Continuing Education Activity
Neisseria gonorrhoeae, an obligate human pathogen, is a sexually transmitted disease that causes consequential worldwide morbidity both in resource-abundant and resource-limited nations, and its diagnosis and treatment require costly expenditures annually. Like other sexually transmitted infections (STIs), gonorrhea disproportionately impacts young adult populations. The obligate pathogen N. gonorrhoeae infects only humans in nature and most commonly manifests as urethritis in men and cervicitis in women. This activity illustrates the presentation, evaluation, and treatment of N. gonorrhoeae and the interprofessional team's role in treating patients, and their partners, with gonococcal infections.
Objectives:
- Summarize the etiology of N. gonorrhoeae.
- Review the appropriate evaluation of gonorrhea.
- Outline the treatment options available for gonorrhea.
- Explain the importance of improving care coordination among the interprofessional team to enhance the delivery of care for patients with N. gonorrhoeae infection.
Introduction
Neisseria gonorrhoeae, an obligate human pathogen, is a sexually transmitted disease that causes consequential worldwide morbidity both in resource-abundant and resource-limited nations, and its diagnosis and treatment require costly expenditures annually.[1][2] Like other sexually transmitted infections (STIs), gonorrhea disproportionately impacts young adult populations.[3] An ancient disease with biblical references (Hebrew Bible; Leviticus 15:1-3), gonorrhea has many slang references, including “the clap,” which likely derived from the name of the ancient Parisian red-light district Les Clapiers.[4]
Etiology
The obligate pathogen N. gonorrhoeae infects only humans in nature and most commonly manifests as urethritis in men and cervicitis in women.[4] Obligate pathogens are bacteria that must manifest disease to facilitate transmission from one host to another. To survive, these bacteria must infect a host and cannot survive outside of a host. Undiagnosed and/or untreated gonorrheal urogenital infections can ascend through the upper urogenital tract and cause many severe reproductive complications, most commonly but not exclusively in women, such as endometritis, pelvic inflammatory disease, infertility, and/or life-threatening morbidity via ectopic pregnancy.[5]
Epidemiology
A major public health concern, N. gonorrhoeae, is currently the second most common cause of bacterial sexually transmitted infections worldwide.[5] The World Health Organization (WHO) estimates that 106 million new gonorrhea cases are documented among adults annually worldwide; many more infections go unreported.[6] With more than 500,000 cases noted annually in the United States, N. gonorrhoeae is the second most commonly reported sexually transmitted disease in the United States.[1]
Gonorrhea infection has a slight male prevalence secondary to the increased likelihood that males will manifest urogenital symptoms and also due to increased diagnoses among men who have sex with men.[1] Over the last decade, the incidence of gonorrheal STIs has increased due to the rising number of antibiotic-resistant strains.[2]
Pathophysiology
N. gonorrhoeae infection starts with the adhesion of gonococci to epithelial cells, followed by local cellular invasion. Gonorrhea has multiple surface proteins that facilitate adhesion. N. gonorrhoeae utilize pili to initiate adhesion to epithelial cells. Hair-like appendages, pili, cover the bacterial surface. Their ability to lengthen and retract allows the bacteria to attach from a distance and move closer to the epithelial cells, promoting cellular invasion. Pili also provide motility and protection.[7] Other surface proteins involved in cellular attachment include Opa, opacity-associated proteins, and LOS, lipooligosaccharide. LOS attaches to sperm cells and likely leads to transmission from males to uninfected sexual partners.[8]
Invasion of cervical epithelium involves bacterial cells interacting with host cell complement receptors type 3 (CR3). This communication is initiated by the binding of pili to the CR3.[9] This causes extensive rearrangement of the host cell actin, resulting in large projections called ruffles.[10] Ruffling then allows gonococci to enter host cells in large vacuoles called macropinosomes and subsequently multiply within infected cells.[11]
