Issues of Concern
Children
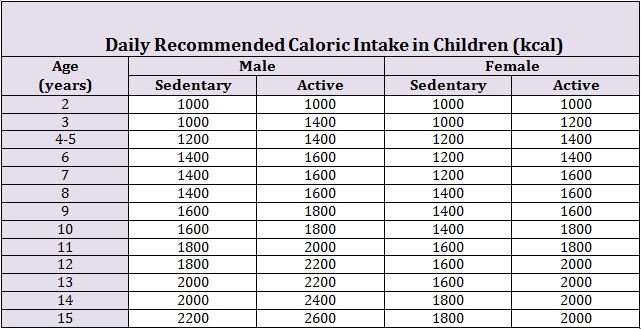
In children, the daily caloric requirement is calculated based on the age, sex, and activity status of the child. For a child between 2 and 3 years of age, the recommended daily caloric intake is 1000 to 1400 kcal/day; this requirement increases with the age of the child. Children during a growth spurt, require higher amounts of calories to maintain the body as well as to grow. The daily recommended caloric intake for children 11 to 12 years range between 1800 and 2200 kcal/day. Another way to generalize caloric need is that an infant needs 100cal/kg/day, ages 1 to 3 years need 80 kcal/kg/day, 4 to 5 years needs 70kcal/kg/day, 6 to 8 years needs 60 to 65 kcal/kg/day and 9+ needs 35 to 45 kcal/kg/day. Growth charts are vital in directing nutritional counseling in children.
The daily recommended intake (DRI) of water depends on age, sex, weight, activity status, air temperature, and humidity. Plain water serves as the best way to fulfill this requirement. In a recent study, adequate plain water intake in children was more in high-income households, while 75% of children fail to meet the DRI.[1] For infants weighing between 3.5 kg to 10 kg, the daily fluid requirement is 100 ml/kg. For children 11 kg to 20 kg, the daily water requirement is 100 ml/kg for the first 10 kg and 50 ml/kg for every kg above 10 kg. For children above 20 kg, the fluid requirement is calculated as 1500ml for 20 kg and 20 ml/kg for every kg above 20 kg, but more than 2400ml of fluid should not be administered at once.
Another way to calculate daily fluid requirements is the 4-2-1 rule with 4ml/kg/hr for the first 10kg of weight and then 40ml/hr +2ml/kg/hr for kg 10 to 20 and then 60ml/hr +1ml/kg for every kg >20. With this formula, a 5kg child would need 20ml/hr or 480ml/day, and a 25kg child would need 65ml/hr or 1,5860 ml/day. Under-nutrition accounts for more than 3 million deaths in children < 5 years per year globally. Factors resulting in a diet that is low in quality include lack of knowledge, poverty, palatability, time scarcity, and lack of availability.[2][3]
Adults
The daily-recommended caloric intake for adult males and females is 2600-2800 kcal/day and 2000-2200 kcal/day, respectively. This requirement is not static and depends significantly on the activity status and the physical condition of the body. Imbalance in the diet leads to under-nutrition and over-nutrition, both of which are harmful to the body. The daily water requirement of the body depends on age, weight, sex, and air temperature. The DRI of water for men and women aged 19 to 30 years is 3.7 L/day and 2.7 L/day, respectively. In an analysis done in the USA, the estimated median total water intake of males and females aged between 19 to 50 years was 3.5 L/day and 3.0 L/day, respectively.[4] In a recent study, 83% of females and 95% of males ≥71 years of age failed to meet the DRI of water.[5]
Pregnant Women
Nutrition plays a vital role in pregnancy. The recommended weight gain during pregnancy depends on the prepregnancy body mass index (BMI). Underweight women (BMI<18.5) before pregnancy are advised to gain 28 to 40 lbs throughout their pregnancy, normal (BMI 18.5 to 24.9) 25 to 35 lbs, overweight (BMI 25 to 29.9) 15 to 25 lbs, and obese (BMI>30) 11 to 20 lbs. Pregnant women do not need to increase their daily calories during the first trimester. During the second trimester, added 340 calories per day are recommended, and then 450 extra calories per day in the third trimester.
