Introduction
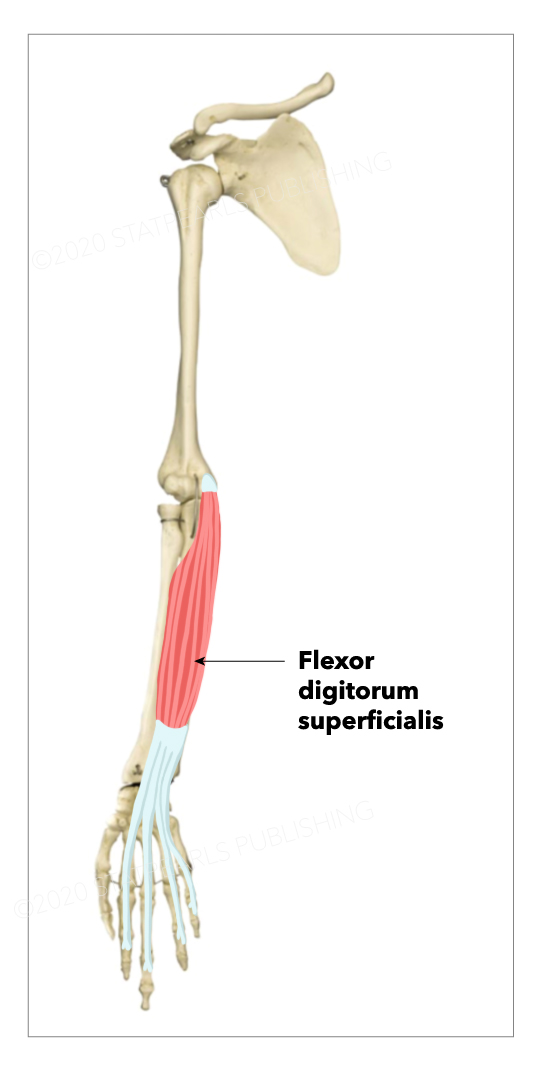
The flexor digitorum superficialis (FDS), formerly known as the flexor digitorum sublimis, is the largest of the extrinsic flexors of the forearm (see Image. Flexor Digitorum Superficialis). It forms the intermediate muscle layer between the superficial and deep muscle groups of the forearm.[1] It contains four digital components, with a tendon that inserts onto each corresponding finger. The flexor digitorum superficialis is the primary flexor of the proximal interphalangeal (PIP) joints of the middle phalanges, but it also assists in flexion of the metacarpophalangeal (MCP) joints.
Structure and Function
Structure
The flexor digitorum superficialis muscle has two origins. The humeroulnar head originates off the medial epicondyle of the humerus and the coronoid process of the ulna. The radial head originates on the upper half of the volar aspect of the radial shaft. The median nerve and ulnar artery enter the forearm by passing between the humeroulnar and radial heads of the flexor digitorum superficialis muscle. The flexor digitorum superficialis courses along the volar aspect of the forearm, superficial to the flexor digitorum profundus and flexor pollicis longus muscles, and deep to the palmaris longus, flexor carpi radialis, flexor carpi ulnaris, and pronator teres.
As it courses down the forearm, the flexor digitorum superficialis separates into two planes of muscular fibers, superficial and deep:
- The superficial plane further divides to supply tendons for the middle and ring fingers.
- The deep plane provides a muscular slip to join the part of the superficial plane associated with the tendon of the ring finger and then divides to supply tendons for the index and little fingers.
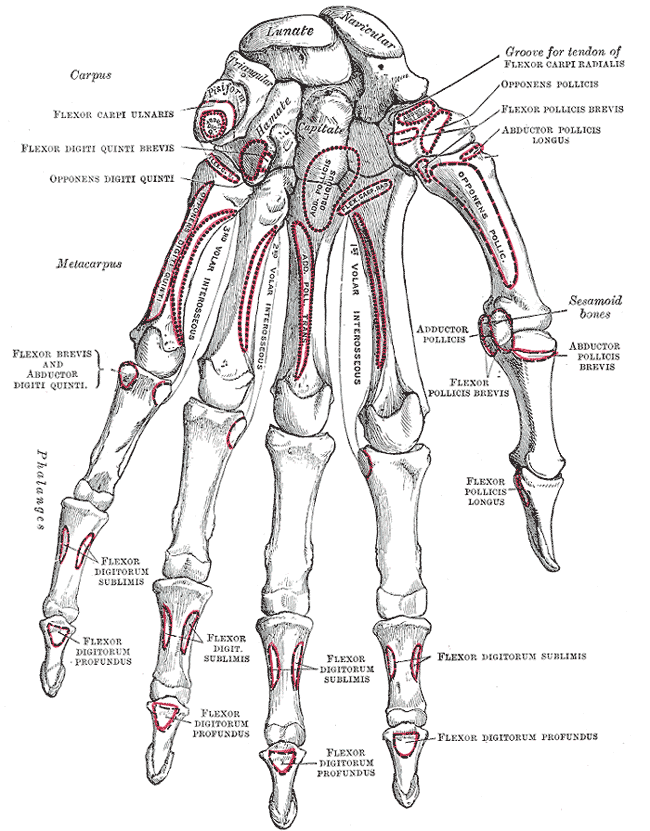
The four flexor digitorum superficialis tendons pass deep to the transverse carpal ligament, constituting four of the nine total tendons in the carpal tunnel.[2] Continuing into the palm, the flexor digitorum superficialis tendinously slips insert onto the middle phalangeal bases of second, third, fourth, and fifth digits, on the volar surface of the hand (see Image. Bones of the Left Hand).
