Continuing Education Activity
This CME activity provides healthcare professionals with the latest updates and advancements in diagnosing and managing abducens nerve palsy. Abducens nerve palsy, characterized by lateral rectus muscle weakness and restricted eye abduction, poses significant challenges in patient care. Through this activity, participants will understand the etiology, clinical presentation, diagnostic workup, and evidence-based management strategies for abducens nerve palsy. Key topics will include differentiating abducens nerve palsy from other causes of diplopia, interpreting neuroimaging findings, exploring nonsurgical and surgical treatment options, and addressing the importance of an interprofessional team approach in optimizing patient outcomes. By the end of this activity, participants will be equipped with the knowledge and skills to effectively diagnose and manage patients with abducens nerve palsy, improving their clinical practice and patient care.
Objectives:
Identify the clinical features and characteristic findings associated with abducens nerve palsy.
Screen patients presenting with diplopia for possible abducens nerve palsy and promptly refer them for further evaluation and management.
Apply evidence-based management strategies for abducens nerve palsy, including non-surgical and surgical interventions, considering the patient's age, overall health, and preferences.
Collaborate with a multidisciplinary team, including ophthalmologists, neurologists, neurosurgeons, and radiologists, to optimize the care and outcomes of patients with abducens nerve palsy.
Introduction
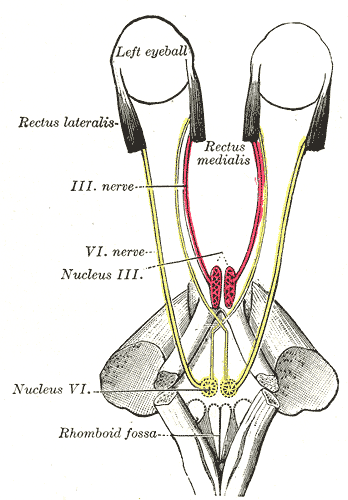
The abducens nerve, the sixth cranial nerve (CN VI), is responsible for ipsilateral eye abduction. Dysfunction of the abducens nerve can occur at any point of its transit from the pons to the lateral rectus muscle, resulting in sixth nerve palsy.[1] To understand the causes of this palsy, it is essential to understand the nerve's anatomy as it transverses the brain.
The abducens nerve originates in the pons, near the seventh cranial nerve. It then exits the brainstem and enters the subarachnoid space, following a path along the skull called the clivus. Continuing its journey, the nerve reaches the petrous apex of the temporal bone in the basal skull, where it enters the cavernous sinus.[2]
Within the cavernous sinus, the abducens nerve is positioned medially to the internal carotid artery, while the trigeminal nerve is located laterally. After passing through the cavernous sinus, the abducens nerve enters the orbit via the superior orbital fissure. Once in the orbit, it innervates the lateral rectus muscle responsible for eye abduction.[3][4][5]
Sixth cranial nerve palsy is the most common isolated palsy in adults and the second most common cranial nerve palsy in children. When diagnosing a case of sixth nerve palsy, the patient's age plays a critical role in determining the underlying cause and the need for further evaluation, including neurological imaging.[6]
In adults, the risk factors for abducens nerve palsy can be categorized as vasculopathic or non-vasculopathic. Vasculopathic risk factors are more common in older patients and may include conditions such as diabetes. On the other hand, non-vasculopathic causes can be present in adults and children and may involve various factors such as trauma, inflammation, or compression.
