Continuing Education Activity
Rubella is a mild viral disease that typically occurs in children and non-immune young adults. In pregnant women, rubella infection can produce a constellation of severe birth defects known as congenital rubella syndrome. To avoid the high morbidity associated with this condition, healthcare providers should play an active role in the prevention and diagnosis of rubella. This article reviews the evaluation, management, and prevention of this condition.
Objectives:
- Summarize the epidemiology of Rubella virus.
- Describe the physical exam findings and complications associated with postnatal rubella infection and congenital rubella syndrome.
- Review the adequate diagnostic tests and treatment options available for rubella infection, including management consideration in pregnant women.
Introduction
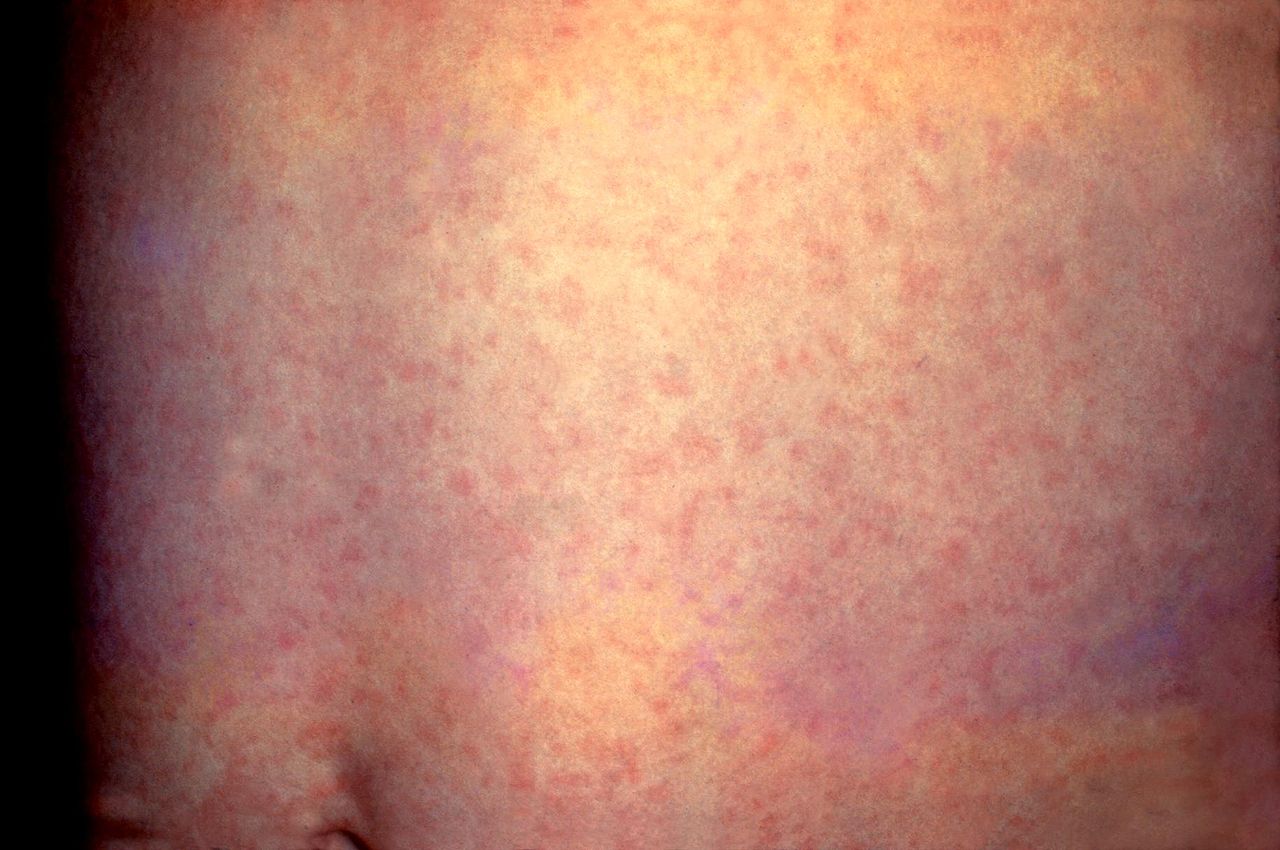
Rubella, or German measles, is a mild viral infection that typically occurs in children and non-immune young adults. It typically begins with low-grade fever, malaise, and lymphadenopathy, followed by a brief generalized erythematous maculopapular rash. [1][2]
In nonpregnant individuals, rubella is generally a self-limited and benign infection. However, maternal rubella infection, especially during the first 10 weeks of gestation, can result in miscarriage, fetal death, or severe birth defects collectively known as congenital rubella syndrome (CRS).[3]
After the introduction of the live attenuated rubella vaccine in 1969, the incidence of rubella infection has decreased dramatically in many countries and was effectively eradicated from the United States; however, rubella remains a public health concern and a significant source of disability around the world.[2]
Etiology
Rubella virus is the sole member of the genus Rubivirus within the newly classified Matonaviridae family.[4] It is a single-stranded, positive sense enveloped RNA virus. Rubella virus encodes two non-structural proteins (p90 and p150) and three structural proteins; glycoprotein (E1 and E2) and the capsid protein (CP). The E1 protein is responsible for receptor-mediated endocytosis and induces the immune response through hemagglutination-neutralizing epitopes.[5][6] The virus is sensitive to heat (temperature >56°C), ultraviolet light, and extremes of pH (pH <6.8 or >8.1).[1]
Epidemiology
In the pre-vaccine era, the peak incidence of rubella was in children aged 5 to 9 years, and the peak rates usually occur in late winter and early spring, with sporadic cases appearing year-round in temperate climates.[1][2][7]. After the implementation of widespread vaccination in the United States, rubella has become increasingly rare, with only occasionally imported cases from those countries where rubella is endemic.[1]
Rubella affects both sexes equally in children, whereas in adults, rubella affects more women than men.[1] After the introduction of the live-virus vaccine, outbreaks occurred more commonly among older adolescents and young adults.[7][8] Risk factors for rubella include under-vaccinated or unvaccinated individuals, traveling to endemic areas, exposure to household members with rubella, and immunodeficiency.[1]
