Continuing Education Activity
Arthritis is defined as an acute or chronic joint inflammation in the joint. Arthritis may attribute to a wide variety of symptoms that include pain, stiffness, decreased range of motion, and joint deformities. There are several different types of arthritis, with management being different for each. History and physical examination are crucial in recognizing the type of arthritis, while additional laboratory and imaging may sometimes be necessary for confirming the diagnosis. This activity outlines the evaluation and treatment of arthritis and explains the role of the interprofessional team in managing patients with this condition.
Objectives:
- Review the epidemiology of arthritis.
- Describe the patient history associated with arthritis.
- Outline the imaging studies used in the evaluation of arthritis.
- Explain the importance of collaboration and communication among the interprofessional team to enhance the delivery of care to improve outcomes for patients affected by arthritis.
Introduction
Arthritis is derived from the Greek term “disease of the joints.” It is defined as an acute or chronic joint inflammation that often co-exists with pain and structural damage. [1] Arthritis is not synonymous with arthralgia, which refers to pain localized to a joint, regardless of the origin of the pain (which may or may not be due to joint inflammation). Arthritis affected both the Neanderthals and ancient Egyptians, but It was not until 1886 that Dr. John K. Spencer coined the term “osteoarthritis.” More than 100 different types of arthritis have been described, the most common being osteoarthritis or degenerative arthritis which is non-inflammatory arthritis. Inflammatory arthritis can occur in several settings, and inflammation can be caused by autoimmune processes (rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, etc.), crystal deposition induced inflammation (gout, pseudogout, basic calcium phosphate disease) or infections (septic arthritis, Lyme's arthritis). Inflammatory arthritis can also accompany other autoimmune connective tissue diseases such as systemic lupus erythematosus, Sjogren syndrome, scleroderma, myositis, inflammatory bowel disease, celiac disease, etc.
The goal of this activity is to provide a general overview of the most common arthritides and briefly touch on key aspects of the different major disease types.
Etiology
The etiology of arthritis varies with the type of arthritis. In osteoarthritis, the major contributory factors include advancing age, female sex, joint trauma, and obesity. Some genetic factors have been described such as mutations in genes encoding types II, IV, V, and VI collagens. [2][3]
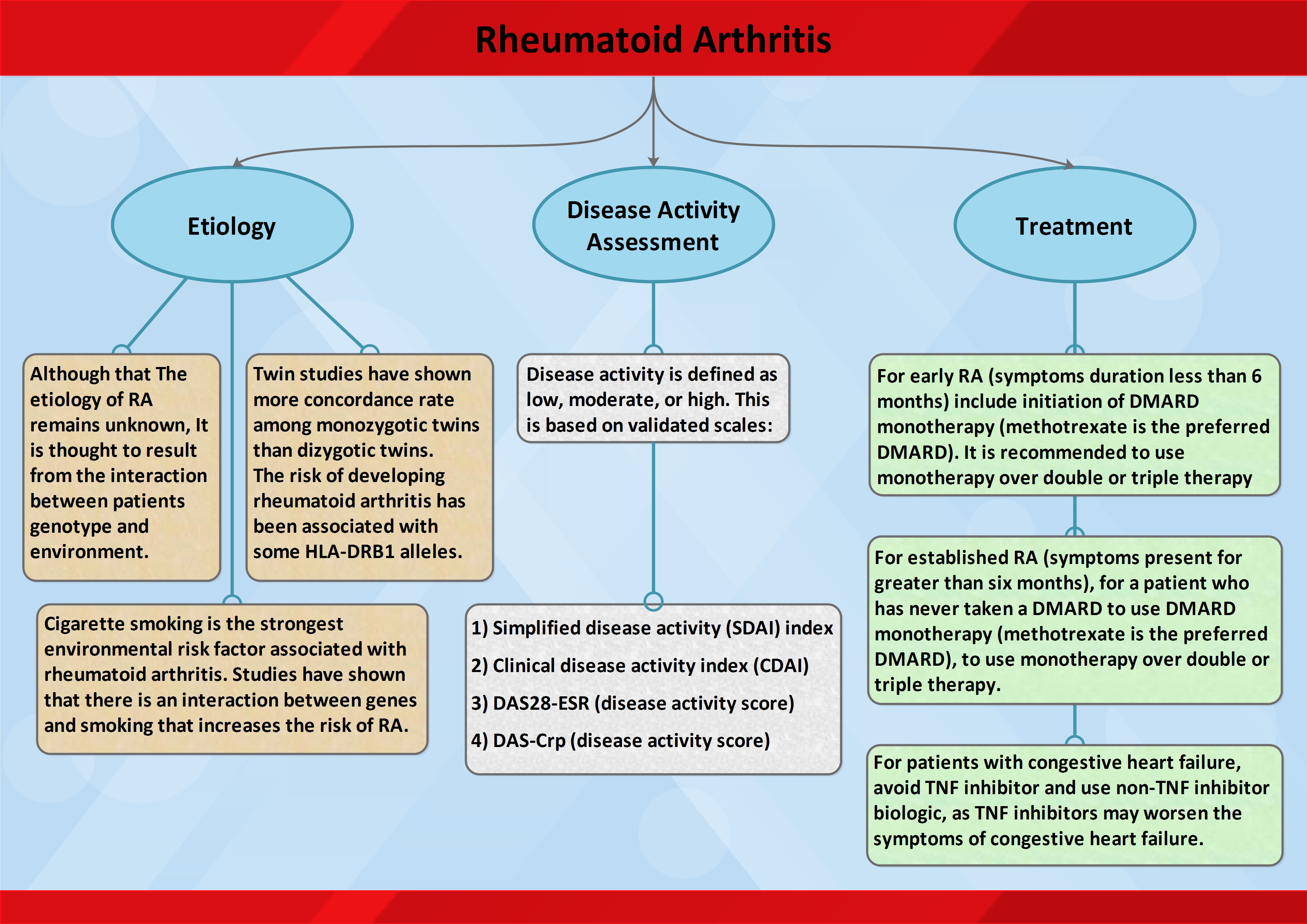
