Continuing Education Activity
Keratoconjunctivitis refers to an inflammatory process that involves both the conjunctiva and the superficial cornea. It can occur in association with viral, bacterial, autoimmune, toxic, and allergic etiologies. This activity outlines the presentation, evaluation, and treatment of keratoconjunctivitis. Additionally, it explores the role of the interprofessional team involved in the management of patients with keratoconjunctivitis.
Objectives:
- Describe the many etiologies of keratoconjunctivitis.
- Describe the typical presentation of keratoconjunctivitis.
- Identify the appropriate treatment(s) of keratoconjunctivitis.
- Explain the importance of improving care coordination amongst interprofessional team members to improve outcomes for patients with keratoconjunctivitis.
Introduction
The conjunctiva is a transparent, thin, mucous membrane that covers the sclera. It extends from the limbus (the perimeter of the cornea) and covers both the sclera (known as bulbar conjunctiva) and posterior surface of the eyelids (known as palpebral conjunctiva). Keratoconjunctivitis refers to an inflammatory process that involves both the conjunctiva – conjunctivitis – and the superficial cornea – keratitis – which can occur in association with viral, bacterial, autoimmune, toxic, and allergic etiologies.[1] While there is an expansive list of causes of conjunctivitis and keratitis, this review will focus on more well-known entities causing combined keratoconjunctivitis. Specifically, this article will discuss the entities known as epidemic keratoconjunctivitis, vernal keratoconjunctivitis, superior limbic keratoconjunctivitis, and keratoconjunctivitis sicca.
Etiology
The list of causes of keratoconjunctivitis is extensive. A general classification scheme is helpful, dividing cases into infectious and non-infectious causes. Under the infectious category, viral and bacterial etiologies are by far the most common, with viral infection accounting for the majority of all-comers suspected of an infectious etiology. Non-infectious keratoconjunctivitis can be allergic, toxic, or immune-mediated. It is often also useful to further divide keratoconjunctivitis into unilateral or bilateral, and hyperacute (onset less than 1 week), acute (onset under 3 to 4 weeks) or chronic (lasting longer than 4 weeks).[2]
Epidemic keratoconjunctivitis (EKC)– viral keratoconjunctivitis caused by the adenovirus, a ubiquitous, nonenveloped, double-stranded DNA virus. The primary targets of human adenovirus are the eyes, respiratory tract, gastrointestinal tract, and genitourinary tract. Research ash found human adenovirus types 8, 19, 37, and 54 as the strains responsible for outbreaks of epidemic keratoconjunctivitis.[3]
Vernal Keratoconjunctivitis (VKC)– Severe allergic conjunctivitis for which the exact etiology is still unclear. Suspicions are that there is a strong allergic component as the immunoglobulin E (IgE) mast cell-mediated pathway plays an important role in symptomatology. The theory is that there is a combination of immune system, genetic, and environmental factors (including air pollutants/allergens).[4]
Superior limbic keratoconjunctivitis (SLK)– Chronic inflammatory condition, though the etiology is unknown. One leading theory suggests that the inciting component to the development of superior limbic keratoconjunctivitis is constant friction between the superior bulbar and tarsal conjunctival interfaces causing chronic microtrauma.[5]
Keratoconjunctivitis sicca – Also colloquial known as dry eye syndrome (DES), various underlying etiologies have been identified as well as associations with several, primarily autoimmune, systemic conditions. Regardless, the final common pathway is shown to be abnormalities in the pre-corneal tear film and lymphocyte-mediated inflammatory changes in the ocular surface, including conjunctiva and cornea.
Epidemiology
The prevalence of keratoconjunctivitis varies widely according to the underlying cause, which is also influenced by age, environment, and genetics. Some estimates suggest as many as 6 million people annually in the United States present to a healthcare provider with signs and symptoms of conjunctivitis or keratoconjunctivitis.