In countries where rubella is endemic, it is estimated to occur at a rate of 1.30/100,000 in the general population.[2]
Pathophysiology
Humans are the only known reservoir for rubella. The virus is contracted through person-to-person contact via aerosolized particles from the respiratory tract secretions of affected individuals.[1][2][7] After infecting the cells of the susceptible host through receptor-mediated endocytosis, the virus replicates in the nasopharyngeal cells and then spreads to the regional lymphoid tissue of the nasopharynx and upper respiratory tract. This process is followed by a viremic phase, which is characterized by hematogenous dissemination of the virus to multiple organs, and it usually occurs 5 to 7 days after inoculation. The exanthem appears approximately 2 to 8 days after the onset of viremia and resolves 3 days later as the humoral immune response develops.[1] An infected individual is contagious from 8 days before to 8 days after the onset of the rash.[2] Immunity acquired after recovering from natural infection or through vaccination is life-long; however, reinfection has been reported after both wild type rubella infection and after receiving one dose of rubella vaccine.[2][7]
In congenital rubella syndrome (CRS), fetal infection occurs transplacentally during the maternal viremic phase.[1] The risk of transmission to the fetus depends on the time of maternal infection; when infection with rubella occurs before 10 weeks of gestation, it may cause multiple fetal defects in up to 90% of cases. The risk of congenital defects declines with infection later in gestation.[7] The pathogenesis of CRS is multifactorial and not well understood[2]. In CRS, damage to the fetus may result from several mechanisms including epithelial necrosis of chorionic villi, apoptosis of infected cells by direct viral damage, inhibition of mitosis, and restricted development of precursor cells by the virus, and cytopathic damage to endothelial cells of blood vessels resulting in ischemia of developing organs.[1]
History and Physical
Postnatal infection with rubella can be asymptomatic in approximately 25% to 50% of the patients, especially in young children. The incubation period ranges from 14 to 21 days and is followed by a prodromal illness characterized by low-grade fever, malaise, anorexia, headaches, sore throat, and adenopathy. The lymphadenopathy typically involves postauricular, suboccipital, and anterior cervical lymph nodes. The exanthem could be the first manifestation in children and consists of pinpoint pink macules and papules that classically begin on the face and rapidly spreads to involve the trunk and extremities. Occasionally, the rash is scarlatiniform or purpuric. The rash typically lasts for 3 days and fades in the same directional pattern as it appears.[1] Petechiae on the soft palate (Forchheimer spots) can also be observed in approximately 20% of the patients.
