious causes like bacterial overgrowth or Clostridium difficile enteritis or secretory tumors like VIPoma, carcinoid, gastrinoma or radiation enteritis or due to medical disorders like hyperthyroidism or adrenal insufficiency in which case the fluid and electrolyte balance of the patient should be restored, with the possible use of anti-diarrhoeal agents and the underlying disorder treated appropriately. In the case of stomal constipation, the stomal obstruction should be ruled out by checking for absent or greatly increased bowel sounds, doing an X-ray abdomen in the anteroposterior view with the patient in the erect posture to rule out proximal obstruction or ileus.
Postoperative ileus may be present in the first few days after surgery, and the colostomy should be expected to be functional within 2 to 4 days after surgery, and the period of ileus may be reduced by early patient mobilization and following the ERAS (Enhanced Recovery After Surgery) protocol. Inter bowel adhesions may be a cause of obstruction in the late postoperative period. Enemas or irrigation of the stoma may be taught to patients with reasonably good results, but should be avoided in stoma prolapse, chemotherapy, pelvic or abdominal radiation treatments, diarrhea-producing medication or in case of an irregular functioning stoma and may lead to dependence.
Severe colostomy related complications include stomal gangrene seen commonly in the early postoperative period, stomal retraction, colostomy prolapse, parastomal herniation, mucocutaneous separation along with other surgical complications like SSI’s and wound dehiscence, postoperative atelectasis and pneumonia, urinary tract infections and DVT. Colostomy gangrene may be due to the disease process, if due to ischemia, involving the stoma or due to technical errors like tying the mesentery or making too narrow a defect in the rectus fascia, causing obstruction of the blood supply to the stoma. This should be managed by re-exploration and new stoma creation after resection of the diseased bowel. Stomal retraction is generally detected when the stoma bag is being changed and refers to the condition when the stoma passes below the level of the skin. It may recede inside the peritoneum, which leads to the discharge of fecal content inside the abdomen leading to peritonitis, which is an emergency.
Depending on the degree of retraction, it may be managed locally by pull up of the stoma and re-fixation to the surrounding skin or may require laparotomy and re-creation of the stoma with a metallic or plastic stoma rod passed through in the mesentery. This rod maybe even placed during primary surgery to reduce the chances of retraction. If the patient is planned for restoration of continuity soon, the surgery may be preponed and done in the same setting. Colostomy prolapse is commonly seen in transverse colostomies and is generally managed conservatively, however laparotomy with stomal revision may be required, especially in case of large prolapses with irreducibility. It is most commonly seen in the distal limb, especially in conditions where there is distal obstruction.
A novel method using a stapler device applied directly to the prolapsed stoma at the local stomal site has been found to be effective, reducing the need for laparotomy. A parastomal herniation is due to the creation of a wide defect in the rectus sheath through which the bowel passes and may lie in the subcutaneous plane, or may pass through the stomal opening in the skin if pressure increases. In severe cases, it may lead to bowel incarceration and strangulation. It is most commonly seen with end colostomies. It may be avoided by prophylactic mesh fixation of the stomal site during index surgery, but that might lead to infected mesh if the procedure is an emergency with an infected abdomen. If it does develop, laparoscopic modified Sugarbaker or keyhole procedures are currently in use with the Sandwich repair as an alternative and are found to have lesser rates of recurrence than the open parastomal hernia repair method. In cases where repair is not possible, resiting the stoma to the other side of the abdomen is better than another site on the same side.[8] Mucocutaneous separation can be treated by simply refixing the stoma to the skin edges using less gap between sutures. [9][10][11][5]
Clinical Significance
Colostomy creation is one of the most common surgeries performed by a general surgeon and is done for diversion or decompression of the remaining bowel or to protect a distal anastomosis. The most common type of colostomy is an end colostomy after a Hartmann procedure. Colostomy care is done through an integrated multidisciplinary team approach. It involves preoperative stomal marking and psychosocial counseling, colostomy creation, early postoperative stomal management for ileus and stomal edema, and application of colostomy bags. Furthermore, it is advisable to teach patients and their relatives about proper bag application and disposal and looking out for stoma related complications by the patient and the entero-stomal therapist in the late postoperative period.
The surgeon must call the patient for regular follow up to assess the condition of the stoma and look for any complications and also assess the disease process for which the colostomy was made and also plan for colostomy closure in case of temporary colostomies.
Enhancing Healthcare Team Outcomes
Colostomy creation and care is a major abdominal procedure, routinely performed in general surgery departments around the world, but have multiple possible complications as well as a severe psychosocial impact on patients. Thus it is imperative to have adequate preoperative guidance as well as intraoperative decision making and postoperative care so as to minimize morbidity and the psychosocial burden. A team approach is an ideal way to go about this, and the following should be done:
- The patient should be evaluated by a general or gastro surgeon to assess the necessity of stoma creation.
- He should be evaluated by a pulmonologist and cardiologist to assess and optimize lung and heart status and also tested for fitness by the anesthesiologist.
- An enterostomal therapist should then explain the procedure, address any concerns the patient might have, and mark the site for stoma creation.
- The nurse should teach the patient how to use an incentive spirometer.
- The stoma should be made by the general or gastro surgeon based on his best clinical judgment.
- In the postoperative period, the nurses or enterostomal therapist should perform colostomy care with the view to teach the patient how to go about it himself at home and also how to assess for complications.
- A physical therapist and a dietician should be contacted for early ambulation and parenteral or early enteral nutrition to reduce postoperative ileus.
- The patient himself performs colostomy care and must look out for complications once he is discharged from the hospital.
- A psychologist may be required to assess and address any psychosocial complications the patient might have regarding the colostomy or the appliance.
An integrated team approach is seen to be vital in colostomy preparation and management and has also been seen to reduce complications related to stoma creation as well as for psychosocial support. [Level 5]
Nursing, Allied Health, and Interprofessional Team Interventions
An integrated team approach has been seen to be essential in colostomy care. Colostomy care in most surgical wards around the world is done by the nursing staff and allied health care workers.
The nursing staff and enterostomal therapists help in deciding and marking the stoma site in the preoperative period. In the postoperative period, they teach patients how to manage and change their colostomy appliances as well as how to look out for complications.
Dieticians help patients in the postoperative period by preparing a diet chart individualized for the patient, based on his weight and the amount of bowel resected and the amount of functioning bowel. They also help to reduce and manage postoperative ileus.
Psychologists help manage the psychosocial aspect of colostomy creation and conduct counseling sessions and send patients to colostomy support groups.
Physical health therapists help in early patient ambulation in accordance with the ERAS protocol to decrease postoperative ileus and decrease the chances of developing DVT.[12][13]
Nursing, Allied Health, and Interprofessional Team Monitoring
Monitoring in colostomy care is an integral aspect to assess for complications and to plan for colostomy closure. It is generally done in hospitals by a team of allied health workers and the nursing staff.
In the hospital setup, in the early postoperative period, the nursing staff must check for viability and full functioning of the stoma and also look for complications like stoma gangrene. Also, general surgical complications like post-op DVT, atelectasis, and UTI must be looked for.
After discharge, the patients must be followed every couple of weeks to look for complications like stomal prolapse, retraction, and parastomal herniation. This is generally done by the nursing staff and, in case of complications, must be communicated to the treating surgeon for appropriate action.
The patients’ weight and body mass index (BMI) should be calculated at regular intervals by a dietician and be advised appropriate dietary and fluid management advice as well as vitamin and mineral supplementation to compensate for the reduced bowel length and reduced absorption.
The mental status of the patient should also be assessed at regular intervals, before and after stoma creation, by a psychologist.