Of all patients presenting with conjunctivitis or keratoconjunctivitis, allergic causes account for the majority of cases, affecting up to 40% of the population. Under the umbrella of allergic etiology, VKC most often occurs in school-aged children, with a peak incidence at ages 4 to 7 years old. It should be noted, however, that it can present as early as 5 months or as late as the third or fourth decades of life. There is a predilection for young males who reside in a dry and hot climate; especially in West Africa, the Mediterranean basin, Middle East, India, and South America. It is less common in North America and Western Europe.[6][7]
Among infectious etiologies, bacterial conjunctivitis is more common in the pediatric population and may be responsible for approximately 50% of cases. Viral is by far the most common despite the patient's age, with estimates of up to 75%. The majority of viral infections – up to 90% - are secondary to adenovirus; other viral agents include enterovirus, herpes simplex, and herpes zoster.[1][8]
Keratoconjunctivitis sicca has been identified as a growing public health concern, as it affects as many as 17% of women and 11% of men in the United States. Some studies suggest this is a gross underestimate as many patients will self-treat without seeing a healthcare provider. These rates are much higher in subgroups of patients who also carry autoimmune diagnoses such as Sjogren syndrome, rheumatoid arthritis, systemic lupus erythematosus, sarcoidosis, and scleroderma, among others. Prevalence of disease also increases in dry climates.[9]
Superior limbic keratoconjunctivitis is a relatively rare condition with a female to male predominance of approximately 3 to 1. Age of presentation ranges from 20 to 60 years of age. There is no documentation of a racial predilection. There is an association with thyroid dysfunction as well as keratoconjunctivitis sicca.[5]
History and Physical
Symptoms common to keratoconjunctivitis, regardless of etiology, include eye discomfort/irritation, pruritis, light sensitivity, minor blurring of vision (often intermittent), epiphora. Common signs include conjunctival injection, conjunctival chemosis, and eye discharge. Examiners should query all patients about contact lens wear, any possible exposures, i.e., sick contacts, chemical exposure, current eye drops or face creams, recent activities that may have resulted in a foreign body or corneal abrasion, etc. Additionally, a time-course regarding their symptoms is necessary, as well as any relieving or exacerbating factors. Systemic conditions, including autoimmune conditions, atopy, and thyroid disease, should be discerned during the historical investigation.
Viral keratoconjunctivitis often presents initially with unilateral involvement, that later spreads to the contralateral eye and will often have asymmetric findings. Patients present with ocular discomfort/itching and often marked light sensitivity. Conjunctival injection and chemosis are common as well as a primarily watery discharge. The palpebral conjunctiva will frequently show a follicular reaction, as well as petechial hemorrhages and formation of pseudomembranes, are not uncommon. Lymphadenopathy and/or an antecedent upper respiratory illness are present in up to 50% of cases and known contact with other affected individuals is common, but not mandatory. Signs and symptoms may last as long as 7 to 21 days, and patients may remain infectious for 10 to 14 days.[8][3]
Vernal keratoconjunctivitis presents with bilateral pruritis, foreign body sensation, photophobia, mucous discharge, epiphora, and conjunctival injection. Symptoms can range from mild to severe, in some cases preventing patients from performing daily activities. Early morning mucoid discharge with stickiness of the lids is characteristic. Classically, the upper palpebral conjunctiva will show a papillary reaction from epithelial hyperplasia with a fibrovascular core. If many, large papillae are present, there may be a cobblestone appearance. Papillae may also appear in the limbal region, and when topped with chalky-white excrescences are termed Horner-Trantas spots. Corneal signs include punctate epithelial erosions and keratitis, but microerosions can accumulate into a characteristic macro-erosion termed a shield ulcer. Though termed “vernal,” approximately one-fourth of cases are symptomatic year-round, and up to 60% will have recurrences during the winter months.[6][7][10]
Keratoconjunctivitis sicca presents with chronic, but often intermittent, bilateral (though often asymmetric) burning, stinging, foreign body sensation, and photophobia. Other symptoms include eye fatigue, a sense of heavy eyelids, pruritis, epiphora, watery discharge, and blurred vision. Reading, computer use, television or other electronic use, or driving when the natural blink reflex is decreased often makes the intermittent blurring of vision worse. Exam findings include conjunctival injection, inspissated meibomian glands, eyelid margin telangiectasias, and erythema, decreased tear lake, rapid tear break-up time, punctate epithelial erosions, and reduced tear production.[9][11]
