Introduction
The process of medical death certification is a challenging and daunting task for most healthcare practitioners and physicians who are tasked with this responsibility. In most instances, in the United States, when a death certificate must be completed, it is the responsibility of the physician to fill it out.
In instances where a crime or foul play is suspected, the medical examiner or coroner takes responsibility for filling out the death certificate. Physicians should not be concerned if the manner of death is natural, suicide, homicide, accident, or indeterminable. The burden of determination lies with the medical examiner (ME).[1][2] In rare instances, for example, the death of a hospice patient, a nurse practitioner may fill out the death certificate if a physician is not available.
If the death certificate is not completed or filled out properly, the document is usually rejected by the official public registrar of vital statistics in the jurisdiction the document is completed.[1][2]
The death certificate is a public record that can be accessed by the decedent's family, clinical researchers, lawyers, and insurance companies when there is litigation involved.
The death certificate should document the immediate cause of death, which can be an event, clinical condition, or disease process, which is unsuitable for the continuation of life.
The mechanism of death is not as important as the event or condition that precipitated the occurrence of death. The physiologic process of respiratory failure or cardiac failure does not explain the event preceding death. For this reason, clinicians are discouraged from using terminologies such as:
- Cardiac arrest
- Respiratory arrest
- Cardiopulmonary arrest
- Old age
The main purpose of death certification is for governmental agencies to compile vital statistics. This is used as official documentation of deaths and the causes of deaths. The death certificate is not intended to document the history of the present illness or the decedent’s clinical problems but rather to focus on the immediate cause of death.
The World Health Organization (WHO) has a mission statement that includes collecting and classification data on mortality. The collection and classification allow researchers to compare data from different countries. The United States is a signatory to this mission statement and follows the WHO's policies, procedures, and regulations.
The responsibility of collecting national data in the United States is vested in the hands of the National Center for Health Statistics (NCHS), which is a part of the Centers for Disease Control and Prevention (CDC). The responsibilities of the NCHS include but are not limited to the collection of national data within the United States on the causes of mortality.
For the NCHS to meet the WHO standards, the United States standard certificate of death is reviewed by NCHS periodically. Each state is required to comply with the rules and regulations set forth by the NCHS to receive federal funding.
In the United States, there are about 2.6 million annual deaths that are reported to the NCHS.
Each US state has specific requirements regarding when a death certificate must be filed. In Wisconsin, for example, the medical portion of the death certificate has to be completed within a maximum of 6 days from the time of death. It is considered a class 1 felony to willfully and knowingly falsify information on the death certificate.
In about 33% to 41% of cases, errors are made on the death certificate.[3][4][5] There is a significant over-representation of cardiovascular diseases as the primary cause of death.[6][7]
The most cited reasons for errors in death certification are:
- Inexperienced physician (physician in training)
- Lack of training by attending physicians
Studies suggest that organizing seminars and workshops that teach the process and procedure involved in death certification can greatly improve documentation accuracy.[8]
Some health care professionals are wary of signing a death certificate, believing that the signature might impose some legal responsibility on the practitioner.
The death certificate is a medical opinion regarding the cause of death based on the available information at the time of death. Lawsuits against health care practitioners for signing a death certificate are extremely rare, and when there is a lawsuit, the certifier of death is usually not held liable.
The death certificate can be subject to amendment.
Function
In the United States, there are similarities and variabilities in the function and content of the death certificate. Nevertheless, the death certificate in almost all the states conforms to the U.S. standard death certificate. There are 3 categories of information contained in the death certificate.[9]
Demographics and Statistics
- Name
- Age
- Social security number
- Race
- Gender
Method of Body Disposition
- Funeral home
- Crematorium
- Burial
- Cemetery site
Death Information
- Date of death
- Time of death
- Manner of death
The pronouncement is a terminology that denotes the time when an individual is found to be legally dead. In forensic or medical examiner (ME) cases, this might not always correspond to the actual time of death. An individual living alone or in a remote area might have been dead for days or rarely years before the pronouncement is made.
Pronouncement of Death
This is the specific date and time an individual is found to be legally dead. The declaration can be made by a physician, medical examiner, or coroner.[9]
Date and Time of Death
This is the date and time that an individual is thought to have actually died. This date and time might be actual or estimated. The date and time of death can be determined by a medical doctor, medical examiner, or coroner.
Cause of Death
This is the causal chain of events that ultimately leads to death.
The Immediate Cause of Death
This is the final event in the sequences of events that lead to death. This is what is filled in as the top diagnosis in the death certificate.