Neisseria gonorrhoeae induces localized infection at the anatomic site of inoculation, typically the urethra, cervix, pharynx, or anus in adults and the eye conjunctiva or the pharynx of newborns, but dissemination can occur.[6] Gonococci are classified as either serum-sensitive or serum-resistant based on their sensitivity to killing by complement activation; serum-resistant strains have the potential to cause disseminated infection.[12] N. gonorrhoeae has evolved multiple mechanisms to combat the innate and adaptive immunity systems of their host organisms’ immune defenses.[4]
Histopathology
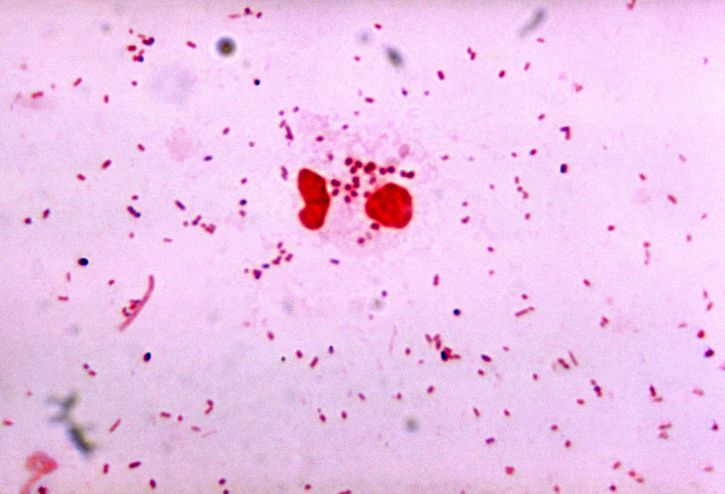
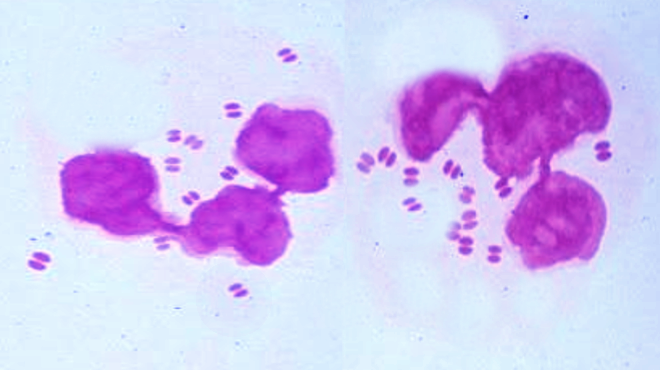
Light microscopy of Gram-negative or methylene blue-stained smears of N. gonorrhoeae urethral or cervical mucus samples will demonstrate neutrophils with intracellular diplococci. Light microscopy has high sensitivity and specificity for symptomatic males with urethral discharge; however, light microscopy has a lower sensitivity for diagnosing cervical, pharyngeal, and rectal gonorrhea.[4]
History and Physical
In females, N. gonorrhoeae most commonly infects the cervix, resulting in cervicitis. When female patients with gonococcal urogenital infections have symptoms, they may complain of vaginal discharge, dysuria, or pelvic pain.[1][13] Gonorrheal infection of the Bartholin’s glands adjacent to the vaginal introitus manifests as labial soft tissue swelling, abscess formation, and pain.[14] If cervicitis goes undetected and untreated, ascending gonococcal infection can result in upper reproductive tract involvement, such as salpingitis and pelvic inflammatory disease. Pelvic inflammatory disease can manifest with pelvic pain, infertility, and increase the risk of ectopic pregnancy.[1][15] Gonococcal infections complicating pregnancy can lead to adverse pregnancy outcomes such as low birth weight newborns and transmission to newborns resulting in oropharyngeal or conjunctival infections.[15]
Although more than 50% of females will not manifest symptoms of their gonococcal cervix infections, most males, more than 90%, will manifest urogenital gonorrhea symptomatically.[4][13] The most common clinical manifestations of gonococcal disease in males include penile purulent discharge, dysuria, and testicular discomfort.[13] Male urogenital gonococcal complications include orchitis, epididymitis, penile lymphangitis, penile edema, and post-infectious urethral strictures. The prevalence of rectal and pharyngeal gonococcal infections has been increasing among populations of men who have sex with men.[3]
Like cervicitis, gonococcal infection of the pharynx, the rectum, and the female urethra often present asymptomatically or with subtle symptoms.[1] If left untreated, gonorrheal infection of the rectum can proceed to manifest with rectal pain, bleeding, discharge, and proctitis.[1] Uncommonly, N. gonorrhoeae manifests systemically as fever/septicemia, tenosynovitis, arthritis, and vasculitis.[15]
Evaluation
Diagnostic laboratory assays are essential to confirm the clinical suspicion of gonorrhea. Laboratory confirmation of N. gonorrhoeae infection is made by direct detection of the gonococcal pathogen in urogenital, anorectal, pharyngeal, or conjunctival swab specimens or first-catch urine.[15]
Populations that engage in anogenital sexual intercourse and/or insertive oral sex will require screening for gonorrhea from the anus and pharynx in addition to urogenital screening.[3] Confirmation of the clinical suspicion of gonorrhea is established by detecting N. gonorrhoeae or its genetic signature in genital or extragenital samples by light microscopy of stained smears, culture, or nucleic acid amplification tests (NAATs).[4]
The routine utilization of NAATs to screen at-risk asymptomatic patients have demonstrated that pharyngeal and rectal gonococcal infections are not uncommon manifestations.[13] NAATs are generally more than 95% sensitive and specific in urethral and cervical swabs and first catch urine of males.[13]
