Continuing Education Activity
Hemorrhoid disease is a common pathology that can yield symptoms ranging from minimal discomfort or inconvenience to excruciating pain and significant psychosocial implications. Conservative measures are considered first-line, and a primary care provider can initiate these. Patient education is paramount. Persistent or severe hemorrhoid disease can be managed by a colorectal surgeon who has numerous modalities at their disposal. These modalities range from minimally invasive procedures to surgical hemorrhoidectomies. This activity explains how to evaluate external hemorrhoids properly and highlights the role of the interprofessional team in caring for patients with this condition.
Objectives:
Identify the risk factors for hemorrhoids.
Review the presentation of external hemorrhoids.
Summarize the treatment options for external hemorrhoids.
Outline the importance of enhancing care coordination among the interprofessional team to ensure proper evaluation and management of external hemorrhoids.
Introduction
Hemorrhoid disease is a common pathology that can yield symptoms ranging from minimal discomfort or inconvenience to excruciating pain and significant psychosocial implications.
Hemorrhoids are rich in vascular supply and have a tendency to engorge and prolapse. Symptoms can vary from mild itching and bleeding to severe pain. Unfortunately, because of the location, many patients never seek treatment for fear of embarrassment.
Conservative measures are considered first-line, and a primary care physician can initiate these. Patient education is paramount. Persistent or severe hemorrhoid disease can be managed by a colorectal surgeon who has numerous modalities at their disposal. These range from minimally invasive procedures to surgical hemorrhoidectomies.[1][2][3]
Etiology
Pathologic hemorrhoids are a result of an increased pressure gradient within the hemorrhoid plexus. This typically results from increased intra-abdominal pressure experienced in scenarios such as prolonged straining during defecation or pregnancy and labor. Not surprisingly, a history of chronic hard stool can precipitate hemorrhoid disease.[4][5]
Risk factors for hemorrhoids include:
- Family history
- Chronic diarrhea
- Sedentary lifestyle
- Obesity
- Higher socioeconomic status
- Injury to the spinal cord
- Rectal surgery
- Anal sex
- Inflammatory bowel disease
Epidemiology
Hemorrhoid disease is a common anorectal disorder affecting millions in the United States and the most common cause of rectal bleeding. Hemorrhoids are believed to affect men and women equally. They are rare under 20 years of age, and incidence peaks between the ages of 45 and 65. Estimates of hemorrhoid disease in pregnant women vary but range as high as 35%.
Pathophysiology
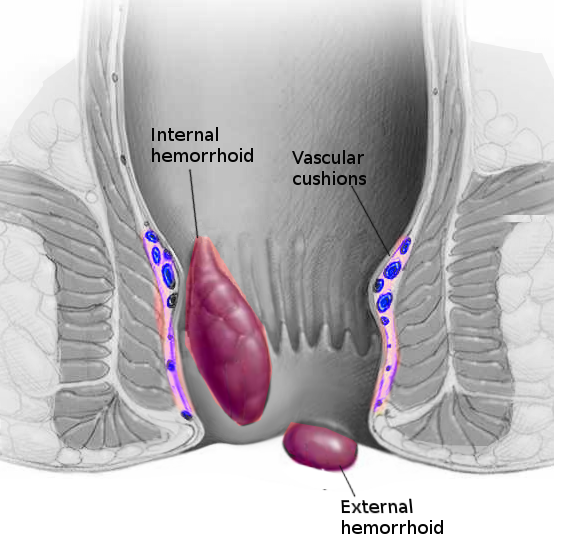
Hemorrhoids are cushions of submucosal tissue that are located within the anal canal. These structures cushion the anal canal and also support the anal canal lining. They are thought to aid in the complete closure of the anal canal at rest and to function as part of the body’s innate continence mechanism.
External hemorrhoids are covered by squamous epithelium and innervated by cutaneous nerves, which are branches of the pudendal nerve. They can occur circumferentially under the anoderm and in any location. Finally, external hemorrhoids are drained via the inferior rectal vein into the inferior vena cava.