The Underlying Cause of Death
This is the initial event in the causal sequence that is the most remote from the time of death.
This information is filled in last, at the bottom of the death certificate.
Manner of Death
This is how death is classified based on the circumstances surrounding the death.
- Natural
- Accident
- Homicide
- Suicide
- Undetermined
Medical Certifier of Death
This is the individual responsible for completing the medical portion of the death certificate. This includes the time, date, cause, and manner of death.
Electronic Death Registry
The non-medical part of death certification can be filled out by the funeral director after the pronouncement of death. In the United States, most states file the non-medical portion using an electronic death filing system.
The electronic death filing system has several advantages in medical certification:
- Accuracy
- Timeliness
- Better surveillance of mortality
- Efficiency
In the electronic death filing, the funeral director fills in information related to the decedent's demographics, statistics, and bodily disposition. An appropriate medical certifier is then selected. In most states, online training or other forms of formal training is required before a health care practitioner can be a registered certifier of death. Most states have statutes that detail which individuals are certifiers of death. Once the non-medical part is completed, a “Fax Attestation for Medical Certification” is sent to the health care practitioner, who is then required to complete the medical part of the death certificate. The Fax Attestation for Medical Certification has a section that can only be completed by a medical certifier. After the completion of the form, the funeral director can verify the information before it is logged into the state registry. There are differences and variability in this process based on a state’s statute for death certificates.
Medical Certification of Death
Accuracy is the most important factor to be considered in the medical death certification. All dates should be indicated by day, month, and year. The time of death should be reported in a 24-hour clock format, military time. For example, if the time of death is 1 p.m., it should be recorded as 1300 on the death certificate.
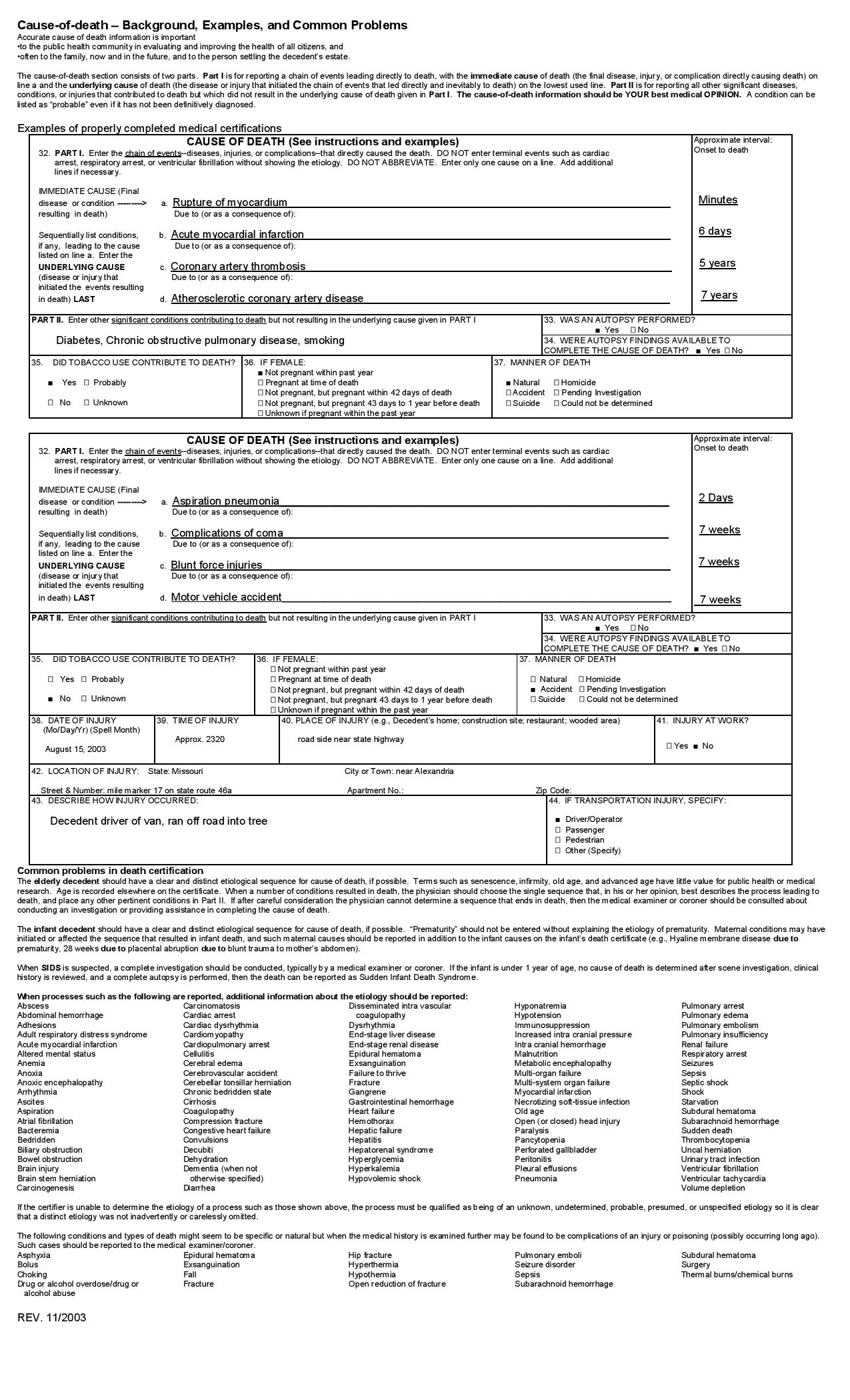
Part I
The cause of death section in the death certificate should be filled out as specifically as possible. Part I reports the causal events that lead to death and is made up of part Ia to part Id.
