Introduction
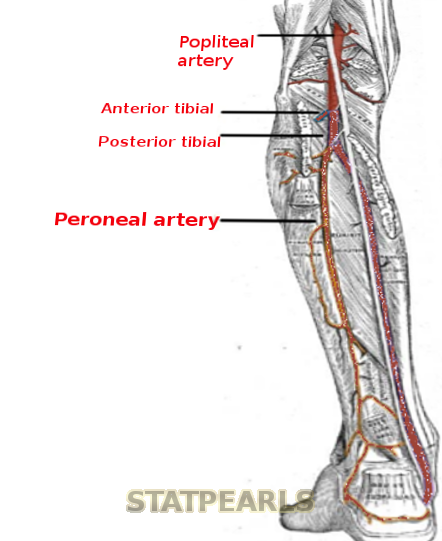
The peroneal artery (also termed the fibular artery) is the posterior lateral branch of the tibial-peroneal trunk in the lower extremity just distal to the popliteal fossa. The peroneal artery (along with the anterior tibial artery) is the vascular supply to the lateral compartment of the lower leg. The three arteries of the lower leg are the peroneal artery, anterior tibial artery, and posterior tibial artery (the proximal aspect of the posterior artery is also know as the tibial-peroneal trunk).
Structure and Function
Although there are many anatomical variations, the most common configuration of the popliteal artery is with the first branch being the anterior tibial artery. Then after the first branch point, the popliteal artery becomes the posterior tibial artery (also known as the tibioperoneal trunk or the tibiofibular trunk). The posterior tibial artery (tibioperoneal trunk) then bifurcates into a posterior tibial and a peroneal artery.
The peroneal artery originates from the posterior tibial artery (tibioperoneal trunk) roughly 2 to 3 cm distal to the popliteal fossa. The peroneal artery is usually the posterior lateral branch of the posterior tibial artery (tibioperoneal trunk). The peroneal artery then courses towards the fibular bone and descends down the lower leg along the posterior surface of the interosseus membrane between the fibula and tibia. The peroneal artery is located at the posterior aspect of the intermuscular septum of the lateral compartment between tibialis posterior and flexor hallucis longus muscles or within flexor hallucis longus muscle belly in the posterior compartment.[1]
The peroneal artery descends to the level of the ankle at the inferior tibiofibular syndesmosis where it divides into the calcaneal arterial branches at the posterior lateral aspect of the calcaneus. Distally the peroneal artery is contiguous with the dorsal artery of the foot, the lateral tarsal artery, the lateral malleolar artery, and the lateral plantar arteries.
The distal peroneal artery gives off a communicating branch which anastomosis with the communicating branch of the posterior tibial artery. The distal peroneal artery also has anterior branches that anastomosis with the distal anterior tibial artery. Arterial anastomosis provides collateral circulation in the hindfoot and ankle.
Inferiorly, through perforating branches, the peroneal artery penetrates the posterior intermuscular septum of the lateral compartment (also known as the peroneal compartment) to supply the peroneus brevis and peroneus longus muscles with blood flow. Superiorly, the anterior tibial artery penetrates the anterior intermuscular septum of the lateral compartment to supply the peroneus brevis and peroneus longus muscles with blood flow.[1]
The lateral compartment of the leg is one of the four compartments in the lower leg. The four compartments of the lower leg are the lateral, anterior, superficial posterior, and deep posterior compartments. Muscles residing in the lateral compartment of the leg function to cause foot eversion. The anterior boundary of the lateral compartment is the anterior intermuscular septum. The posterior boundary of the lateral compartment is the posterior intermuscular septum. Medial and lateral boundaries of the lateral compartment are the fibular surface and deep leg fascia, respectively.[2]
Embryology
Smooth muscle of the peroneal artery and all large arteries derive from lateral plate mesoderm and neural crest cells. In general blood vessels are formed by two basic methods: 1) by vasculogenesis, where blood vessels form by the combination/ uniting of angioblasts and 2) by angiogenesis, where new vessels are formed by branching off from parent (proximal) blood vessels.[2]
Blood Supply and Lymphatics
There is a peroneal vein in the posterior lateral aspect of the lower leg that has a course similar to the peroneal artery. The peroneal vein drains into the popliteal vein. The superficial veins of the lateral leg drain into the small saphenous vein. The deep veins of the lateral leg drain into the posterior tibial vein.
Superficial lymphatics provide lymphatic drainage to the lateral compartment of the lower leg.[1]
Muscles
The peroneal artery supplies the muscles of the lateral compartment of the lower leg. The peroneus brevis and peroneus longus muscles are the only two muscles of the lateral compartment.[1]
Physiologic Variants
The peroneal magnus artery is a congenital vascular variant of the lower leg. In patients with a peroneal magnus artery, the anterior and posterior tibial arteries are smaller than normal, and the peroneal magnus artery is larger than normal peroneal arteries. The peroneal magnus artery provides the majority of blood supply to the lower leg and foot. A peroneal magnus artery is seen in up to 5% of the population.[1]
Patients with a peroneal magnus artery that undergo vascular surgery involving grafting in the lower leg have an increased likelihood of experiencing surgical complications such as foot and limb ischemia.
Clinical Significance
Peripheral arterial disease (PAD), caused by atherosclerosis, is the primary clinical issue associated with the peroneal artery. Mild cases of PAD correlate with mild leg pain with exertion (for example – walking). The term for pain with exertion is claudication. Moderate cases of PAD demonstrate severe pain with walking, and severe PAD presents with leg pain at rest.[3]
Radiographic evaluation of PAD can be performed with multiple different modalities. Plain radiographs (x-rays) can diagnosis atherosclerosis by identifying vascular calcifications. However, plain radiographs are not considered to be a suitable method of evaluating for PAD due to the very low sensitivity that x-rays have in being able to identify atherosclerosis when present.
Vascular ultrasound enjoys extensive use in the evaluation of PAD. Vascular ultrasound is often the first step in the evaluation of patients with symptoms of claudication. Atherosclerosis of lower extremity arteries can be identified with ultrasound with good sensitivity. Vascular ultrasound is a non-invasive method of evaluating the lower extremity arteries. Another non-invasive radiographic evaluation of PAD is CT angiography (CTA). MR angiography (MRA) is also a non-invasive radiographic modality to evaluate for PAD.[4]
Vascular ultrasound, CTA, and MRA allow for the evaluation of arterial stenosis, occlusion, as well as evaluation of abnormal collateral circulation in the lower extremities. The presence of abnormal collateral circulation indicates the presence of longstanding significant atherosclerotic disease.
Digital subtraction angiography (DSA) is an invasive radiographic modality that can evaluate for PAD and has high specificity. Digital subtraction angiography requires intravenous contrast to be injected into the arterial system to evaluate for stenosis, occlusion, and abnormal collateral circulation.
Digital subtraction angiography also allows for therapeutic intervention to be performed in addition to diagnosis (unlike vascular ultrasound, CTA, and MRA which are diagnostic only). Arterial balloon angioplasty with stenting of areas of stenosis caused by atherosclerosis can be performed as a treatment for PAD at the same time as diagnostic DSA analysis.[5]