Rheumatoid arthritis (RA), on the other hand, is an autoimmune systemic inflammatory disorder. An interplay between several genetic factors (HLADRB1 and others) and environmental factors (smoking) leads to activation and dysfunction of the immune system leading to inflammation in RA.
In Gout, prolonged hyperuricemia leads to uric acid deposition in joints, which then leads to joint inflammation. There are several genetic mutations that can cause hyperuricemia, although this accounts for less than 10% of gout. The majority of patients with gout are under-excretors ie. they are not able to get rid of all the uric acid that is produced in them as a result of endogenous or exogenous purine metabolism. Male sex, advancing age, chronic kidney disease, alcoholism, and certain drugs such as the diuretics are additional risk factors for hyperuricemia and gout.
Septic arthritis is acute arthritis that is rare in the general population, but patients with pre-existing risk factors such as immunodeficiency, advancing age, diabetes mellitus, prosthetic joints, rheumatoid arthritis, and intravenous drug abuse are at a higher risk.
Arthritis can frequently be seen in patients with other autoimmune diseases and is one of the most common clinical features in patients with systemic lupus erythematosus (SLE). [4] Other diseases frequently associated with arthritis include inflammatory bowel disease, psoriasis, celiac disease, Sjogren syndrome, systemic sclerosis, dermatomyositis, mixed connective tissue disease (MCTD), etc.
Epidemiology
Over one-third of the American population has arthritis on imaging, and this number is bound to increase with the mean population age. [5] Of the arthritides, osteoarthritis is most prevalent. Between 19% and 30% of adults over the age of 45 years have knee osteoarthritis[6], 27% have osteoarthritis of the hand, and 27% have osteoarthritis of the hip. [7] It is estimated that 40% of men and 47% of women will develop osteoarthritis in their lifetime, with the incidence increasing to 60% if they have a body mass index greater than 30. [8]
Gout is the most common inflammatory arthritis in the United States, affecting more than 8 million individuals in the United States with a prevalence of 3.9%, [9] with a prevalence of more than 9% in individuals over 60 years of age.[10][11]The incidence of gout is more than 45 per 100,000. Notably, both the incidence and prevalence of gout is on the rise with more than 2 fold increase in over the past few decades.[12] The prevalence of pseudogout in the adult population is between 4% and 7% with over half of patients suffering from knee arthritis. [13]
Rheumatoid arthritis is found in approximately 1% of Caucasians, with females being affected more frequently than males (lifetime risk of 3.6% in women vs. 1.7% in men). [14] Disease onset is typically in early adulthood, with a disease prevalence of 5% in women over the age of 65.