Superior limbic keratoconjunctivitis displays bilateral burning, irritation, foreign body sensation. Symptoms are typically chronic with gradual clearing but may have periods of remission. Asymmetric involvement is not uncommon. Characteristic exam findings include watery discharge and epiphora, superior palpebral and bulbar conjunctival injection and chemosis. A conjunctival papillary reaction may be present as well as redundant conjunctiva or conjunctivochalasis. Punctate epithelial erosions involving the upper third of the cornea are often present. In chronic or severe disease, conjunctival overgrowth or pannus may be present on the cornea.[5]
Evaluation
Irrespective of underlying etiology, evaluation should include the following components:
- Assessment of best-corrected visual acuity
- Pupillary reactions
- Extraocular motility
- Confrontational visual fields
- Intraocular pressure
- External exam including assessment of preauricular lymph nodes and periorbital signs of erythema or edema
- Eyelid examination for hyperpigmentation, erythema, edema, rash/vesicles, discharge
- Discharge should be categorized as purulent, mucopurulent, mucoid, or watery – purulent discharge can reform as soon as it is cleared from the eye; mucoid discharge adheres to the eyelashes and appears sticky; watery discharge is clear and copious – if a purulent discharge is found, a culture should be sent
- Eversion of the eyelids to examine the palpebral conjunctiva, especially to evaluate for the presence of follicles, papillae, or pseudomembranes
- Examination of the bulbar and forniceal conjunctiva for injection and chemosis as well as the geographic pattern of injection
- Fluorescein staining and subsequent examination with either a Wood lamp or slit-lamp microscope or direct ophthalmoscope utilizing a cobalt blue filter to evaluate for presence and pattern of corneal abrasions, microtrauma, or epithelial defects; if a herpetic infection is suspected, particular attention to identifying dendritic/pseudodendritic lesions is necessary. More specific testing can be considered depending on underlying etiology suspicion[12]:
- Schirmer testing can evaluate tear production in suspected cases of keratoconjunctivitis sicca
- Corneal sensation testing is an option in cases of suspected herpetic viral infection which can cause decreased corneal sensitivity
- Tear osmolarity has been increasing in popularity and shows elevated tear film osmolarity in patients with keratoconjunctivitis sicca
- Rapid sequence adenoviral testing is available in cases of suspected epidemic keratoconjunctivitis, however, most commonly this is a clinical diagnosis
- If keratoconjunctivitis sicca is suspected, the provider might consider initial testing for Sjogren syndrome by serum antibody testing of SS-A (anti-Ro) and SS-B (anti-La)
Treatment / Management
Management largely depends on underlying etiology as follows:
Epidemic Keratoconjunctivitis – viral infection is extremely contagious, and a focus should be on preventing spread to others. Spread occurs through direct contact of contaminated fingers, household objects, or medical instruments. Diligent hand washing and cleansing of household and/or medical office equipment are paramount in preventing transmission. Estimates of incubation and contagious periods are 5 to 12 days and 10 to 14 days, respectively. This prolonged recovery period should also be emphasized with patients and parents of patients to prevent concern over persistent symptoms and prevent unnecessary return healthcare visits.[13] No effective treatment exists, however symptomatic treatment with artificial tears, cool compresses, and in some cases, topical antihistamines have been shown to be effective. Some in-vitro studies using topical ganciclovir and cidofovir have shown potential in future treatment.[14]