Increased intra-abdominal pressure, such as that associated with straining, passing hard stools, or childbirth, yields venous engorgement of the hemorrhoid plexus. Bleeding, thrombosis, and prolapse can follow.
External hemorrhoids cause symptoms in the following ways:
- Acute thrombosis may be linked to a change in diet, straining with severe constipation, and physical activity.
- Pain can also result from sudden distension of the overlying skin by the blood clot. This pain may last 5 to 12 days and with a resolution of the swelling, a skin tag is visible.
Histopathology
By definition, internal hemorrhoids occur proximal to the dentate line and are covered by anorectal mucosa that is insensate. External hemorrhoids occur distal to the dentate line and are covered by richly innervated anoderm. As such, internal hemorrhoids are classically considered relatively painless, while external hemorrhoids can yield very significant pain.
History and Physical
Typical complaints associated with hemorrhoid disease include pain, bleeding, pruritis, burning, and swelling. Patients may describe bright red blood dripping into the toilet. Hemorrhoids are the most common cause of rectal bleeding.
Physical findings include:
- Skin tags
- Fistulas/fissures
- Prolapsed or thrombosed hemorrhoid
- Blood
Evaluation
A physical exam can be accomplished with the patient in the prone jackknife position or left lateral decubitus. Buttocks must be distracted for a visual examination which can readily identify many hemorrhoids, as well as other pathologies such as anal fissure, rectal prolapse, and fistulas. The digital exam is accomplished with a gloved and well-lubricated finger and can aid in excluding other palpable etiologies. Lastly, anoscopy can be performed, and patients may be asked to bear down to simulate the increased intra-abdominal pressure associated with defecation. In complicated cases, or when a patient has difficulty tolerating an exam in a clinical setting, colorectal surgeons may sometimes opt to perform an exam in the operating room under anesthesia.
Treatment / Management
Conservative therapy is considered the first-line treatment for symptomatic hemorrhoids. This includes increased dietary fiber, stool softeners, and increased water intake. Notably, the fiber must be accompanied by adequate water intake to ensure that stool is not just bulky but also soft. Polyethylene glycol is an osmotic laxative that softens stool by increasing the water content of stool. Docusate is an anionic surfactant that promotes water and lipid entry into the stool, softening it. These conservative medical measures can decrease straining and the sheering pressure associated with passing stool. This alleviates congestion and allows hemorrhoid cushions to return to their natural, non-pathologic state.
Rubber band ligation is a minimally invasive treatment option for first, second, and some third-degree internal hemorrhoids that do not respond to conservative therapy. Other minimally invasive options include sclerotherapy and infrared photocoagulation.[6][7][8][9][10]
The persistent or severe disease can be managed operatively with surgical hemorrhoidectomy. In otherwise healthy patients, hemorrhoidectomies can be performed as "same-day" surgeries. Post-operative pain is typically managed with oral narcotics, NSAIDs, and sitz baths.
The acutely thrombosed external hemorrhoid can be excised under local anesthesia. A pressure dressing should be applied and the patient should be asked to undertake sitz baths.
Other measures include:
- Adequate fluid intake
- Stool softeners
- High fiber intake
- Become physically active
- Maintain good anal hygiene
- Use analgesics for pain
The key is to avoid constipation.
Differential Diagnosis
When considering hemorrhoid disease as a diagnosis, one must give specific consideration to other potential anorectal pathologies. For example, anal fissures occur in the lower portion of the anal canal and typically yield pain and bleeding, worse with defecation. Anorectal abscesses can yield severe rectal pain and sometimes a palpable mass. These have the potential to result in life-threatening sepsis. Although rather uncommon, anal prolapse typically presents with pain during defecation, and the patient may report a palpable mass. Anal intercourse can result in proctitis that yields pain, bleeding, and even skin changes. Offending microbes include Chlamydia trachomatis, Neisseria gonorrhoeae, and Herpes simplex. Malignancy is a potential cause of blood per rectum that must be considered. If bleeding originates from hemorrhoid disease in a young, otherwise healthy patient, the complete colonic examination may be deferred in favor of a close follow-up. Patients with a family history of cancer or patients older than 49 years of age should be scheduled for a routine colonoscopy.