Excess weight gain during pregnancy can lead to maternal and fetal complications. Maternal complications include cesarean delivery, retention of weight after delivery, and postpartum depression. An increased incidence of obesity, allergy, asthma, and cancer is seen in children of mothers who had excess weight gain during pregnancy. The National Research Council guidelines also recommend a range of weight gain for women carrying twin fetuses. Women with normal pre-pregnancy weight should gain 17kg-25 kg, while overweight and obese women should gain, 14kg-23kg and 11kg-19kg, respectively. It is important to ensure that women conceive while they are in the normal weight category; preconception counseling and adequate contraception should be discussed. The healthcare provider should track the weight gain during pregnancy and should guide the pregnant females regarding adequate dietary changes.
A prenatal vitamin should be taken before conception and then throughout pregnancy and breastfeeding. Adequate intake of folate (400 mcg/day) in the first trimester decreases neural tube defects. The recommended intake of iron doubles to 30 mg/day to assist with increased blood production. Vitamin D requirements increase to 600 IU per day, and calcium intake remains 1000 mg/day. Protein requirement increases from 0.8g/kg/day to 1.1g/kg/day. Fluid requirements also increase to 3 liters per day. Women should not avoid highly allergenic foods as a prophylactic measure during pregnancy. Women who follow certain diets may continue to do so with the assistance of their physician to ensure the meeting of all dietary needs.
Athletes
The nutritional requirements for athletes vary based on intensity and type of training. Physicians need to consider body composition and not just body weight when determining the needs of athletes. Special circumstances to consider would be a desire to gain weight, lose weight, build muscle, training in excess heat, training at high altitudes, and how much time in a day is spent in training. Hydration is important for maximal performance, so athletes should be sure to hydrate the 24 hours before an event, in the hour before their event, during their event, and then recovery after their event.[6]
Clinical Significance
The deficiency of any one of these nutrients can cause serious health concerns. Hence, it is essential to consume a diet that is rich in both macronutrients and micronutrients.
Carbohydrates
About 50 to 55% of the daily calories should come from carbohydrates, which are composed of monosaccharides that include fructose, glucose, and galactose. Each gram of carbohydrate contains energy equivalent to 4 kcal. Complex carbohydrates with a low glycemic index steadily raise the blood sugar level and are preferred over simple carbohydrates such as dextrose.[7] The limitation of simple sugars should be 5 to 10% of the daily caloric requirement. Legumes, whole grains, beans, fruits, and vegetables should be consumed to fulfill the daily requirement of carbohydrates.[8]
Proteins
Proteins are comprised of subunits called amino acids. These subunits provide energy and are essential for the construction of structural units of the body e.g., muscle, bone, and ligaments. Around 30% of the dry body weight is attributed to proteins. Approximately 20% of daily calories should come from sources rich in protein such as red and white meat, egg, and legumes. The daily recommendation for protein intake is 1.6 g/kg body weight for an adult. Some amino acids e.g., leucine and valine, are called essential; these are not synthesized by the body and must be obtained in the diet. Plant-sourced proteins, when consumed in replacement to animal proteins, have been shown to decrease cancer and cardiovascular disease-related mortality in a large prospective study.[9]
Marasmus is a type of protein-energy malnutrition resulting from the deficiency of energy-producing nutrients such as carbohydrates, proteins, and fats. On physical examination, the patient has generalized wasting, loss of subcutaneous fat, and muscle bulk. Another type of protein-energy malnutrition is kwashiorkor, which occurs in children consuming a diet that may be rich in energy but is deficient in proteins. The presence of skin findings e.g., pedal edema, dermatitis, skin depigmentation, hair loss, and loosening of teeth, differentiate kwashiorkor from marasmus. However, a child with marasmus can develop pitting edema due to protein deficiency; this is marasmic-kwashiorkor.[10]
Fats