Vernal Keratoconjunctivitis – Often, a multi-disciplinary approach is required, including referral to ophthalmology. Treatment should focus on a balance of relieving symptoms and avoiding medication/treatment side effects. First-line treatment options are lubricating treatments for the ocular surface, e.g., preservative-free artificial tears, gels, or ointments. These are often inadequate in isolation but have an essentially non-existent side effect profile. Additionally, cool compresses and lid scrubs should be prescribed to attempt removal of any possible allergens. Subsequent treatment with topical antihistamines may be adequate in mild cases. Topical mast cell stabilizers are often added to topical antihistamines and can control symptoms in moderate cases. It is worth noting that mast-cell stabilizers (cromolyn sodium nedocromil sodium, and lodoxamide) have loading periods to reach a therapeutic effect. If a seasonal variation is noted, mast cell stabilizers can be initiated before symptoms in anticipation of the seasonal recurrence. Combination antihistamines/mast cell stabilizers are available such as olopatadine, azelastine, and ketotifen. Systemic antihistamines can be used; however, there is little evidence for their use in keratoconjunctivitis and side-effect profiles must be considered before initiation. Topical non-steroidals can be trialed, though are often found to be poorly effective. Topical corticosteroids are typically the most effective in a high initial dose with a quick tapering method. Though topical corticosteroids carry a low systemic side-effect profile, it is imperative to monitor for ocular side-effects including elevation of intraocular pressure. With severe, persistent cases, long-term immunomodulation with steroid-sparing agents, such as cyclosporine and tacrolimus, has been shown to be helpful.[15][16][6][7][17]
Keratoconjunctivitis sicca – Initial management is typically conservative, including preservative-free artificial tears, gels, and ointments. Warm compresses and lid scrubs can be utilized to increase oil production/release from meibomian glands, which help to stabilize the tear film. Oral flaxseed oil and fish oil supplements have been shown to be useful in alleviating symptoms and decreasing dependence on topical treatments. Procedural treatment by way of insertion of punctal plugs to prevent lacrimal drainage of the tear film is available. More permanent punctal treatment by cautery is also sometimes performed. Topical cyclosporine A, tacrolimus, and lifitegrast are available by prescription and work as steroid-sparing inflammatory dampening agents. Topical steroids are also useful, though preferably in short courses, and monitoring of intraocular pressure is mandatory. Oral doxycycline in low doses has been shown to have a benefit via its unique anti-inflammatory properties. More recently, topical autologous serum drops have increased in popularity. Serum drops contain anti-inflammatory factors that inhibit mediators of the dry eye inflammatory cascade. These serum drops can be prohibitively expensive. Typically, a combination of the above treatment options is needed to provide adequate symptomatic relief.[9]
Superior limbic keratoconjunctivitis – First-line treatment is conservative with preservative-free artificial tears, gels, and ointments. Other topical treatments utilized with varying degrees of success include mast-cell stabilizers, anti-histamines, vitamin A, and non-steroidal anti-inflammatories. Punctal occlusion techniques can also help to increase ocular surface lubrication. Topical autologous serum eye drops have also been found to be effective, though long-term treatment is often necessary and cost of medication is commonly a barrier. Chemocautery of affected conjunctiva by silver nitrate often results in symptomatic relief for 1 to 2 months, but generally requires re-treatment. Surgical conjunctival resection of the affected/redundant conjunctiva is thought to be a highly effective treatment. Alternatively, liquid nitrogen cryotherapy can be used to treat affected conjunctiva and generally results in long-term symptomatic relief, though repeat treatments may be necessary.[5][18][19][20]
Differential Diagnosis
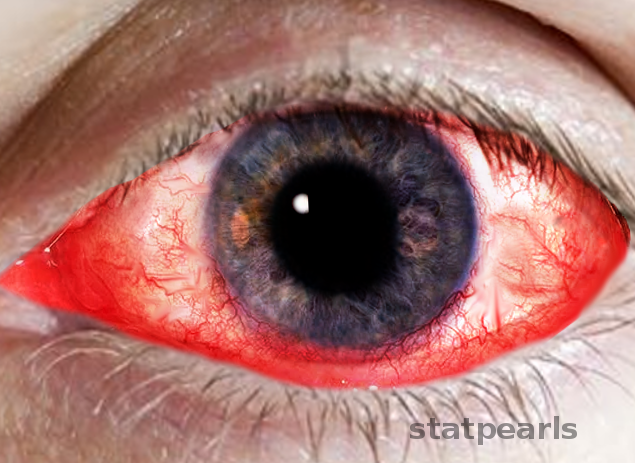
Patients with keratoconjunctivitis typically present with a red, irritated eye. Therefore a differential diagnosis should include:
- Conjunctivitis (bacterial, fungal, viral, chemical, exposure, toxic)
- Episcleritis/scleritis
- Uveitis/Iritis
- Endophthalmitis
- Corneal abrasion/ulcer
- Corneal foreign body
- Acute angle closure glaucoma
- Subconjunctival hemorrhage
Urgent conditions to consider from the above list include acute angle closure glaucoma, endophthalmitis, corneal ulcer, corneal foreign body, and uveitis/iritis. Concern for any of these conditions should prompt referral to ophthalmology. Other signs/symptoms that might trigger ophthalmology referral include:
- History of foreign body/trauma
- Elevated intraocular pressure
- An asymmetric/nonreactive pupil
- Marked loss in visual acuity
- Extensive/debilitating pain including an inability to open eye or keep the eye open
- Corneal opacity
- Copious or hyperacute and progressive purulent discharge
Prognosis
Viral keratoconjunctivitis or epidemic keratoconjunctivitis is a self-limiting disease. However, it can take 2 to 3 weeks for resolution. Recurrence is possible by acquiring subsequent viral infections; however, long-term complications are rare.