The development of commercially available point-of-care assays for N. gonorrhoeae infection has impacted the time to treatment. However, while these point-of-care assays have few false-positive results, i.e., they demonstrate high levels of specificity, their sensitivity profiles range widely, with false-negative rates varying from 13% to greater than 90%.[16] Repeat laboratory screening after patient and partner treatment for gonococcal infection enhances eradication efforts.[16] Recently, the development of multiplex NAATs allows for the screening of an extensive panel of STDs in addition to N. gonorrhoeae.[15]
Treatment / Management
Empiric therapy for gonococcal infections is often administered during the initial clinical visit based on historical factors such as sexual intercourse with a person with an STI or a clinical exam suspicious of an STI, such as penile drip or abnormal vaginal discharge. Worldwide N. gonorrhoeae STI treatment for urogenital infections in males and females most commonly consists of dual therapy with a single intramuscular or intravenous dose of 500 mg ceftriaxone.[2][6] In patients 150 kg or more, 1 g of ceftriaxone should be given. If the clinician has not ruled out chlamydial infection, then treatment for chlamydia is with doxycycline 100 mg orally twice a day for seven days unless the patient is pregnant.)
In Canada, an alternative antimicrobial regimen is favored for first-line N. gonorrhoeae treatment of urogenital infections, a single dose of oral cefixime 800 mg paired with a single dose of azithromycin 1 g.[6] Of note, 2 g of oral azithromycin and 800 mg of oral cefixime have notable gastrointestinal adverse effects, such as vomiting.[6] Cefixime does not provide as high or sustained bactericidal blood levels as ceftriaxone. It demonstrates limited treatment efficacy for pharyngeal gonorrhea.
For complicated gonococcal infections, including pelvic inflammatory disease (PID), epididymitis, and proctitis, dual therapy with a single intramuscular or intravenous dose of 500 mg of ceftriaxone is paired with oral doxycycline 100 mg BID for seven days, rather than a single 1 g dose of azithromycin, because of doxycycline’s effectiveness against C. trachomatis and documented efficacy in treating epididymitis and proctitis.[3] Directly observed therapy, endorsed by the World Health Organization, of gonococcal therapy promotes adherence to therapy and limits treatment failures secondary to noncompliance.[17]
N. gonorrhoeae has evolved antimicrobial resistance utilized for its treatment since the first use of sulfonamides in the 1930s. In some parts of Asia and Europe, gonococcal isolates exhibiting elevated mean inhibitory concentrations to ceftriaxone have been identified, and ceftriaxone treatment failures have been reported. When there is a high suspicion or confirmation of N. gonorrhoeae resistance to standard therapy based on culture and sensitivity results, treatment of urogenital infection with a single dose of gentamicin 240 mg IM with a single dose of azithromycin 1 g orally can be administered.[18]
In patients with a documented life-threatening allergy to cephalosporins or B-lactam allergy, aztreonam monotherapy can be utilized to treat N. gonorrhoeae infections. Aztreonam 1 g administered intravenously treats urogenital gonorrhea and may also have efficacy for pharyngeal and rectal gonococcal infection when using a 2 g dose.[2]
Differential Diagnosis
Urogenital symptoms induced by gonorrhea can be observed with other sexually transmitted diseases, as well as non-sexually transmitted illnesses. Sexually transmitted infections that can cause dysuria, penile discharge, abnormal vaginal discharge, and pelvic pain include Chlamydia trachomatis, Trichomonas vaginalis, Treponema pallidum, Mycoplasma genitalium, and herpes simplex virus.[3]
Acute gonococcal infection can impact multiple organ systems. Infectious and noninfectious diseases can cause urethritis, cervicitis, proctitis, conjunctivitis, pharyngitis, and arthritis. Autoimmune, neoplastic, traumatic, and toxicologic etiologies must be considered when evaluating patients presenting with symptoms that raise suspicion of gonorrhea. The gonococcal infection itself can have autoimmune manifestations such as reactive arthritis in association with urethritis and conjunctivitis.[1]
Prognosis
Gonorrhea morbidity has risen over the last 20 years, secondary to the progression of antimicrobial resistance.[2]