Fats are composed of glycerol and fatty acids; these are high energy molecules that help the body grow, keep it warm, and serve as an inventory in case of emergency. Certain fatty acids (essential), e.g., omega-3 and omega-6, are required for the synthesis of eicosanoids such as prostaglandins and leukotrienes and should be consumed in the diet. About 25 to 30% of the daily calories should come from fats, out of which saturated fats should not be more than 10%.[11]
Cholesterol can be synthesized by the human body and hence is not essentially necessary in the diet. However, when consumed, it should not be more than 300 mg/day. A high-fat diet can lead to the development of obesity and is associated with an increased risk of cardiovascular disease.[12][11] Intake of fats can be reduced by replacing red meats, fried food, and fat-containing dairy products with white meat and fat sources that are rich in monosaturated fats e.g., olive oil, avocado, nuts, and flaxseed. A recent study reported that people consuming a diet rich in monosaturated fats were at a decreased risk of developing cardiovascular disease, type II diabetes mellitus, and cognitive decline.[8]
Dietary Fiber
Fiber improves digestive health by creating bulk in the stool and stimulating peristalsis. It prevents constipation and diarrhea and is a protector against colon cancer. Fruits and vegetables are the chief sources of fiber, and the recommendation is that one should consume at least five servings/day. The daily recommended amount of dietary fiber intake is 38 gram/day and 25 gram/day for men and women age 19 to 50 years, respectively. In children, the goal fiber intake is age+5 grams. Consuming a diet rich in fiber can help improve the lipid profile, increase tolerability to statins, and reduce the risk of developing atherosclerosis hence preventing cardiovascular disease.[13]
Minerals and Trace Elements
Calcium and phosphorus are required for healthy bone development, while potassium, sodium, and chloride are the major electrolytes in the intracellular and extracellular compartments. An imbalance of these electrolytes can lead to drastic fluid shifts. Trace elements such as chromium, copper, and selenium also play an essential role in metabolic reactions, and their deficiency can lead to various diseases. The recommended daily allowance (RDA) of calcium is 1000 mg for both male and female adults. Females require an increased quantity of iron as compared to men due to the cyclic loss of blood during menstruation; hence the RDA for iron is 18 mg in females as compared to 8 mg in males. RDA for copper, zinc, and selenium is 30 μg, 900 μg, and 55 μg, respectively. Salt intake should be limited to fewer than 6 grams per day, as an increased quantity could lead to the development of hypertension.
The DASH diet, which is low in sodium and fat, helps improve hypertension and total cholesterol. In a recent study, the consumption of the DASH diet led to a 13% reduction in 10 years of Framingham Risk Score for cardiovascular disease in the subjects.[14] Iron deficiency can cause microcytic hypochromic anemia, as iron is an essential component of hemoglobin. In a study by Sehar et al. done in Pakistan, an estimated 500 mg of the iron reserve is necessary to meet the increased demands of pregnancy, while only 20% of the females have this reserve.[15] The thyroid gland uses iodine for the formation of thyroxine and triiodothyronine. The deficiency of iodine causes a decreased production of thyroid hormone, which leads to increased production of thyroid-stimulating hormone (TSH). Increased TSH upregulates thyroid hormone production and also causes the growth of the thyroid gland resulting in goiter. Calcium and phosphorus are vital for healthy bones, and their deficiency can lead to diseases such as osteoporosis and hypophosphatemic rickets.
Vitamins
Water-soluble (B, C) and fat-soluble (A, D, E, and K) vitamins have several vital roles. Vitamin A, also called retinol (RDA= 700 μg-900 μg retinol activity equivalents (RAE)/day), plays an essential role in the regeneration of epithelial cells and the development of rhodopsin, a photoreceptor pigment in the retina. Deficiency of vitamin A can cause xerophthalmia, keratomalacia, and night-blindness. A cross-sectional study done on pregnant and lactating women in Ethiopia revealed that 13.7% of the women had night blindness, and 0.4% had Bitot's spot.[16]
Thiamine (vitamin B1, RDA= 1.1mg/day) in the form of thiamine pyrophosphate (TPP) serves as a coenzyme in catabolic reactions of sugars and amino acids. Deficiency of vitamin B1 can cause wet beriberi, dry beriberi, and Wernicke-Korsakoff syndrome. Wernicke syndrome has distinct features of ophthalmoplegia, gait disturbances, and confusion, while Korsakoff syndrome includes confabulation and amnesia. It is a medical emergency and should be treated with intravenous thiamine and dextrose.