Similarly, vernal keratoconjunctivitis is typically a benign and self-limiting disease that often resolves spontaneously with age, particularly at the peri-pubescent period. If symptoms persist beyond childhood and adolescence, which can occur in as many as 12% of patients, then it is considered conversion to atopic keratoconjunctivitis which has a similar symptomatic, diagnostic, and treatment profile but requires chronic treatment.[7]
Keratoconjunctivitis sicca has a broad spectrum of disease severity. In most patients, symptomatic control is possible by adherence to a regular treatment regimen; this does not represent a “cure,” however symptoms can be well-controlled. Changes in the environment (climate, geographic, or air pollutant changes) can also lead to a resolution of symptoms. It is not uncommon, though, for well-controlled patients to have break-through episodes requiring a brief step-up in treatment methodology.
Treatment of superior limbic conjunctivitis usually is very successful. In cases that are not responsive or symptomatically managed with conservative treatments, then more aggressive treatments such as chemo-‘cautery or surgical conjunctival resection are quite successful.
Complications
Complications of keratoconjunctivitis occur from prolonged inflammation, persistent rubbing, and also from some treatment modalities. Though rare, prolonged inflammation of the conjunctiva and cornea can result in symblepharon, forniceal shortening, conjunctival scarring, limbal stem cell deficiency, corneal scarring. Prolonged and aggressive eye rubbing can result in acquired eyelid ptosis, early cataract formation, and also correlates with the development of keratoconus. Finally, the healthcare provider must be cognizant of medication side-effects. Topical corticosteroids carry a risk of increasing intraocular pressure leading to steroid-induced glaucoma, an irreversible and vision-threatening condition. Topical and systemic steroids also increase rates of early cataract formation. Topical corticosteroids can also predispose patients to ocular herpes simplex reactivation or allow significant progression of ocular herpetic or bacterial infection; thus, it is important for providers to rule-out herpetic and bacterial infections before initiating topical corticosteroid treatment.
Deterrence and Patient Education
Patients should receive counseling in all cases of the prolonged time course to symptomatic resolution. Even with strict adherence to a treatment regimen, immediate symptomatic relief is unusual. Purposeful discussion with patients or parents of patients regarding expectations may avoid unnecessary, time-consuming, and costly return visits to the primary care, urgent care, or emergency room setting. However, patients should also have specific counseling regarding warning signs; specifically, decrease in vision, worsening pain, increased photophobia, worsening discharge, or lack of response to therapy after 1 week of treatment.
Enhancing Healthcare Team Outcomes
Keratoconjunctivitis and conjunctivitis are extremely common causes of visits to primary care providers and nurse practitioners. Referral to an ophthalmologist for every case of red eye is unnecessary and burdensome to the patient both temporally and financially. Referral to ophthalmology should take place when any of the following develop: persistent/worsening disease states, vision loss, moderate to severe pain, severe purulent discharge, marked corneal involvement, conjunctival scarring, a concern of herpetic disease, lack of response to therapy. Special attention should is necessary for patients who wear contact lenses, may require treatment with steroids, or also present with severe photophobia.[21][22][23] [Level V]
Keratoconjunctivitis requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and pharmacists, all collaborating across disciplines to achieve optimal patient results. [Level V]