Septic arthritis is typically caused by bacterial seeding of an already arthritic joint via the hematogenous spread, most often from skin or urinary tract infection. Septic arthritis has a prevalence of 0.01% in the general population and 0.7% in patients with rheumatoid arthritis. [15]
Pathophysiology
Osteoarthritis is characterized by a degenerative cascade of progressive cartilage loss which leads to bone damage. Characteristic findings include subchondral cysts, osteophytes, and subchondral plate thickening. Interleukin-6, monokines, interferon-induced protein-10, and macrophage chemotactic protein induce proteolytic enzymes such as matrix metalloproteinases, serine proteases, and cysteine proteinases and result in the degradation of joint collage. [16] Calcification of the surrounding articular cartilage reduces the thickness of and eventually destroys the cartilaginous matrix. Old age also is associated with a decrement in chondrocyte function, enhancing susceptibility to osteoarthritic degeneration.
Symptoms of rheumatoid arthritis are typically more severe than those of osteoarthritis. Rheumatoid arthritis is a systemic and chronic inflammatory state caused by an autoimmune response to an environmental trigger. The degradation of cartilage and, eventually, bone is preceded by endothelial cell activation and synovial cell hyperplasia. The pathology occurs following the aberrant production of inflammatory mediators (such as tumor necrosis alpha, interleukins 1, 6 and 8 and others following exposure to an antigenic pathogen). [17]
The monosodium urate salts of gout precipitate as needle-shaped crystals. This crystallization is more likely to occur in cooler body parts and with acidic conditions. Destabilization of these deposited intraarticular uric acid crystals leads to IL-1 mediated inflammatory response leading to the typical acute gouty arthritis flare. The process is different in pseudogout where the inorganic pyrophosphate from chondrocytes combines with calcium to form calcium pyrophosphate dihydrate. This crystal is deposited in joint spaces that have a predilection to osteoarthritic changes. Pseudogout crystal damage includes the fragmentation of bone and cartilage and the formation of osteophytes and subchondral cysts. Metabolic disorders such as hemochromatosis, hyperparathyroidism, or hypomagnesemia increase the likelihood of calcium pyrophosphate deposition. [18]
Septic arthritis is typically an inflammatory response to a monobacterial infection. Bacterial entry into the synovial fluid triggers a release of cytokines, chemokines, and proteases that degrade cartilage and trigger hyperplasia of the synovial membrane. Toxins produced by bacteria play an additional destructive role within the joint space itself. In adults, Staphylococcus aureus is the most common pathogen (with streptococci strains also being common). [19] Infection by gram-negative bacteria is more commonly seen as a result of trauma, intravenous drug use, immunosuppression, or in the elderly or very young.
History and Physical
History and physical examination plays a crucial role in the evaluation of arthritis and determining the type of arthritis, and differentiating symptoms from non-articular etiologies. The 1st step in the physical examination of a patient with musculoskeletal complaints should be determining and confirming if the pain is articular or not. Non-articular pain can be seen secondary to several pathologies including fibromyalgia, where patients have tenderness in articular as well as extra-articular areas, but no effusion, swelling, warmth or erythema localized to the joints. Tendinitis can also cause periarticular pain, a physical exam in these cases usually reveals tenderness along the tendon course or insertion without any focal tenderness or loss of range of motion of the joint.