Staging
Hemorrhoids are classified as internal or external based on their location relative to the dentate line. External hemorrhoids occur distal to the dentate line. Internal hemorrhoids occur proximal to the dentate line and are further categorized into 4 different grades. Grade I hemorrhoids prolapse beyond the dentate line upon straining. Grade II hemorrhoids prolapse through the anus upon straining but spontaneously reduce, while grade III hemorrhoids prolapse through the anus upon straining and can only be reduced manually. Grade IV hemorrhoids have prolapsed through the anus and cannot be reduced.
Prognosis
Many cases of mild hemorrhoids resolve spontaneously or with conservative therapy. However, hemorrhoids are recurrent and can become infected, thrombosed, and lead to incontinence. Conservative management results in a recurrence rate of more than 50%; after surgery, the recurrence rate is less than 5% to 10%. After surgery, pain can be significant, and retention of urine in males is common.
Complications
The most common complication of operative hemorrhoidectomy is urinary retention, occurring in 30% to 50% of patients. Post-operative pain is typically significant and requires oral narcotics in addition to NSAIDs. Other potential complications include bleeding, infection, and loss of continence.
Postoperative and Rehabilitation Care
Postoperative pain associated with excisional hemorrhoidectomy is significant and typically requires oral narcotics in addition to NSAIDs, muscle relaxants, and sitz baths. Persistent and worsening pain accompanied by fever may signal a necrotizing soft tissue infection.
Consultations
Initial management of hemorrhoid disease includes conservative care and patient education. A primary care physician can routinely initiate this treatment. If the disease is severe or persistent, a colorectal surgeon can evaluate it and, if indicated, perform operative management.
Deterrence and Patient Education
Conservative therapy is considered the first-line treatment for symptomatic hemorrhoids. This includes increased dietary fiber, stool softeners, and increased water intake. These modifications can decrease straining and the sheering pressure associated with passing stool. This alleviates congestion and allows hemorrhoid cushions to return to their natural, non-pathologic state.
Increased fiber intake can be helpful with symptomatic hemorrhoids, but it must be accompanied by adequate water intake to ensure that stool is not just bulky but also soft. Polyethylene glycol is an osmotic laxative that softens stool by increasing its water content. Docusate is an anionic surfactant that promotes water and lipid entry into the stool, softening it.
Enhancing Healthcare Team Outcomes
External hemorrhoids affect millions of people and, even though not life-threatening, can seriously affect the quality of life. Over the years, many treatments have been developed to manage hemorrhoids, but none is perfect. Today, the aim of treatment is to prevent hemorrhoids in the first place. Hemorrhoids are best managed by an interprofessional team that includes an emergency department physician, general surgeon, gastroenterologist, and an internist. The primary care provider, pharmacist, and nurse practitioner play a vital role in educating the patient on preventing these lesions.
Conservative therapy is considered the first-line treatment for symptomatic hemorrhoids. This includes increased dietary fiber, stool softeners, and increased water intake. Rubber band ligation is a minimally invasive treatment option for first, second, and some third-degree internal hemorrhoids that do not respond to conservative therapy. [11] Other minimally invasive options include sclerotherapy and infrared photocoagulation. While surgery is effective, the results are not optimal, and recurrences are common. Many patients do have residual anorectal pain after surgery. [12]
Primary care clinicians and nurses should educate patients on the need to change their lifestyles to prevent hemorrhoids. This means becoming physically active, eating a high-fiber diet, drinking ample water, taking a stool softener, reducing body weight, and avoiding prolonged sitting. These simple measures not only reduce the risk of hemorrhoids but also decrease healthcare expenses. Only via an interprofessional approach can the morbidity of hemorrhoids be reduced.
Outcomes
The outcomes for most people who do not change their lifestyle are unsatisfactory. Even those who undergo surgery cannot be guaranteed a good result. Pain, urinary retention, and recurrence are common postoperatively. 12. [Level 5]