The most common risk factors for sixth nerve palsy in children include increased intracranial pressure, vascular anomalies, and neoplastic disorders. It is important to note that in children, after ruling out trauma, idiopathic causes, and postviral etiologies, neurological imaging is necessary to investigate the underlying cause further.[7]
Etiology
As mentioned previously, understanding the path of the abducens nerve is important in determining the etiology of abducens nerve palsy. Neoplasms and trauma can affect the abducens nerve at any point along its course and cause palsy. However, other causes of abducens nerve palsy can be categorized based on the location of the abducens nerve.[8][9][10]
Abducens nerve palsy can have nuclear and fascicular causes, which involve pathologies that directly affect the pons, where the nucleus and fascicles of the sixth nerve are located. Some examples of nuclear and fascicular causes include ischemic stroke, metabolic diseases such as Wernicke disease, and demyelinating lesions. These nuclear causes may be associated with facial nerve palsies due to the proximity of abducens and facial nerves in the pons.[11]
Additional etiologies may arise as the abducens nerve enters the subarachnoid space, leading to abducens nerve palsy. In these cases, the palsy is primarily caused by increased intracranial pressure. Other accompanying symptoms, such as headache, nausea, vomiting, and papilledema, may be observed. Several causes can contribute to abducens nerve palsy in this context. These include an aneurysm, carcinomatous meningitis, procedure-related injury (eg, spinal anesthesia, postlumbar puncture), inflammatory lesions (eg, sarcoid, lupus), and infection (eg, Lyme disease, syphilis, tuberculosis, Cryptococcus).[12]
Since the abducens nerve courses over the petrous apex, there are specific causes of abducens nerve palsy associated with this region. These causes include complicated otitis media or mastoiditis, sinus thrombosis, and basal skull fracture.[13]
As the abducens nerve traverses the cavernous sinus, the most common cause of palsy in this region is stretching or compression of the abducens nerve. These etiologies include cavernous sinus thrombosis, cavernous sinus fistula, and internal carotid aneurysm or dissection.[14]
Lastly, orbital lesions can also cause an abducens nerve palsy. These conditions include neoplasm, inflammatory disease, infection, or trauma.[15]
Table 1. Etiology of Sixth Nerve Palsy in Children
|
S. No
|
Etiology
|
Examples
|
|
1
|
Idiopathic
|
|
|
2
|
Trauma
|
Traumatic brain injury
Basal skull fracture
|
|
3
|
Tumor
|
Benign
Malignant
Metastasis
|
|
4
|
Iatrogenic
|
Birth injury
Vaccine-induced trauma
Neurological injury
|
|
5
|
Neurological Pathologies
|
Idiopathic intracranial hypertension
Migraine
Multiple sclerosis
|
|
6
|
Infections
|
Brain abscess
Herpes zoster virus
Epstein-Barr virus
Meningitis
Cytomegalo virus
Gradenigo syndrome
Lyme Disease
|
|
7
|
Vaculopathic disorders
|
Diabetes
Hypertension
Atherosclerosis
|
|
8
|
Miscellaneous
|
Intracranial aneurysms
Arteriovenous malformation
Arnold-Chiari malformation
Hydrocephalus
|
Table 2. Etiology of Sixth Nerve Palsy in Adults
|
S. No
|
Etiology
|
Example
|
|
1
|
Vasculopathic
|
Diabetes
Hypertension
Atherosclerosis
|
|
2
|
Traumatic
|
Basal skull fracture
Head trauma
Spinal fracture
|
|
3
|
Tumur
|
Benign
Metastatic
Malignant
|
|
4
|
Infectious
|
Fungal infection
Bacterial infections
Syphilis
Herpes zoster
Lymes disease
|
|
5
|
Hematologic
|
Leukaemia
Lymphoma
Interferon therapy
|
|
6
|
Neurological pathologies
|
Idiopathic intracranial hypertension
Multiple sclerosis
Cluster headache
Lithium toxicity
|
|
7
|
Systemic disorders
|
Systemic lupus erythematosus
Collagen vascular disorders
Sarcoidosis
Amyloidosis
|
|
8
|
Vascular intracranial pathologies
|
Aneurysms
Arteriovenous malformations
Giant cell arteritis
Carotid artery dissection
|
|
9
|
Iatrogenic
|
Neurosurgical trauma
Nerve block
Lumbar puncture
Myelography
Spinal anesthesia
|
Syndromes Associated with Sixth Cranial Nerve Palsy
- Brainstem syndromes
- Elevated intracranial pressure
- Petrous apex syndrome
- Cavernous sinus syndrome
- Orbital syndrome [2]
Brainstem Syndromes
- Raymond syndrome is characterized by abducens nerve palsy and contralateral hemiplegia (pyramidal tract involvement).[16]
- Millard-Gubler syndrome: In this syndrome, abducens nerve palsy (CN 6 involvement), ipsilateral facial nerve palsy (CN 7 involvement), and contralateral hemiplegia (pyramidal tract involvement) are observed.[17]
- Foville syndrome: This syndrome presents with abducens nerve palsy (CN 6), horizontal conjugate gaze paresis, ipsilateral Horner's syndrome and ipsilateral involvement of trigeminal (CN5), facial (CN 7), vestibulocochlear (CN 8).[18]
Elevated Intracranial Pressure
The change in intraocular pressure can cause downward herniation of the brainstem, resulting in stretching or compression of the sixth nerve. The abducens nerve is located near the pons and Dorello's canal, making it susceptible to such effects.