Usual symptoms of arthritis are pain, swelling, loss of function, stiffness, deformity, weakness, and instability. They may also be accompanied by fatigue, sleep disturbance, emotional liability and symptoms of the underlying systemic illness. Pain from arthritis is usually worse by activities and at the end of the day. Inflammatory arthritis will also cause pain in the morning and at rest that may initially improve with activity, but subsequently gets worse with prolonged use and activity. Patients with fibromyalgia and myofascial pain syndrome usually complain of a diffuse all over pain. Neuropathic pain can be accompanied by paraesthesias in the nerve distribution. Morning stiffness lasting more than 45 minutes is typically associated with inflammatory arthritis, [20] but this is non-specific as patients with osteoarthritis or non-articular syndromes such as fibromyalgia can also have prolonged morning stiffness.
Physical examination is the most important tool in assessing arthritis and arthralgias. Inflammatory arthritis is associated with tenderness, swelling, effusion, erythema and warmth. These features are more obvious in an acute inflammatory arthritic process, but maybe less pronounced in chronic inflammatory arthritides. Osteoarthritis can also be associated with tenderness, swelling, and effusion, although erythema and warmth are usually lacking. Decreased range of motion and obvious joint deformity can also be observed in arthritis.
The next step shall be assessing the arthritis onset, the number of joints involved, symmetry, distribution, and pattern.
1. Onset.
Acute onset arthritis is typical of septic arthritis, crystalline arthropathies, and reactive arthritis. Osteoarthritis, on the other hand, is almost always insidious onset. Rheumatoid arthritis and psoriatic arthritis are of insidious onset in most cases, although occasionally they can be acute onset as well. Arthritis associated with underlying autoimmune disorders is usually insidious onset.
2. Number of involved joints.
Arthritis can be monoarticular (single joint), oligoarticular (2-4 joints) or polyarticular (several joints). Bacterial, Lyme's, mycobacterial and Neisseria infections present with acute monoarthritis. Monoarthritis is also seen in patients with gout (especially early in the disease), pseudogout, hydroxyapatite disease, and trauma. Rarely, psoriatic arthritis can have an initial presentation as monoarthritis, which may later evolve into oligo or polyarthritis. Chronic monoarthritis can be seen in patients with untreated infections (Bacterial, Lyme's, mycobacterial and fungal), gout, pseudogout, osteoarthritis, Pigmented villonodular synovitis, hemarthrosis, tumors, osteonecrosis, early oligoarticular juvenile idiopathic arthritis (JIA) and rarely in rheumatoid or psoriatic arthritis.
In general, diseases with monoarticular or polyarticular involvement can also present as oligoarthritis. However, oligoarthritis predominantly of the lower extremity joints (knees or ankles) is characteristic of HLA-B27 associated seronegative spondyloarthritides. A subgroup of patients with psoriatic arthritis present with oligoarticular involvement of small joints of the hands including the distal interphalangeal (DIP), proximal interphalangeal (PIP), and metacarpophalangeal (MCP) joints.
Polyarthritis can be caused by several inflammatory as well as non-inflammatory arthritides. The causes of inflammatory polyarthritis include rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, reactive arthritis, IBD associated arthritis, juvenile idiopathic arthritis, undifferentiated spondyloarthritis, gout, pseudogout and arthritis associated with underlying autoimmune diseases such as SLE and MCTD. Non-inflammatory polyarthritis can be seen in osteoarthritis, especially erosive osteoarthritis, nodal osteoarthritis, and primary generalized osteoarthritis.
3. Symmetry.
Polyarticular symmetrical inflammatory arthritis involving the small joints of hands and feet is the hallmark of RA. Other causes of symmetrical polyarthritis include JIA, psoriatic arthritis, pseudogout (pseudo-RA type), Adult-onset Still disease, arthritis associated with underlying autoimmune diseases such as SLE and MCTD and osteoarthritis, especially erosive osteoarthritis, nodal osteoarthritis, and primary generalized osteoarthritis. Asymmetrical polyarthritis can be seen in psoriatic arthritis, ankylosing spondylitis, reactive arthritis, IBD associated arthritis, juvenile idiopathic arthritis (pauciarticular or oligoarticular type), undifferentiated spondyloarthritis, gout, pseudogout, and osteoarthritis. As noted above, asymmetrical oligoarthritis of lower extremity joints can be seen in HLA-B27 associated seronegative spondyloarthritides.