Complications
Complications from gonorrhea result in substantial morbidity and socioeconomic consequences. If gonorrhea infections are not detected or appropriately treated, they can induce serious complications with reproductive health complications in women, including pelvic inflammatory disease, chronic pelvic pain, infertility, first-trimester abortion, and ectopic pregnancy.[6] Uncommonly, the disseminated gonococcal infection will manifest as septic arthritis or endocarditis. Gonorrheal infection can cause Fitz-Hugh-Curtis syndrome, liver capsule inflammation with resultant intra-abdominal adhesions, in women, and male infertility.
Complications specific to males include epididymitis, prostatitis, and proctitis.[1] Immune-mediated, systemic complications following gonorrhea infection can result in the triad of reactive arthritis, urethritis, and conjunctivitis.[1] Gonorrheal infection can complicate obstetrical delivery by infecting newborns via eye contact with genital secretions during the puerperal period and can result in gonococcal conjunctivitis that can progress to blindness. Gonorrheal infection increases the risk of sexual transmission of HIV-AIDS.[1][13]
The development of N. gonorrhoeae with antimicrobial resistance is a complication that has societal implications. Generally, the development of antimicrobial resistance corresponds to local, regional, and national antibiotic use; populations in countries such as Holland with lower utilization of cephalosporins, macrolides, and fluoroquinolones have a lower incidence of gonococcal resistance than high antibiotic consumption nations.[18]
Consultations
When treating individuals with suspected or confirmed cephalosporin resistance, clinicians are recommended to consult an infectious disease consultant and report treatment failure to the Centers for Disease Control within 24 hours of laboratory culture confirmation of the diagnosis of antimicrobial-resistant N. gonorrhoeae.[18]
Deterrence and Patient Education
Public health control of gonorrhea depends upon suitable antimicrobial therapy in tandem with generalized and targeted prevention interventions, accurate diagnostic assays, partner notification procedures, and epidemiological surveillance. Antibiotic administration should resolve individual cases to decrease the risk of complications and avert further transmission of the infection.[4]
Patients should abstain from sexual activity for at least one week following the initiation of antibiotic therapy. Patients should be counseled regarding the necessity to microbiologically confirm a cure of N. gonorrhoeae if they are treated with alternative therapy if significant comorbidities are present, including HIV, or if symptoms persist. Retesting can provide antibiotic susceptibilities that can avoid further treatment failure. Infected patients with gonorrhea are also at increased risk of contracting other STIs, including HIV. Up to 27% of patients diagnosed with HIV have a diagnosis of gonorrhea within 12 months of HIV diagnosis.[19]
Enhancing Healthcare Team Outcomes
The Centers for Disease Control and Prevention advocates for screening pregnant women and women with STI risk factors for N. gonorrhoeae infection. STI risk factors include prior STI diagnoses, non-Latino African American ethnicity, young age, sparse condom use, and multitudinous sexual partners.[16]
An interprofessional team of clinicians, epidemiologists, infectious disease specialists, community health nurses, and pharmacists (preferably with infectious disease specialization) can improve patient outcomes. Patients need to be taught preventative measures, and management of recent sex partners (i.e., < 60 days) is also a crucial element in preventing community spread. Nurses and mental health professionals are key players in this type of counseling. Pharmacists will be able to verify dosing and should have knowledge of the latest antimicrobial resistance data and can share that with the clinical staff, in addition to performing medication reconciliation. All interprofessional team members should keep accurate and updated records; these are crucial in the event of drug-resistant infections. The interprofessional approach will help drive the best outcomes with the fewest adverse events. [Level 5]