In patients with pseudotumor cerebri, abducens nerve palsy can occur along with other symptoms, such as papilledema and visual field defects, resulting in blind spot enlargement.
Other pathologies associated with elevated cranial pressure are subarachnoid hemorrhage, infection of the meninges (viral, bacterial, or fungal), inflammatory conditions (sarcoidosis), or infiltrative causes such as lymphoma, leukemia, and carcinoma.[19]
Petrous Apex Syndrome
- Gradenigo Syndrome: Also known as Gradenigo's Triad, this is a rare condition characterized by a combination of symptoms that include Abducens nerve palsy, Facial nerve (CN 7) involvement causing reduced hearing, ipsilateral facial pain along the trigeminal nerve (CN 5) distribution and ipsilateral facial paresis (due to CN 7). Tumors in the cerebellopontine angle, such as acoustic neuromas and meningiomas, can also affect the sixth cranial nerve and other nearby cranial nerves, resulting in hearing loss and decreased corneal sensitivity. This can sometimes be mistaken for petrous apex syndrome.[20]
- Pseudo-Gradenigo Syndrome: This condition presents with hearing loss, sixth nerve palsy, and trigeminal symptoms. It is typically caused by brainstem lesions such as cerebellopontine angle tumors. Nasopharyngeal carcinoma may also mimic Gradenigo's syndrome as it blocks the Eustachian tube.[21]
Cavernous Sinus Syndrome
- Nasopharyngeal carcinoma: This carcinoma may cause sixth nerve palsy, typically occurring between the fourth and seventh decades. Symptoms may include nasal obstruction, rhinorrhoea, epistaxis, and serous otitis media.[22]
- Intracavernous internal carotid artery aneurysm: Aneurysms in the cavernous sinus can involve the sixth and the third cranial nerves, which are most vulnerable in this location. However, the proportion of aneurysms causing palsy is very small, approximately 3%.[23]
- Carotid-cavernous fistula (CCF): CCF refers to an abnormal connection between the internal carotid artery and the cavernous sinus. This condition can result in arterialization of the sinus and ocular and orbital veins leading to symptoms such as pain, congestion, chemosis, proptosis, ocular pulsation, and double vision.[24]
- Tolosa-Hunt syndrome: This idiopathic sterile inflammation affects the anterior portion of the cavernous sinus and causes sixth nerve palsy.[25]
Meningioma
Meningiomas along the sphenoid ridge, anterior clinoid, or tuberculum sellae can be associated with sixth nerve palsy. In addition to this palsy, these meningiomas may cause exophthalmos, bitemporal hemianopia, monocular blindness, and upper temporal junctional scotoma.[2]
Miscellaneous
Miscellaneous causes can lead to an abducens nerve palsy, such as metastatic lesions, neurofibromatosis, syphilis, herpes zoster, multiple myeloma, craniopharyngioma, and lymphoma.