The most "immediate" or "recent" event that leads to death is listed in line a. The other conditions are listed in Line b to and then sequentially. The last and most remote condition leading to death is listed as the “underlying” cause of death.
All conditions that fall between the immediate and underlying cause of death are known as intermediate or intermediary. The approximate interval between the onset of each of the events and time of death should be listed in hours, days, weeks, or months.
Part II
All other diseases and injuries that may have contributed to death but did necessarily precipitate the cascade of events leading to death are listed in part II.
Examples of Completing a Death Certificate
Example 1
- Part I
- a. Pulmonary edema (2 days) due to or as a consequence of
- b. Anasarca (2 months) due to or as a consequence of
- c. Chronic renal failure (5 years) due to or as a consequence of
- d. Systemic lupus erythematosus (15 years)
- Part II
- Chronic obstructive pulmonary disease (20 years)
- The manner of death: natural
- Autopsy: yes/no
In this example, the immediate cause of death is pulmonary edema. Anasarca and chronic renal failure are the intermediate cause of death related to systemic lupus erythematosus, the underlying cause of death. The death certificate must be very specific. Edema has to specify the location: pulmonary edema. It is advisable to be as specific as possible when listing the cause of death. Abbreviations and acronyms are also best avoided.
Example 2
- Part I
- a. Fat embolism (2 hours) due to or as a consequence of
- b. Chronic tissue hypoxia (12 years) due to or as a consequence of
- c. Sickle cell anemia (12 years)
- Part II
- Moderate persistent asthma (7 years)
- The manner of death: natural
- Autopsy: yes/no
In this example, the immediate cause of death is a fat embolism. Chronic tissue hypoxia from sickle cell disease is a cause of chronic hypoxia that can cause fatty tissue to dislodge from the bone marrow. This is the intermediate cause of death. The underlying cause of death is sickle cell disease, which is the primary disease causing chronic hypoxia from abnormal hemoglobin with impaired oxygen-carrying capacity. The cause of death is what is required in the death certificate and not the mechanism. The mechanism of most death is usually cardiopulmonary arrest. It is not advisable to use this diagnosis in the death certificate as it does not specify the cause of death.
Issues of Concern
Special Cases
Injuries
Death can occur as a result of an injury sustained in the hospital or outside the hospital setting. Death related to injury has no statute of limitations. A patient developed overwhelming sepsis secondary to empyema and necrotizing pneumonia from a stab wound with a knife to the chest. Even though the immediate cause of death in this instance is overwhelming sepsis, the manner of death for medical-legal reasons is still homicide.
Hip fracture from falls, especially in elderly, frail patients, is very common. The presence of hip fracture can predispose patients to sepsis and a thromboembolic event that can ultimately cause death. If, as a sequela of a hip fracture from a fall, a patient later develops pulmonary embolism from prolonged immobilization, the manner of death in this instance will be an accident.
Even if an injury is listed only in part II of the death certificate, the non-natural cause, in this instance, the accident prevails and is used as a determinant of the manner of death. The cause of death on a death certificate can be changed or amended, if needed, based on the specific circumstances related to the death. If death or demise occurs as a result of injury or poisoning, non-natural causes are listed as the manner of death.
