Continuing Education Activity
Congenital lobar emphysema is a rare developmental anomaly of lungs that occurs mostly due to defective bronchial cartilages. It is diagnosed with a chest x-ray or ct-scan and treated with lobectomy in severe symptomatic cases. This activity describes the histopathology, etiology, evaluation, and management of congenital lobar emphysema and highlights the role of the interprofessional team in improving care for patients with this condition.
Objectives:
- Describe the etiology of congenital lobar emphysema.
- Summarize the histopathology of congenital lobar emphysema.
- Outline the management options available for congenital lobar emphysema.
Introduction
Congenital lung diseases are rare but exceptionally distinct in their presentation ranging from large masses requiring immediate surgical intervention to small and asymptomatic lesions. The effects of congenital lung malformation can be critical; thus, a knowledge of the diagnosis and treatment of these abnormalities is essential. Lung development and anatomy are key fundamentals in consideration of these malformations and helps in the comprehension of the pathophysiology of each disease.
Congenital lobar emphysema (CLE) is a rare developmental malformation of the lung with a wide range of presentations, which poses a diagnostic and therapeutic dilemma and associated with high morbidity and mortality. CLE is characterized by respiratory distress due to overexpansion of one or more pulmonary lobes of the histologically normal lung without the destruction of alveolar walls with compression of surrounding lung parenchyma; that is why it is also called congenital lung overinflation. There is air trapping in the lung during the expiratory phase of respiration due to deficient bronchial cartilage, which causes repeated episodes of respiratory distress. The affected lobe is essentially non-functional because of overdistention and air trapping. It is frequently recognized in newborns; however, a few cases do not get evident until adulthood. This disease is potentially reversible if diagnosed and treated on time.[1]
Etiology
The etiology of congenital lobar emphysema in not known in 50% of the patients. In 25% of the patients, there is an absence of bronchial cartilage, hypoplasia, or dysplasia. Due to absent or defective cartilage, there is bronchial collapse and thus air trapping during expiration. The congenital lobar emphysema could be due to:
- Idiopathic in 50% of the cases.
- Absence of bronchial cartilage, hypoplasia, or dysplasia in 25% of patients
- Parenchymal diseases.
- External bronchial obstruction.
- Internal bronchial obstruction.[1]
Congenital lobar emphysema could be due to parenchymal disease like a poly-alveolar lobe. A poly-alveolar lobe theory for the etiology of congenital lobar emphysema proposed that there could be a 3- to 5-fold increase in the number of alveoli in the affected lobes of the lung compared to normal lobes. The reason behind air trapping in poly-alveolar lobes is not known.[2] Congenital lobar emphysema could also be due to internal bronchial disease. The bronchial disease can be stenosis, atresia, or bronchomalacia.[3][4] Diseases originating from structures adjoining lungs or bronchi such as vessels, mediastinal masses may also cause congenital lobar emphysema.[5]
Epidemiology
The incidence of CLE among live births is 1 out of 20,000-30,000. The occurrence is more in males than females with a ratio of 3 to 1. CLE is more common in infants and is extremely rare among adults. Thirty-three percent of the cases are symptomatic at birth. Due to the severity of symptoms, most are diagnosed within the first six months of birth. The left upper lobe is most commonly involved (43%), followed by the right middle lobe (32%) and right upper lobe (21%) involvement. The involvement of the lower lobe is as rare as only 2% of the cases.[1] A quarter of the cases are caused due to deformity of bronchial cartilages and another quarter due to obstruction of bronchi. CLE is also associated with anomalies of other systems, especially cardiac in up to 20 percent of the cases.[6]
Histopathology
Histologically, there is no tissue destruction observed, such as in acquired emphysema. There is no destruction of alveolar walls and alveolar septum, normal acinus structure, but no acinar maturation with age and overinflated alveoli. Congenital lobar emphysema has two forms:
- Hypo-alveolar
- Poly-alveolar
In the great number of CLE cases, there are normal numbers of radial alveoli. Nonetheless, there is no remarkable progression with age as to normal individuals inferring that acinar development in the concerned lung ends in the postpartum period. In hypo-alveolar, there are fewer than the expected number of alveoli, and in poly-alveolar, there are greater than the expected number of alveoli.[2] The airways and arteries are normal for normal in number, size, and structure.
History and Physical
Almost 50% of the patients are symptomatic at birth and another 50% present within the first six months of life. The patient usually presents with difficulty in feeding and breathing, wheezing, retractions, and cyanosis. There is typically a history of chronic cough and recurrent respiratory infections. Due to overlapping symptoms, some patients are wrongly diagnosed with pneumonia or pneumothorax instead of congenital lobar emphysema.[3] Lobes affected with CLE are overinflated; thus, there is impaired ventilation and perfusion. Due to progressive overinflation, there is compression of adjacent organs leading to further impairment of ventilation/perfusion and, ultimately, respiratory failure.