Orbital Syndrome Involving Sixth Nerve Palsy
Patients experiencing orbital syndrome with sixth nerve palsy exhibit various symptoms, including proptosis, conjunctival chemosis, optic atrophy, and papilledema. Horner syndrome may also manifest in these cases, while ptosis might go unnoticed due to the masking effect of proptosis. Other tumors that can present with similar symptoms are orbital tumors, pseudotumors, thyroid eye disease, orbital cellulitis, and myositis.[26]
Isolated Sixth Nerve Palsy Syndrome
Isolated sixth nerve palsy can arise from various factors, including diabetes, hypertension, and recent viral infections. The isolated involvement can also be recurrent. Ophthalmic migraine can also cause abducens nerve palsy, and the involvement can be either central or peripheral. When imaging results reveal mixed findings, determining the specific type of palsy becomes challenging. Immunologic damage to the sixth nerve can occur at any point.[2]
Epidemiology
The sixth cranial nerve is the most commonly affected ocular motor nerve in adults. In children, it is the second most common, following the fourth cranial nerve, with an incidence of 2.5 cases per 100,000. Poorly controlled diabetes is a significant risk factor for developing abducens nerve palsy.[9]
A study of the Korean population revealed an overall incidence rate of 4.66 cases of sixth cranial nerve palsy per 100,000 individuals per year within the patient population. The incidence of this condition demonstrated an upward trend with advancing age. The incidence significantly increased at 60, reaching its peak between 70 and 74.[27]
The incidence rates of sixth cranial nerve palsy vary depending on the underlying cause. The reported incidence ranges are as follows: traumatic causes for 3% to 30%, aneurysms for up to 6%, demyelination or miscellaneous factors for 10% to 30%, idiopathic cases for 8% to 30%, ischemic causes for up to 36%.
A 15-year study in the United States, involving 137 cases, reported an age- and gender-adjusted incidence rate of sixth nerve palsy to be 11.3 per 100,000. The study found that the peak incidence occurred in the seventh decade of life. Among the cases, there were 4 cases of bilateral sixth nerve palsy and 16 cases of multiple cranial nerve palsy.[27]
Pathophysiology
The abducens nerve supplies the ipsilateral lateral rectus, which is responsible for horizontal eye movement. Consequently, when the sixth cranial nerve is affected, deviations occur only in the horizontal plane. In cases where only the isolated peripheral nerve is involved, no vertical or torsional movements are present.[28]
The abducens nerve is primarily responsible for ipsilateral eye abduction. When abducens nerve palsy occurs, the affected nerve cannot transmit signals to the lateral rectus muscle, resulting in an inability to abduct the eye and subsequent horizontal diplopia. In cases involving central nervous system defects, the sixth nerve tract can be localized based on characteristic findings associated with each type of lesion.[29]
Involvement of the sixth nerve nucleus causes ipsilateral gaze palsy. The absence of contralateral adduction helps distinguish a nuclear lesion from a fascicular or nonnuclear lesion. When intracranial pressure is elevated, and the sixth nerve is stretched, a false localizing sign can occur, indicating abducens nerve palsy as the nerve crosses the clivus.
Abducens nerve palsy can also result from post-viral syndrome in the pediatric and adolescent populations, while in adults, it can present as ischemic mononeuropathy.[30]
History and Physical
Patients who develop abducens nerve palsy often present with binocular horizontal diplopia, which refers to double vision when viewing objects side by side. This is due to a notable weakness in the ipsilateral lateral rectus muscle, resulting in an inability to abduct the affected side.[31] Some patients may present with a constant head-turning movement to maintain binocular fusion and reduce the degree of diplopia.[32] The diplopia is more pronounced when looking into the distance or during lateral gaze.
Additional clinical history findings may include vision loss, headache, vomiting, trauma, hearing loss, recent lumbar puncture, or recent viral illness. Patients may also present with esotropia, head turn, facial pain, or numbness. Some patients may have underlying conditions such as giant cell arteritis, sharp shooting temporal headache, and facial pain. All patients presenting with these symptoms need a detailed ophthalmological examination.[33]
When assessing a patient with abducens nerve palsy, a comprehensive evaluation should be conducted, including the following:[34]
- Visual acuity evaluation
- Binocular single vision
- Stereopsis
- Ocular movement assessment
- Squint evaluation
- Measurements at near and distance
- Cardinal positions of gaze
- Assessment of fusional amplitude
- Manifest and cycloplegic refraction
- Anterior and posterior segment evaluation
Measuring ocular movements during lateral gaze and assessing duction and ocular versions are valuable for identifying incomitance associated with abducens nerve palsy.