Function
The flexor digitorum superficialis flexes the middle phalanges of the medial four digits at the proximal interphalangeal joints. It also flexes the proximal phalanges at the metacarpophalangeal joints and the wrist joint. Flexor digitorum superficialis can flex each finger it serves independently.[1] The flexor digitorum superficialis is one of the long flexors of the digits along with the flexor digitorum profundus. The flexor digitorum profundus flexes the digits slowly. Flexor digitorum superficialis reinforces this action when speed and flexion are required against resistance.
Embryology
In the fourth week of development, the small upper limb buds form.[1] The limb bud is an outgrowth of somatic mesoderm, forming muscles, nerves, and vasculature, as well as lateral plate mesoderm, which will form bone, cartilage, and tendon into the ectoderm.[3] By week 7, every upper limb muscle can be grossly identified and contains muscle fibers. The more superficial muscles, like the flexor digitorum superficialis, will differentiate before the deep muscles.
Blood Supply and Lymphatics
The primary blood supply to the flexor digitorum superficialis muscle is from the ulnar artery. Lymphatic drainage of the upper limb occurs via the axillary lymph nodes.
Nerves
The flexor digitorum superficialis muscle receives innervation by the median nerve (C7, C8, and T1).[4]
Physiologic Variants
There are several physiological anomalies of the flexor digitorum superficialis muscle and tendon that have been described in the literature and typically occur in the palm.
These variations may include those involving muscle belly itself, the presence of additional accessory tendons, duplicate tendons, and variant tendon-tendon anastomoses.[1][5] Some of these anomalies mimic soft tissue tumors or cause nerve entrapment secondary to mechanical compression. For example, in rare cases, the flexor digitorum superficialis muscle may extend into the carpal tunnel and cause a patient to complain of intermittent symptoms with repetitive motion consistent with carpal tunnel syndrome (CTS).[6][1] Also, flexor digitorum superficialis accessory muscles are a known etiology in causing anterior interosseous nerve (AIN) syndrome.[7]
The literature has classified the anatomical variations of the flexor digitorum superficialis muscle and tendon as followed[8]:
- Type I: A small muscle attached to the flexor digitorum superficialis tendon proximally and index finger distally. During digital flexion, this muscle invades the carpal tunnel and could cause intermittent symptoms related to median nerve compression.
- Type II: A small muscle arising from the flexor retinaculum is attached to the flexor digitorum superficialis tendon in the distal palm.
- Type III: An additional digastric muscle inserted on the base of the middle phalanx of the index finger, passes under the carpal tunnel, with an apparent proximal path.
- Type IV: The flexor digitorum superficialis muscle belly that corresponds to the index finger and extends into the carpal tunnel, that can cause similar symptoms as type I.
- Type V: A small muscle crossing the median nerve anteriorly attached to the flexor digitorum superficialis muscle of the middle finger by a tendon and deep surface of the transverse carpus ligament. The anomaly was found about 8 cm proximal to the wrist fold and was unlikely to be clinically significant.