Scurvy presents with symptoms of skin bruises, petechiae, loosening of teeth, bleeding gums, slow wound healing, and mood changes. It occurs due to deficiency of vitamin C (RDA= 90 mg/day), which acts as a cofactor for both prolyl hydroxylase and lysyl hydroxylase, which help stabilize collagen. Collagen is a structural protein and is essential for healthy blood vessels, bones, cartilage, and connective tissue.
Vitamin D (RDA= 600IU/day) helps the absorption of calcium from both the gut and kidneys. A deficiency of vitamin D in childhood and adulthood can cause rickets and osteomalacia, respectively. On physical examination, children with rickets present with frontal bossing, pigeon chest deformity, bowing of legs, and rachitic rosary.
Vitamin E (RDA= 33IU/day [synthetic]) is an antioxidant, and its deficiency can lead to neurotoxicity and anemia.
Vitamin K (RDA= 120μg/day) plays an important role in the coagulation cascade. The gut flora helps convert vitamin K1 into vitamin K2, which is one of the main sources of the vitamin.
Water
Dehydration can occur due to inadequate consumption of water and classifies into three categories based on the percentage of body fluid loss. Loss of <5%, 5% to 10%, and >10% of body weight loss categorizes as mild, moderate, and severe dehydration, respectively. WHO has classified dehydration into no, some, and severe dehydration based on the physical examination. Patients with severe dehydration are lethargic, have sunken eyes, skin pinch goes back slowly, and the patient cannot drink on his own.
Patients with some dehydration are irritable, drink eagerly, have sunken eyes, and the skin pinch goes back slowly. Those with normal physical features are labeled as having no dehydration. Mild to moderate dehydration is treatable with oral fluids, while patients with severe dehydration or shock should be treated with intravenous fluid replacement. A recent study reported that people consuming less than the recommended amount of water per day have a constantly elevated level of serum arginine vasopressin (AVP). This hormone promotes reabsorption of water from kidneys and constricts arterioles to raise blood pressure.[17]
In a recent systematic review, decreased intake of water was related to a higher incidence of urolithiasis. While adequate water intake does not diminish the incidence of obesity or type II diabetes mellitus, it most certainly reduces the daily caloric intake.[18] Plain water is the ideal beverage to consume to fulfill the daily water requirement.[19]
Nursing, Allied Health, and Interprofessional Team Interventions
Every patient should be interviewed, examined, and investigated for potential malnutrition or overnutrition. Patients with dehydration may present with low blood pressure and increased heart rate. Nursing staff should be cautious and should work in collaboration with the physician to administer the right type and quantity of fluid. In severely dehydrated patients, it is necessary to have two wide bore cannulas in place. 0.9% normal saline is the fluid of choice.
In children, a bolus of 20 ml/kg of 0.9% normal saline should be administered in 10 to 20 minutes. If the vitals do not improve, the bolus dose can be given again. In adults, a 500 ml bolus of crystalloid fluid e.g., 0.9% normal saline, should be administered in 10 to 20 minutes. If no improvement occurs even after the administration of 2000 ml of fluid, then expert help should be taken.
Primary care providers should keep an eye on the nutritional status and development of new signs and symptoms in their patients. Clinicians practicing emergency medicine often get to see patients with a history of alcohol abuse. They can diagnose nutritional deficiency and the diseases related to it. Gynecologists and primary care physicians should pay special attention to females planning to conceive; multivitamin supplements, which include folic acid, iron, and calcium, should be prescribed. In children or elderly with severe malnutrition, cautious refeeding should be started, electrolyte abnormalities should be corrected, and the clinical team should initate activity to prevent hypoglycemia.