Patients with sixth nerve palsy have slow saccadic velocity in side gaze, which helps diagnose.
In pediatric patients, tumors and trauma are the most common etiologies of sixth nerve palsy. Therefore, a thorough and careful evaluation must be performed to rule out serious etiologies. It is imperative to consider the pseudo-restrictive effects of alternating monocular fixation and vergence, as assessing both eyes simultaneously may lead to misleading results. Thus, independent evaluation of each eye is essential.[35]
Diplopia is the most common symptom in patients with abducens nerve palsy. The characteristic diplopia experienced is horizontal and uncrossed, primarily affecting distant vision rather than near vision. The diplopia is more pronounced in the direction of the affected muscle and improves with a contralateral gaze. In acute onset sixth nerve palsy cases, the deviation is more prominent when the paretic muscle is fixating compared to the nonparetic muscle. This follows Hering’s law of primary and secondary deviations.[31]
The other symptoms accompanying sixth nerve palsy depend on the underlying etiology—patients with raised intracranial pressure present with headache, ocular pain, nausea, vomiting, and tinnitus. Conversely, low intracranial pressure due to CSF leak can also lead to abducent nerve palsy, accompanied by headache, mimicking the symptoms of raised ICP. Patients with a neurological etiology present with neurological signs and symptoms. For example, those with subarachnoid hemorrhage can exhibit leptomeningeal irritation and a feature of cranial nerve palsy.[36]
When the cause of sixth nerve palsy involves the brainstem and affects the sixth nerve fasciculus, it can lead to ipsilateral facial weakness, sensory involvement, and contralateral hemiparesis (Millard-Gubler syndrome). In the event of multiple cranial nerve palsy, the lesion can be localized to various anatomical sites, including the meninges, orbital apex, superior orbital fissure, and cavernous sinus.
Evaluation
The sixth cranial nerve palsy diagnostic workup depends on the suspected underlying cause. A thorough evaluation should be conducted in cases involving children, as there is a significantly higher risk of neoplastic causes. Neuroimaging should be performed promptly at the time of injury in the setting of abducens nerve palsy associated with trauma. A lumbar puncture should be performed if elevated intracranial pressure is suspected as the cause. When an ischemic etiology is suspected palsy is suspected, MRI is recommended as the preferred modality because of its superior capability of imaging the posterior fossa.[37][38]
MRI is indicated in patients younger than 50 without vasculopathy, mainly when there is a history of associated pain or neurological abnormalities, as well as with patients with a history of carcinomas, bilateral abducent nerve involvement, or papilledema. If the palsy doesn't improve within 3 to 4 months or when other cranial nerves are involved, a detailed medical, neurological, and imaging workup should be conducted for microvascular ischemic sixth nerve palsy.[39]
Laboratory Studies
In the workup of sixth cranial nerve palsy, the following laboratory studies may be considered:
- Complete blood cell count: Assessing for any abnormalities
- Diabetes profile: Includes fasting glucose, 2-hour postprandial glucose, glycosylated hemoglobin (HbA1C), and glucose tolerance test.
- Erythrocyte sedimentation: Measuring for inflammation.
- C-reactive protein: Testing to assess for possible giant cell arteritis.
- Platelet count: Evaluation for thrombocytopenia in elderly patients.
- Acetylcholine receptor antibodies: Considered if myasthenia gravis is suspected.
- Rapid plasma reagin test: Screening for syphilis infection.
- Fluorescent treponemal antibody-absorption test: Used to confirm syphilis diagnosis if there is a suspicion.
- Lyme titer: Testing for suspected Lyme disease.