Studies have demonstrated the absence of flexor digitorum superficialis muscle or tendon components as variations that may be clinically relevant. In particular, the congenital absence of the flexor digitorum superficialis component that corresponds to the little finger may cause difficulty with determining normal function during the examination of a finger laceration.[9][10]
Surgical Considerations
Flexor Digitorum Superficialis Tenodesis, also known as the superficialis sling, is an operation that is used to treat swan neck deformity, a condition characterized by hypertension of the PIP joint of the finger and flexion posture of the distal interphalangeal (DIP) joint.[11] The goal of the procedure is to create a static volar restraint against hyperextension. The flexor digitorum superficialis muscle is often used in tendon transfer surgeries. There is a wide range of approaches, but the surgeon must have adequate access to both the point of incision, which slips off the FDS to use and the point where the tendon will be secured. The main approaches include funneling the tendon through the proximal phalanx and connecting it to the A1 or A2 pulley or securing the tendon to the proximal phalanx with bone anchors.[11] Following the operation, the affected PIP joint should be blocked from extension for about 6 weeks through immobilization with a splint.
One complication this can arise with this procedure is the creation of a flexion contracture that is greater than the degree desired. However, there is no uniform agreement in the literature regarding an optimal angle of PIP joint flexion during tenodesis.[11]
The Carpal Tunnel Release (CTR) procedure is an option when patients who are suffering from carpal tunnel syndrome do not respond to all non-operative therapies.[12] The two main approaches, open and endoscopic, both have associated risks and benefits that are well-characterized in the literature. Regardless of etiology, open CTR (OCTR) is the current gold-standard operation for the treatment of this condition, and it involves decompression of the median nerve by dividing the transverse carpal ligament (TCL).[13] Endoscopic CTR (ECTR) is a single portal surgical technique, which also involves transection of the TCL, but carries at least an increased theoretical risk of transection or injury to any of the carpal tunnel constituents.[13] Relief of CTS symptoms and full finger range of motion is usually the result in uncomplicated cases at the two-week postoperative stage, and most individuals can return to full activity after six weeks.
Clinical Significance
Testing the Function of the Flexor Digitorum Superficialis Muscle
Ask the patient to flex one out of the four medial fingers at the proximal interphalangeal joint against resistance, and the other three fingers are held in an extended position to inactivate the flexor digitorum profundus.
There are two methods which are more frequently used and accurate in practice for the clinical assessment to check for the variation of flexor digitorum superficialis muscle to the fifth finger. These include:
1. Modified Baker's test: Ask the patient to flex the proximal interphalangeal (PIP) joint of the little finger alone while the other fingers are held extended by the examiner. The little and ring fingers are then released to flex together to observe the proximal interphalangeal joint flexion improvement. Suppose the patient cannot flex the proximal interphalangeal joint of the little finger while other fingers are restrained in extension. In that case, however, the patient can flex the proximal interphalangeal joint of the 5th digit while the 4th digit is released, then it shows the absence of the 5th tendon of flexor digitorum superficial.
2. Bilateral palms test: Ask the patient to put bilateral palms and corresponding fingers face to face closely and rely on the forces of their own hands. While the little finger is ordered to flex, the adjacent fingers' influence can be observed apparently if there is a connection between the little finger and the adjacent fingers.[14]
Other clinical relevances of the flexor digitorum superficialis muscle include the following:
Swan Neck Deformity is the hyperextension of the PIP joint with flexion posture of the DIP joint that most commonly occurs secondary to rheumatoid arthritis, cerebral palsy, connective tissue disorders such as Ehlers-Danlos syndrome, or trauma.[15][16] This deformity can cause difficulty flexing the middle interphalangeal joint because tendons are located in this region. As a result, a snapping sensation can occur during flexion. Over time, swan neck deformities can become stiff and cause long-term disability.[15] Treatment of the swan neck deformity is largely dependent on severity but can include splinting or surgical intervention of the affected finger.
Carpal Tunnel Syndrome (CTS) is the most common peripheral nerve entrapment syndrome. This condition can occur secondary to a retracted flexor digitorum superficialis tendon that invades the tunnel. Patients with CTS will often present with intermittent numbness in their thumb, index, and middle fingers. Patients may also complain of discomfort in their wrist and palm of the affected hand that worsens throughout the night, weakness, and loss of grip strength. A common feature on physical exam is a positive Phalen's test, a sensitive and specific test for CTS, and usually present in moderate to severe cases.[17] The patient would be asked to flex their wrists and hold the dorsal aspects of their hands together for 1 minute. A positive test is determined by the presence of tingling in the thumb, index, and middle fingers, as well as the side of the medial half of the ring finger. Carpal tunnel syndrome can be managed surgically with a carpal tunnel release, or non-operatively with an ultra-sound guided steroid injection or wrist splint.[12] Early surgery is typically an option with clinical evidence of median nerve denervation or when the patient elects surgery as their preferred option.
Other injuries to the flexor digitorum superficialis, namely FDS belly or tendon rupture, are relatively rare but have been described occasionally by a case report.[18]