Example
- Part I
- a. Sepsis and septic shock
- b. Empyema and necrotizing pneumonia
- c. Knife wounds to the chest
- Part II
- Type 2 diabetes
- The manner of death: homicide
- Autopsy: yes/no
Place of Injury
The place of injury should be specified in the death certificate. The place of injury might also be the place where the pronouncement of death is made. For example, the place of injury can be listed as a shopping mall, fast food restaurant, hotel, or resort.
Location of injury should include the street name, zip code, county where the injury happened, or where the decedent is found.
Injury at Work
This is usually a yes or no. This part is important to fill in, especially if there is an employer/employee relationship.
How the Injury Happened
This should be described precisely, for example, "skiing on a steep slope, lost control, and hit a tree;" or "driving a car, struck from behind, and ejected from a vehicle."
In most jurisdictions, if the cause of death is not natural, the medical examiner or coroner is responsible for completing the death certificate.
Acute and Chronic Substance Abuse
Acute and chronic consumption of illicit drugs or alcohol can cause death. Chronic alcohol abuse can cause pancreatitis, seizure from alcohol withdrawal, or hepatic cirrhosis. Bacterial endocarditis can develop from chronic intravenous drug abuse. Oral carcinoma can develop from tobacco chewing or chronic obstructive lung disease from smoking. Death from a chronic condition is classified as natural.
On the contrary, death resulting from acute drug toxicity, for example, overdose with cocaine, phencyclidine, or opiate, is classified as suicide or accident. Classification of death as suicide as a manner of death depends on whether there is evidence to support self-harm or injury. When a death occurs as a result of therapeutic intervention, for example, overwhelming sepsis from bone marrow suppression secondary to the initiation of chemotherapy, the manner of death in this instance is natural.
Physician-Assisted Suicide or Euthanasia
In some states, this form of death is classified as “other” or “unclassified.”
Terminal Events
Events like electromechanical dissociation, ventricular fibrillation, pulseless ventricular tachycardia, asystole, respiratory arrest, or respiratory failure are common and nonspecific. It is recommended not to use these terminologies in the death certificate.[9][10]
Amending a Death Certificate
As at the time of certifying death, the certifier fills in information in the death certificate based on the information available at that time. In other words, this is the best medical opinion at the time of completing the death certificate. Most states have provisions in their laws to amend the death certificate. If an autopsy is requested and will be completed within a reasonable time, it is best to wait for the result of the autopsy before completing the death certificate. Some institutions have policies to ensure that the pathologist performing the autopsy consults with the medical certifier of death, and both assume responsibilities for signing the death certificate. This is to prevent discordance between the autopsy report and the cause of death certification.
The medical examiner or coroner can amend the death certificate should additional information comes up.
Clinical Significance
The clinical significance of a death certificate cannot be overemphasized. The 2 most important events in life are birth and death. Legal existence is from the time of birth to death. Records of death and birth are part of the vital statistics that governments collect to plan for food, housing, health care delivery, and education.
The statistical analysis of the cause of death forms the backbone of vital statistics, which are used by governments for planning and implementing health care policy.
Other Issues
Brain Death
Brain death is defined as the irreversible cessation of all functions of the brain activities, including the brain stem. Traditionally, the concept of death has always been historically linked to the cessation of heartbeat, but with advances in technology, including mechanical ventilation and inotropic support therapy, an individual might have a beating heart but an irreversible loss of brain functions.[11][12]
Brain death declaration is a wholly clinical diagnosis. Practitioners are not required to perform another test if 2 tests for brain stem function and an apnea test are conclusive for brain death.
Determination of Brain Death
History and physical examination that point to a clear-cut etiology of brain death includes anoxic brain injury, fulminant hepatic encephalopathy, or severe head injury.[13][14][15]
Exclusion of other causes of coma:
- Severe electrolyte abnormalities
- Ingestion of drug or toxins that are potential central nervous system depressant, for example, neuromuscular blocking agents, benzodiazepines
- Hypothermia with core body temperature less than 32 C
- Encephalopathy associated with hepatic, renal failure, or hyperosmolar coma
- Severe hypophosphatemia
A detailed neurological examination that includes:
- Examination for spontaneous movement, decerebrate and decorticate posturing
- Stimulation with noxious stimuli
- Absence of pupillary response to consensual light
- Absent oculocephalic, corneal, cough, and gag reflexes on stimulation
- Absence of oculovestibular reflex on instillation of water
Apnea Test
An apnea test can then be performed once the neurological assessment is complete.[16][17]
The patient must meet the following criteria prior to the initiation of the apnea test:
- The core body temperature should be greater than 36.5 C or 97 F
- Euvolemic status with normal blood pressure
- The partial pressure of carbon dioxide in the blood PC02 be equal to or greater than 45 mm Hg.