- Thyroid function tests: Assessing thyroid hormone levels
- Antinuclear antibody test: Detecting autoantibodies associated with various autoimmune conditions.
- Rheumatoid factor test: Checking for possible underlying rheumatoid arthritis.
Other Tests
Several factors should be considered and assessed when evaluating a patient with sixth cranial nerve palsy. It is essential to examine the patient's blood pressure for any abnormalities or signs of hypertension, as specific causes of sixth nerve palsy can be associated with vascular conditions. A thorough history should be obtained, and attention paid to recent trauma, ocular infections, transient loss of vision, and fluctuating symptoms. The other cranial nerve should be examined in detail to identify any additional neurological abnormalities.
Higher mental functions should be assessed along with sensory and motor examination. A detailed otoscopic examination should be mandated in pediatric patients to rule out complicated otitis media.
Treatment / Management
The management of sixth nerve palsy depends on the underlying etiology. The initial focus should be addressing any uncontrolled systemic pathology in the patient. For most patients, sixth nerve palsy resolves spontaneously without requiring systemic treatment. However, in children, treatment approaches may be considered.
Treatment options for children with sixth nerve palsy include alternate patching, prism therapy, strabismus surgery, and botulism toxin injections. Alternate patching involves patching each eye alternatively for a few hours each day.[40] This approach is used to prevent amblyopia in the affected eye. Prism therapy requires placing a temporary press-on prism on the lens of the affected eye to help align the visual axes. Children who do not show improvement with prism therapy would be eligible for strabismus surgery to correct the misalignment. Botulinum toxin injections can sometimes be administered into the medial rectus muscle of the affected eye to prevent contracture and nasal deviation.[41][42][43]
Using Bangerter filters or patches also helps eliminate diplopia and confusion and prevents amblyopia in children. These filters or patches can also reduce the possibility of ipsilateral medial rectus contracture. Additionally, Fresnel prisms can help patients maintain single binocular vision in the primary position when placed in a base-out position.[44]
In most cases of microvascular sixth nerve palsy, no intervention is required, and the condition resolves spontaneously with observation alone. It takes nearly 3 to 6 months for the symptoms to resolve independently. However, the underlying cause of the abducens nerve palsy will dictate the specific treatment approach.
For example, if the cause is temporal arteritis, steroid medications may be prescribed as part of the treatment plan. When the cause is related to intracranial pressure, such as pseudotumor cerebri and cancer, the pressure must be reduced through surgical intervention or by performing a lumbar puncture.
Treatment of persistent sixth nerve palsy that does not resolve spontaneously would be similar to those used in children. However, alternative patching has not proven effective in adults.[45]
Surgical treatment for sixth nerve palsy is reserved for patients with stable orthoptic status for at least 6 months. Before undergoing any surgical intervention, every patient should undergo a forced duction test for meticulous surgery planning.[46] Once the stability of the orthoptic status has been established and the forced duction test has been conducted, the appropriate surgical procedure can be planned.
The surgical technique employed will depend on the underlying cause of the sixth nerve palsy and the patient's condition. Surgical options may include muscle transposition procedures, muscle recessions, or other corrective techniques to address the imbalance of ocular muscle function.