Rubella infection during embryogenesis leads to the classic triad of cataracts, congenital heart defects, and sensorineural deafness; however, many other defects might be observed. During the neonatal period, CRS has been associated with low birth weight, thrombocytopenic purpura, hemolytic anemia, hepatosplenomegaly, and meningoencephalitis. These manifestations are usually transient. Other clinical manifestations of CRS include ophthalmopathies (retinopathy, glaucoma, chorioretinitis, iris hypoplasia, and microphthalmia), cardiac abnormalities (patent ductus arteriosus, pulmonary artery hypoplasia), psychomotor retardation, and microcephaly.
Of all the manifestations, deafness is the most common finding and could be the only defect observed. Individuals that survive the neonatal period may face severe disabilities (e.g., visual and hearing impairments) and have an increased risk for developmental disorders, including autism. In addition, a variety of late-onset endocrine, cardiovascular and neurological abnormalities have been described.[1][2]
Evaluation
The clinical diagnosis of rubella is difficult because the manifestations can be mild and non-specific. Therefore, physicians must rely on serological testing to confirm rubella.
The most common diagnostic test for recent postnatal infection is the detection of rubella-specific IgM antibodies by using an enzyme immunoassay. Rubella-specific IgM antibodies are usually detectable 4 days after the onset of rash.[9] In addition, rubella infection and reinfection can be demonstrated by a four-fold or greater increase in rubella-specific IgG titers between acute and convalescent sera. Recent primary rubella infections can also be confirmed by rubella-specific low avidity IgG. [7]
In those cases in which a pregnant woman has been exposed to a suspected rubella case, a specimen of blood should be tested as soon as possible for the measurement of rubella-specific IgG antibodies. If it is positive, then the woman was likely to be immune and could be reassured. If it is negative, a determination rubella-specific IgG and rubella-specific IgM antibodies should be obtained in 3 weeks to exclude an asymptomatic primary rubella infection. [1]
Congenital rubella infection may be diagnosed prenatally either by a demonstration of specific IgM in fetal blood or by the detection rubella RNA in amniotic fluid, fetal blood, or chorionic villus biopsy using reverse transcription-polymerase chain reaction (RT-PCR). In the newborn period, the serologic diagnosis of congenital rubella is made by the detection of rubella-specific IgM within the first 6 months of life. Congenital rubella infection can also be confirmed by the increase or persistence of rubella-specific IgG in the infant after 6 to 12 months of age. Detection of the viral genome in nasopharyngeal swabs, urine, and oral fluid by RT-PCR provides laboratory evidence of CRS.[2]
Treatment / Management
Treatment of postnatally acquired rubella in non-gravid individuals is mainly supportive and consists of the use of non-steroidal anti-inflammatory drugs for fever, arthralgia and/or arthritis.[1] In pregnant women, the management depends on the gestation age at the onset of infection.[2]If the infection occurs before 18 weeks of gestation, the fetus is at high risk for infection and subsequent malformation, and management should include the consideration of pregnancy termination according to local ethical and legislative regulations. If the infection occurs after 18 weeks of gestation, the pregnancy could be continued with ultrasound monitoring and specific neonatal management. [2][10] Treatment of children with congenital rubella syndrome should be symptomatic and organ-specific. It usually involves a multidisciplinary approach and requires pediatric, ophthalmologic, cardiac, audiological, and neurodevelopmental evaluation. Long-term follow up is needed to monitor for delayed manifestations.[1]
Differential Diagnosis
Rubella needs to be distinguished from other infections with similar maculopapular rashes, including measles, human herpesvirus 6 and 7, infectious mononucleosis, cytomegalovirus, arboviruses (Zika virus, West Nile fever, Ross River fever, and Chikungunya virus), enteroviruses, scarlet fever, and mycoplasma infection. Other conditions to be considered in the differential diagnosis for rubella are non-infectious causes like Kawasaki disease, drug eruption, and contact dermatitis. [1]
Prognosis
Postnatal infection with rubella is generally mild, self-limited, and has an excellent prognosis. However, the prognosis of children with congenital rubella syndrome is less favorable and varies depending on the severity and number of organs affected. The risk of mortality risk is high in infants with thrombocytopenia, interstitial pneumonia, hepatosplenomegaly, and pulmonary hypertension. [1] Also, individuals with congenital rubella syndrome are at risk of long-term complications, including blindness, cardiac failure, developmental delays, and reduced life expectancy.[11]
Complications
The development of polyarthritis and polyarthralgia is the most common complication of rubella infection, affecting up to 70% of adolescents and adult women. It is usually symmetric and involves the wrists, fingers, knees, and ankles. Other manifestations, although rare, include thrombocytopenia, hemolytic anemia, myocarditis, pericarditis, hepatitis, orchitis, retinopathy, uveitis, Guillain-Barré syndrome, and post-infection encephalitis. Rubella infection during pregnancy may lead to miscarriage, intrauterine fetal demise, premature labor, intrauterine growth retardation, and congenital rubella syndrome. [1] The risk of developing complications is highest if the infection is contracted within the first 12 weeks of gestation.