4. Distribution.
Axial or spine involvement is common in osteoarthritis. Diffuse idiopathic skeletal hyperostosis (DISH) is another cause of non-inflammatory axial arthritis. Of the inflammatory arthritides, axial involvement is mostly seen in HLA-B27 associated seronegative spondyloarthritides including ankylosing spondylitis, reactive arthritis, IBD associated arthritis, psoriatic arthritis, undifferentiated seronegative spondyloarthritis, and non-radiographic axial spondyloarthritis. Other causes of inflammatory arthritides with axial involvement include JIA and SAPHO syndrome. Axial involvement is not seen in RA.
Several patterns on peripheral involvement can give a clue to the diagnosis. RA is typically associated with polyarticular symmetrical inflammatory arthritis involving the small joints of hands (MCP, PIP) and feet (MTP). Wrist, ankle and knee involvement is also common. However, DIP joints of the hands are usually spared in RA. DIP joint involvement can be seen in osteoarthritis, psoriatic arthritis, and gout. Knee, wrist and 2nd and 3rd MCP joints are the commonly involved joints in pseudogout. Pain, stiffness and limited range of motion of bilateral shoulders and hips due to underlying inflammatory arthritis and periarthritis is the hallmark of Polymyalgia rheumatica, although rarely, RA can have a similar presentation.
5. Pattern.
Progressive additive pattern with the ongoing involvement of more joints can be seen in RA, psoriatic arthritis and polyarticular osteoarthritis. A migratory pattern where arthritis moves from one joint to another with complete resolution in the previously involved joint can be seen in Whipple disease, neisserial arthritis, and rheumatic fever. An intermittent pattern can be seen in palindromic rheumatism, gout, pseudogout, familial Mediterranean fever, Adult-onset Still disease and Muckle-Wells syndrome, This is characterized by complete resolution of symptoms in the previously involved joints with the asymptomatic period lasting varying amount of time before arthritis recurs in the same or other joints.
Other clinical features that can assist narrowing the differential diagnosis include family history and the age of onset with osteoarthritis more common in the older population while inflammatory arthritides more common in younger adults. It is also important to closely evaluate the neighboring joints to rule out referred pain. Skin examination is crucial and can greatly assist in diagnosis (eg. skin psoriasis, subcutaneous nodules, tophi, lupus rashes, sclerodactyly, etc.).
Evaluation
Laboratory and radiographic evaluation can assist in the diagnosis and grading of the severity of an arthritic condition.
Inflammatory arthritides are associated with an elevation in markers of inflammation (ESR and CRP). Anemia of chronic disease is common. Leukocytosis can be seen in septic arthritis as well as gout, pseudogout and Adult-onset Still disease, while leukopenia and thrombocytopenia can be seen in RA and SLE-associated arthritis. Serum uric acid may be elevated in patients with gout, although this shall not be the sole diagnostic criterion. Serologies such as rheumatoid factor, anti-citrullinated peptide antibodies, Anti-Nuclear antibodies, and more specific autoantibodies shall be performed when appropriately indicated to assist diagnosis. [21]
Plain radiographs shall be the initial imaging modality. Joint space narrowing, osteophytes and effusion are common findings in osteoarthritis. Periarticular osteopenia is the first radiographic feature in inflammatory arthritis and erosions, joint space narrowing and secondary osteoarthritis developing later in the disease. Central "gull-wing" erosions are a feature of erosive osteoarthritis, while periarticular erosions are seen in RA. Entheseal calcifications can be seen in seronegative spondyloarthritis especially psoriatic arthritis and ankylosing spondylitis. Xrays in axial spondyloarthropathies are normal early in the disease but later can show bamboo spine and sacroiliac joint fusion and erosions. Axial osteoarthritis, on the other hand, presents with osteophytes, disc bulges, joint space narrowing on the X-ray. Pseudogout has characteristic radiographic features of chondrocalcinosis which is calcification of the cartilages, as can be seen in the menisci, triangular fibrocartilage of the wrist, or the cartilages of the 2nd/3rd MCP joints of the hands. X-rays in gout are normal early in the disease, but later, can show the presence of hard tophi, periarticular osteopenia and classic juxta-articular erosions (rat-bite erosions) with overhanging edges.