- The Resect and Recess procedure is a surgical approach performed for patients with residual lateral rectus function in cases of sixth nerve palsy. This procedure involves resecting the lateral rectus muscle on the affected side and recessing the same side medial rectus muscle. Alternatively, the procedure can be modified by resecting the lateral rectus muscle and recessing the medial rectus muscle on the affected side.[47]
- If the lateral rectus function is absent, transposition surgeries can be considered an alternative surgical approach. These procedures include tendon transposition, Jensen procedure, Hummelsheim procedure, Augmented Hummelsheim with resection and with or without Foster modifications, and Knapp procedure. Superior rectus transposition, combined with medical rectus recession, has improved esotropia, head positions, and abduction in patients with abducens palsy.[48]
Differential Diagnosis
The differential diagnosis for abducens nerve palsy is extensive and includes the following:
- Myasthenia gravis
- Type 1 and 3 Duane retraction syndrome (DRS) in children [49]
- Thyroid eye disease
- Syphilis [50]
- Pseudotumor cerebri
- Spasm of the near reflex
- Orbital medial wall fractures
- Lyme disease
- Trauma [51][52][53][54]
- Neoplasm
- Delayed break in the fusion
- Old blowout fracture
- Diabetes mellitus
- Hypertension
- Aneurysms
- Vasculopathy
- Congenital esotropia [55][56]
- Sphenoiditis
- Lateral rectus myositis
- Chronic suppurative otitis media
- Miller-Fisher syndrome
- Neoplasms
- Neuromyotonia
In DRS, a palpebral fissure narrowing occurs upon adduction of the affected eye. However, there is no narrowing in sixth nerve palsy, differentiating the 2 conditions. Patients with thyroid eye disease may present with bilateral involvement, although unilateral involvement can occur, with symptoms such as proptosis and inflamed conjunctiva. In myasthenia gravis, symptoms include fluctuating diplopia along with fatigue, shortness of breath, and hoarseness.
Prognosis
The prognosis of abducens nerve palsy varies depending on the underlying cause. When caused by a viral illness, complete remission is commonly observed. However, residual symptoms may persist when the palsy is secondary to trauma. The most significant improvement is typically seen in the first 6 months. Most patients who experience idiopathic sixth cranial nerve palsy recover completely, although a few individuals may experience permanent vision changes.[2]
Complications
Complications associated with abducens nerve palsy vary based on the underlying etiology. The most common complication following surgical correction is the potential of over- or under-correction. Such complications can be effectively managed postoperatively using prisms to achieve optimal alignment.
A list of complications following surgical correction are as follows:
- Overcorrection
- Under correction
- Slipped muscle
- Lost muscle
- Muscle hemorrhage
- Iatrogenic injury to the muscle
- Anterior segment ischemia
- Diplopia
- Steroid-induced glaucoma [57][58]
Postoperative and Rehabilitation Care
Regular follow-up is essential for all patients who have undergone surgical correction of strabismus. Postoperative medication should be continued in tapering doses as prescribed. Patients should be educated about the importance of regular and timely usage of topical steroids and lubricants. They should also be informed about the potential occurrence of postoperative diplopia and how it can be managed using prisms.[59]
Consultations
All patients displaying signs of sixth nerve palsy should undergo a thorough evaluation by a pediatric ophthalmologist, strabismologist, and neurologist. This comprehensive evaluation aims to accurately diagnose and determine the underlying cause of the sixth nerve palsy.[40]
Deterrence and Patient Education
Patients should be informed about the possibility of the self-limiting nature of the condition and may be advised to undergo an observation period of about 6 months. Surgical correction can be offered if the patient fails to show any improvement during this time. Of course, a known underlying condition must be addressed first, and patient counsel will primarily focus on that issue.[60]
Pearls and Other Issues
Abducens nerve palsy is a condition that requires careful consideration of the underlying pathology responsible for the observed lateral rectus paresis. The process involves employing a systematic differential diagnosis approach that follows the anatomical pathways of the nerve to determine the underlying cause. Once the cause is identified, treatment can be targeted toward addressing the underlying condition.[15]
Enhancing Healthcare Team Outcomes
Abducens nerve palsy is a frequently encountered condition characterized by horizontal diplopia. However, accompanying symptoms may vary depending on the underlying cause. Due to the numerous etiologies associated with this condition, a collaborative approach involving multiple healthcare professionals is essential for effective management. The team typically includes a neurologist, ophthalmologist, neurosurgeon, and radiologist. Additionally, an ophthalmology specialty-trained nurse should assist with surgical interventions and educate patients about the condition and its treatment. When a patient presents with horizontal diplopia, prompt referral to a neurologist should be made by the nurse practitioner or primary care provider. The underlying cause determines the prognosis and outcome of abducens nerve palsy.[61][62]