Deterrence and Patient Education
Parents should be educated and counseled on the importance of routine immunization in infants and young children. It is also essential to identify and immunize all susceptible women of childbearing age prior to conception.
Pearls and Other Issues
Universal immunization of all susceptible individuals with rubella vaccines is the cornerstone to the prevention of rubella and, more importantly, congenital rubella syndrome. In the United States, the rubella vaccines consist of a live attenuated RA 27/3 strain. The vaccine is usually administered in combination with measles and mumps (MMR) or measles, mumps, and varicella (MMRV), with the first dose at ages 12-15 months and the second dose at ages 4-6 years.[1][2] Immunization of all unvaccinated adolescents and adults with at least one dose of rubella vaccine is also recommended. Contraindications for rubella vaccination include a history of an anaphylactic reaction to a previous dose or any of the vaccine's components (e.g., neomycin and gelatin), and immunodeficiency. MMR vaccine is not contraindicated in individuals with an allergy to eggs.
Rubella vaccine should be deferred after recent use of high-dose corticosteroids, recent administration of immunoglobulin or blood products, and after another live vaccine has been given (if not given simultaneously).[1] Due to a theoretical teratogenic risk of the rubella vaccine, women of childbearing age without documentation of rubella immunity should get vaccinated at least one month before they become pregnant. However, if pregnancy occurs within 28 days of immunizations or it is inadvertent given to pregnant mothers, termination of pregnancy is not warranted as there is no evidence that the rubella vaccine can cause fetal or maternal complications. [1][2]
Adverse effects of the rubella vaccine are uncommon in children. MMR administration is associated mainly with fever and rash in 15% and 5% of vaccinees, respectively. Arthralgia and arthritis can develop after vaccination, usually occurring in postpubertal women. [2]Less common adverse reactions are transient lymphadenopathy, parotiditis, and febrile convulsions. Moderate to severe sequelae such as anaphylaxis, anterior uveitis, thrombocytopenic purpura, or encephalitis is very rare. [1] Despite popular beliefs, there is not known association between MMR vaccination and autism. [12]
Passive immunization with immunoglobulin is not recommended for non-pregnant contacts. For susceptible pregnant women with known exposure to rubella in which termination of pregnancy is not an option, the administration of immunoglobulin within 72 h of exposure should be considered. [13]
Enhancing Healthcare Team Outcomes
Suspected cases of rubella should be notified immediately to the Centers for Disease Control and Prevention (CDC). Once the diagnosis of rubella is confirmed, the patient should be promptly isolated for at least 7 days after onset of the rash. Because rubella is transmitted primarily by inhalation of virus-laden airborne droplets, standard and droplet precautions are recommended for hospitalized patients. The management of congenital rubella syndrome should include a multidisciplinary team, as previously discussed. Children with congenital rubella syndrome can shed the virus in saliva and urine for several months and therefore are contagious. These individuals should be isolated until two pharyngeal or urine cultures have negative results.[1]