If radiographs are non-diagnostic, further imaging can be considered. MRI is a very helpful tool and can assist in evaluating the presence or absence of synovitis, erosions, sacroiliitis with a much higher sensitivity than X-rays. Further, MRI may assist in evaluating soft tissue or ligamentous injuries and tumors that are otherwise difficult to identify. CT-scan can assist in identifying bony deformities and can detect chondrocalcinosis but is performed mostly if MRI cannot be performed. Musculoskeletal ultrasound which is an evolving technique is extremely helpful especially in the evaluation of peripheral arthritis and can assist in evaluating the presence or absence of synovitis, effusion, erosion, structural defect such as rotator cuff or meniscus teat and can also assist in performing ultrasound-guided aspiration/injection. [22] Nuclear medicine joint scan is rarely indicated due to its high sensitivity but poor specificity but can assist in evaluating the presence or absence of inflammation, especially to evaluate prosthetic joint infections. Dual-energy CT scan is another evolving radiographic modality that is very accurate for assisting in gout diagnosis.
The synovial fluid examination is one of the most important tests especially for the initial diagnosis of arthritis. Cell counts and differentials, crystal evaluation under polarized light microscopy, bacterial/acid-fast bacilli/fungal cultures and Lyme's DNA PCR shall be performed on the synovial fluid as appropriate. Degenerative arthritis is usually associated with cell counts of less than 2,000 cells/mm3 while in inflammatory arthritis, cell counts are usually more than 5,000 cells/mm3 and may be as high as 50,000 cells/mm3. More than 50,000 cells/mm3 cells and/or more than 90% neutrophils in synovial fluid analysis shall raise suspicion of septic arthritis, although this can also be seen in the setting of acute gout or pseudogout. Gout crystals are needle-shaped and strongly negatively birefringent. Pseudogout crystals are rhomboid-shaped and are weekly positively birefringent. Basic calcium phosphate crystals are not visible on polarized light microscopy and need special staining to confirm positivity. A synovial biopsy is rarely performed but can be considered especially in cases of monoarthritis where other modalities have failed to provide a diagnosis. [23]
Treatment / Management
The management of osteoarthritic joints should aim to limit the pain and improve function. Usually, a combination of non-pharmacological (or conservative) and pharmacological treatments are required for optimal care. Non-pharmacologic treatments include specific exercises, physical therapy, bracing, acupuncture, and weight reduction. The pharmacologic management of osteoarthritis utilizes topical and oral medications. Frequently used medications include oral and topical non-steroidal anti-inflammatory drugs (NSAIDs), topical capsaicin, and duloxetine. Corticosteroids can be injected directly into the joint. In most instances, topical NSAIDs, capsaicin, and other ointments are first-line therapy, and oral NSAIDs are to be initiated if symptoms are not relieved by these, or the disease is more systemic. Duloxetine can be useful for patients that have medical contraindications to NSAID use and has been proven to be beneficial especially in osteoarthritis of the knees. If both non-pharmacological and pharmacological management fails, intra-articular corticosteroid injections might provide symptom relief. Opioids should be avoided. [24] Surgical replacement of the affected joint(s) is reserved for refractory symptoms and can be highly effective. Patients may experience post-surgical complications and limited function in the immediate post-surgical period is not unusual. [25] Physical therapy is necessary post-operatively to optimize patient outcomes.
The emphasis in the pharmacological management of rheumatoid arthritis and the seronegative spondyloarthropathies is on early disease remission and preventing radiographic progression. The early use of disease-modifying anti-rheumatic drugs (DMARDs) and biologics is more effective than treatment with glucocorticoids and NSAIDs. [26] Anti-inflammatories can be used as an adjunct to reduce the amount of inflammation while the disease remains active. Regular monitoring of symptoms and dose adjustment continues through symptom remission. Treatment of disease exacerbations may require corticosteroids when severe. [27]
In gouty arthritis, flare-ups can be quite debilitating and painful. The use of anti-inflammatory medications can provide substantial relief and shall be ideally initiated within 24 hours an acute gouty flare. These include oral corticosteroids, NSAIDs such as indomethacin or high-dose naproxen, or colchicine. The use of intra-articular corticosteroid injections may be useful for a patient with pauciarticular involvement, whereas the use of intramuscular or intravenous corticosteroids may be used if the patient is not able to take medications orally. Medications that decrease uric acid levels play no beneficial role in the treatment of an acute flare but are recommended for patients with recurrent flares, chronic kidney disease, nephrolithiasis or tophi. [28] The goal is to decrease serum uric acid burden which then decreases the intra-articular uric acid burden eventually leading to the resolution of gout is symptoms.