- The normal partial pressure of oxygen; clinician will preoxygenate the patient to 200 mm Hg.
After satisfaction of the above prerequisite, the apnea test can then be conducted in the following manner:
- Connect the patient to 100% via a T tube or a cannula after disconnecting the patient from mechanical ventilation.
- Watch the patient closely for any spontaneous breaths.
- Take blood samples for blood gas analysis at 4 to 5 minutes intervals twice (8 to 10 minutes).
In the absence of spontaneous respiratory and the PC02 is greater than 60 mm Hg or has risen about 20 mm Hg above baseline, the apnea test is positive.
If the patient develops spontaneous breaths during the test, the test is considered negative.
The patient should be connected back to mechanical ventilation if:
- Systolic blood pressure falls below 90 mm Hg. In children, if the systolic blood pressure is below the threshold for age
- Significant desaturation on pulse oximetry[17]
- Presence of arrhythmia or dysrhythmia
The healthcare provider should draw and analyze an arterial blood gas sample.
- If PCO2 is greater than 60 mm Hg or PCO increase is by more than 20 mm Hg over baseline normal PCO2, the apnea test result is considered to be positive, meaning it supports the clinical diagnosis of brain death.
- If PCO2 is less than 60 mm Hg and PCO increase is less than 20 mm Hg over baseline normal PCO2, the result is considered to be indeterminate.
- In this case, a confirmatory test can be considered.
Confirmatory Test
Confirmatory test for brain death includes:
- Angiography might be conventional, magnetic resonance imaging (MRI), or computed tomography (CT); brain death is demonstrated by an absence of intracerebral filling at the level of the circle of Willis and or the level of the carotid bifurcation.
- Electroencephalography: Brain death can be confirmed by demonstrating the absence of electrical activities
- Nuclear brain scanning
Cerebral Scintigraphy (Technetium Tc 9m Exametazime)
Brain death is demonstrated by the absence of uptake of radioscope by brain parenchyma.
Transcranial Doppler ultrasonography flow studies will show small peaks during the systolic phase and no flow during the diastolic phase. This is indicative of a high vascular resistance to blow flow from increased intracranial pressure associated with brain death.
Brain Death in Children
Brain death determination in pediatrics is a clinical diagnosis. There is not enough data on brain death on an infant less than 37 weeks of age. Therefore, the recommendations listed below do not apply to infants less than 37 weeks of age.
Prior to the initiation of brain death protocol, hypothermia, hypotension, and electrolyte abnormalities should be treated as in adults. Medication that will interfere with the apnea test or neurological examination should be discontinued. The physical examination should be performed by 2 physicians. The apnea test can be performed by one physician.
Observation Period
The 2 examinations are separated by an observation period of:
- Twenty-four hours; for newborn up to 30 days
- Twelve hours for infants and children older than 30 days to 18 years[18]
The first examination determines if the child has met all the required criteria for brain death. The second examination is to confirm brain death based on the fact that the condition is irreversible.
The assessment of neurological status after cardiopulmonary resuscitation or other severe injuries to the brain should be deferred for about 24 hours or longer if there are inconsistencies in the neurological examination.
The protocol for the apnea test is the same as in adults.
Certification of Brain Death
A single physician with institutional privileges can certify brain death. If the question of organ donation arises, the state of New York requires that the brain death certification be done by the physician who attended to the patient at the time of death and another physician. Both physicians should confirm that the clinical evaluation meets an accepted medical standard.
All the processes and phases involved in the brain death determination should be properly documented:
- The cause of irreversibility of coma and unresponsiveness
- The absence of motor response to noxious stimuli
- The absence of brainstem reflexes in 2 separate examinations separated by at least 6 hours.
- The absence of respiration with pCO greater than 60 mm Hg
- The rationale and justification for ancillary studies and confirmatory test
A death certificate can be issued after the test is completed. Once a patient is declared brain dead, mechanical ventilation can be discontinued. However, the family should be treated with sensitivity and respect. Reasonable accommodation should be made for the families to come to terms with brain death. Institutional policies are usually put in place to address the issues and concerns family members might have during the process of certification of death based on brain death criteria.[19]