On physical examination, there is usually wheezing and rhonchi. The affected lobe is hyper-resonant on percussion, and breath sounds are diminished in the area. Congenital cardiac defects are usually associated with congenital lobar emphysema.[7]
Evaluation
Patients with congenital lobar emphysema develop air-trapping and hyperinflation in the affected lobes, but they are poorly perfused. It is vital for pediatric as well as adult radiologists to be familiar with radiological features of congenital lobar emphysema to maximize diagnostic accuracy. Patients with congenital lobar emphysema could even be diagnosed prenatally. The lungs of a fetus affected with congenital lobar emphysema show hyper-echogenicity without abnormal blood flow. This may also be accompanied by polyhydramnios or mediastinal shift. Magnetic resonance imaging is also safe to use prenatally to confirm the diagnosis.[8][9]
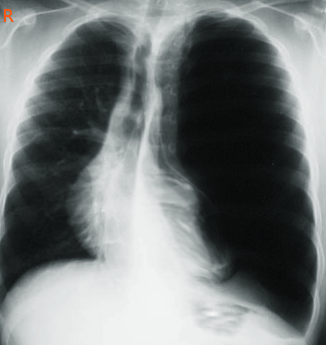
A chest x-ray is the first examination of choice in patients with respiratory distress. The affected lobe shows overinflation and hyperlucency in the case of congenital lobar emphysema. Computed tomography (CT) of lungs is the gold standard for the diagnosis of congenital lobar emphysema. It helps in the evaluation of the affected lobe as well as surrounding structures. CT-scan of the chest with IV contrast can help evaluate the vascular anomalies related to CLE.[10]To determine if lobectomy should be used as the treatment for congenital lobar emphysema, a single-photon emission tomography combined with computed tomography could be used to assess the relationship of perfusion to ventilation in affected lobes.
High clinical suspicion for congenital lobar emphysema should be present too to be able to diagnose the patients presenting with symptoms.
Treatment / Management
Clinical severity of patients with congenital lobar emphysema defines the treatment of choice. Apart from a few asymptomatic patients, almost half of the patients show symptoms within the first month of birth. Patients with mild or moderate symptoms could be treated conservatively. In case of severe symptoms, lobectomy is the gold standard for the treatment. However, the conservative treatment seems to be increasing as a result of antenatal diagnosis and intrauterine regression.[11][12]
Differential Diagnosis
Congenital lobar emphysema should be differentiated from:
- Congenital cystic adenomatoid malformation. Congenital lobar emphysema and congenital cystic adenomatoid malformation type III have similar findings on ultrasound, which shows a highly echogenic mass. Congenital lobar emphysema is devoid of cystic lesions as compared with cystic adenomatoid malformation.[13]
- Pneumonia. Patients with pneumonia present with fever, chest retractions, and cyanosis. The affected lung on chest x-ray may present with collapse consolidation, and it usually improves with antibiotics, unlike congenital lobar emphysema, the affected lung in pneumonia is not hyperinflated.[11]
- Tension Pneumothorax. Like congenital lobar emphysema, patients with tension pneumothorax also presents with respiratory distress, the physical examination will reveal hyperresonance and decreased breath sounds on the affected lung, and the chest x-ray will show that the mediastinum deviates to the contralateral lung. Tension pneumothorax is a medical emergency, and patients have hypotension, and it needs prompt decompression. The chest x-ray of the affected lung in tension pneumothorax shows depression of the hemidiaphragm, which is not seen in congenital lobar emphysema.[14]
- Congenital diaphragmatic hernia. Congenital lobar emphysema and congenital diaphragmatic hernia present with hyperlucent lung on chest x-ray. It can be differentiated with congenital lobar emphysema because of the gas-filled loops of bowel in the chest.[15]
Prognosis
- In mild and moderate cases, non-surgical conservative management has good results.
- In patients with severe symptoms, lobectomy has an excellent prognosis, and mortality with surgery is very low.[16]
Complications
Congenital Lobar emphysema can have the following complications:
- Cyanosis
- Respiratory failure
- Surgical complications due to lobectomy
- Infantile death
Consultations
Patients may require to consult these specialties for appropriate diagnosis and treatment:
- Primary care physician
- Radiologists
- Pediatrician
- Thoracic surgeon
Deterrence and Patient Education
Patients with congenital lobar emphysema can present differently. The usual presentation is respiratory distress, wheezing, cyanosis, and difficulty in feeding. The parents of the newly diagnosed patient should be given emotional support and detailed information about the condition, its treatment, prognosis, and effects on everyday life.
Asymptomatic patient: If the patient is asymptomatic, the parents should be guided about conservative management. There should be regular follow-up and observation, and the parents should be advised of the steps that should be taken if the patient starts to show symptoms.
Symptomatic patient: If the patient has severe symptoms, parents should be guided about the possibility of surgery (lobectomy) as well as its prognosis and lifestyle changes accordingly. The parents should be provided with educational material about the disease. Flow charts, diagrams, and videos should be used to explain each and every aspect of the disease, treatment, and lifestyle changes until the parents fully understand everything and are satisfied with the provision of care.
Pearls and Other Issues
Here are some important points to remember:
- Congenital lobar emphysema is a rare developmental malformation of lungs.
- The main etiology is the deficient development of bronchial cartilages leading to overinflation of the affected lobe.
- CLE usually presents with respiratory distress, wheezing, rhonchi, cyanosis, and difficulty in feeding.
- Chest x-ray and CT-scan are used for diagnosis.
- The best treatment in severe cases is lobectomy.
- Congenital lobar emphysema usually has a good prognosis even in patients with severe symptoms after lobectomy.
Enhancing Healthcare Team Outcomes
It is the responsibility of healthcare professionals that the parents of the patient have a good understanding of the disease and the appropriate treatment available for the disease. The diagnosis of congenital lobar emphysema in the newborn is usually distressing and can cause significant anxiety. Healthcare providers need to provide emotional support to the parents of the newly diagnosed patient.
The therapeutic approach to congenital lobar emphysema should utilize an interprofessional team, including primary care physician, pediatrician, physician assistant, nurse practitioner, radiologist, and thoracic surgeon to establish a definitive diagnosis and provide appropriate treatment. If the patient has mild or moderate symptoms, treatment is conservative. Primary care providers or pediatricians can closely monitor patients who are asymptomatic and have no local or systemic manifestations. Patients with serious manifestations such as respiratory failure and cyanosis should be referred to a thoracic surgeon for lobectomy.