The treatment of septic arthritis requires draining the affected joint and the use of antibiotics. Cultures and sensitivities of the joint fluid determine the joints of antibiotics. [29]
Differential Diagnosis
Arthritis shall be differentiated from non-articular pain, including pain secondary to fibromyalgia, myofascial pain syndrome, neuropathy, tendinitis, and complex regional pain syndrome. Physical exam along with laboratory and radiographic imaging can help make this differentiation.
There are more than 100 different types of arthritis described and is important to have a definite diagnosis before initiating treatment.
Prognosis
Osteoarthritis is a progressive disorder with no cure. The prognosis depends on the number of joints and the severity of the disease. Rapid progression is likely in older patients, obese individuals, those with varus deformity and multiple joint involvements. After joint replacement, the outcomes are good but no prosthesis is permanent; thus revision may be necessary after 10-15 years. [30]
With recent advancements in therapy, the prognosis of rheumatoid arthritis has improved significantly, although morbidity and mortality in rheumatoid arthritis are significantly higher than the general population, predominantly due to the extra-articular manifestations.
Postoperative and Rehabilitation Care
Rehabilitation
Exercise programs have demonstrated significant benefits for individuals with osteoarthritis (OA) and RA within specific parameters. Benefits include improved aerobic capacity, muscle strength and mass, joint mobility, functional mobility, and pain reduction.
The type, intensity, and duration of exercise are important, as joint damage can occur with overuse or repetitive activities for these patients. Literature highlights the risk of sport-related injuries, necessitating modifications for patient safety during sporting activities. The current literature also suggests that individuals early in their diagnosis will respond better than those at progressed stages of arthritis. Aerobic conditioning, resistance training, and balance training should be incorporated based on the individual's deficits and goals. Collaboration among therapists and practitioners ensures coordinated care.[31][32][33][34]
Deterrence and Patient Education
Patient Education is one of the most important aspects of patient management. Education about the disease process, exacerbating factors, signs, and symptoms to monitor and diet and lifestyle modification including weight loss, exercises, and muscle strengthening may improve long-term outcomes in patients with various different types of arthritides.
Pearls and Other Issues
Arthritis is a broad and complex topic with many types, subtypes, and variations. The above is a summary of this expansive subject and does not aim to cover it in its entirety. It does, however, aim to provide an introductory synopsis of the arthritides and give the reader the knowledge to diagnose and treat this condition in most settings.
Enhancing Healthcare Team Outcomes
Arthritis may be a disease of the joint but it also has systemic repercussions. There is no cure for osteoarthritis and it can severely diminish the quality of life and lead to depression. Depending on the type of arthritis, there may also be other organs involved. The management of arthritis is ideally done by an interprofessional team that includes a nurse, dietitian, rheumatologist, physical therapist, orthopedic surgeon, pain specialist, pharmacist, and an internist. Guidelines by the American College of Rheumatology encourage an interprofessional approach. Polypharmacy is a major concern in these patients because of the need to resolve the pain, hence the pharmacist should closely monitor the medications to prevent serious drug interactions and if narcotics are required, monitor for overuse. Almost all patients may benefit from physical rehabilitation and physical therapy. Ample evidence indicates that water-based exercise can diminish pain and improve joint function. Further, loss of weight also decreases the stress on the joint. In addition, a dietitian can help educate the patient on a healthy diet. The nursing team should assist the clinician in educating the patient on medication compliance, abstaining from alcohol, and discontinuing smoking. Since arthritis is a progressive disease, all patients should be urged to have close follow up with the primary care provider. A referral to a pain consultant early in the course may help prevent abuse of narcotics and other prescription-strength pain medications. (Level V)