The skull is a compact structure that covers and protects the brain and facial organs.[1][2] It is in a complex anatomical relationship with many craniofacial organs and associated tissues, each of which has a different embryological origin and performs different functions. Therefore, skull lesions may be of the bone origin or may have originated from the adjacent brain, scalp, or craniofacial organs. Although the definitive diagnosis of a skull lesion usually requires histopathologic evaluation, radiologic imaging plays an important role in limiting the diagnosis list and establishing the management plan. Radiologic evaluation should be based upon clinical factors such as the patient's age, gender, trauma history, and medical history, which play a decisive role in the differential diagnosis. The main radiological features guiding the diagnostic approach include the location, number, type of margin, vascular configuration, and radiolucency of the lesion, as well as the attenuation/signal characteristics, presence or absence of remodeling/destruction, and presence or absence of accompanying soft tissue involvement.[3][4]
While radiography has been the principal imaging modality of skull lesions until recent years, today it is largely replaced by computed tomography (CT) and magnetic resonance imaging (MRI). Thanks to its high spatial resolution, CT is excellent at precisely localizing the skull lesion and defining its extensions. And owing to its high contrast resolution, MRI is the preferred method for the assessment of diploic involvement and lesion texture.[5][6] Bone scintigraphy has a considerably high sensitivity in detecting bone lesions. However, its low specificity usually necessitates further evaluation using other radiologic or nuclear medicine imaging techniques.[7] In this review, after a brief anatomical description of the skull, the imaging methods used in the diagnosis of skull pathologies and the main strengths and drawbacks of these methods will be discussed.
Anatomy
The skull, also referred to as the cranium, is one of the hardest and most durable structures of the human body. It consists of two parts, one of which is neurocranium encasing the brain, and the other is viscerocranium forming the facial skeleton. The neurocranium is a large neural cavity formed by the tight engagement of the calvarium (cranial vault) and the skull base with each other. The calvarium is made up of flat bones, including frontal bones, parietal bones, the squamous portions of the temporal bones, and the interparietal portion of the occipital bone. Although the calvarium is a monolayer structure at birth, the diploic space emerges in around the fourth year giving the calvarium its characteristic double-layer form. The skull base forms the floor of the neurocranium on which the brain sits smoothly.[1][2] It consists of frontal, ethmoid, sphenoid, temporal, and occipital bones and is home to many holes and fissures that allow passage of multiple neural and vascular structures. The skull base comprises anterior, central, and posterior compartments. The petrous temporal bone that separates the central and posterior compartments is sometimes referred to as a posterolateral skull base.[3] The viscerocranium is located on the anterior aspect of the neurocranium. It consists of 14 facial bones that are shaped and articulated per the numerous complex functions they carry out.[2] In addition to protecting the facial organs that perform critical sensory functions, the viscerocranium has serious tasks such as ensuring the entry of vital substances such as oxygen, water, and nutrients into the body.[8]
Plain Films
In today's clinical practice, cross-sectional imaging methods such as computed tomogram (CT) and magnetic resonance imaging (MRI) have largely replaced skull radiography, and the use of plain films has been significantly limited. However, it is still regarded as the first-line imaging method in cases of suspected skull lesions and is sometimes used to obtain a diagnostic clue.[5][6] Currently, radiography is mostly used to evaluate the surgically implanted material such as shunts, cochlear implants, intrathecal catheters, and deep brain stimulators. The most commonly used imaging study for this purpose is the shunt series consisting of radiographs of the shunt components obtained in at least 2 planes. The shunt series is applied to investigate the type of shunt, the localization of the proximal and distal catheter tips, and the cause(s) of shunt dysfunction.[9] Another current indication for skull radiography is the skeletal survey, which is conducted for various purposes such as suspected child abuse, skeletal dysplasias, multiple myeloma, eosinophilic granuloma, and Paget disease.[10]
Computed Tomography
The skull imaging study has a long list of indications that can practically be classified as trauma, benign or malignant focal skull lesions, and systemic pathologies affecting the skull. CT is the principal modality in imaging of the traumatic skull lesions since it not only provides perfect visualization of cortical bone but also offers a very short imaging time allowing immediate intervention before brain damage or death. Besides, it is regarded as the most accurate method in the detection of a cerebrospinal fluid leak. Multidetector computed tomography (MDCT) allows rapid volumetric image data acquisition, and with the use of sub-millimetric slice thickness, it permits multiplanar reformations (MPR) and 3-dimensional (3D) reconstructions.[8][11][12] 2D axial and coronal images are more sensitive and reliable than 3D reconstructions in the detection and detailed evaluation of skull fractures. However, since 3D imaging provides a global view of the fracture pattern and has significant contributions in preoperative planning, it is widely requested by surgeons. For this reason, 3D reconstructions should be added to the imaging study in skull fracture cases, especially in those detected in the maxillofacial area.[8] CT and MRI are complementary modalities for imaging focal skull lesions, and both are performed in most cases, especially in skull base lesions. CT is the ideal method for evaluating the inner and outer tables of cortical bone, detecting bone lysis or sclerosis, precise localization of the lesion, and visualizing the mineralized part(s) of the lesion.[3][4][5][6][13][14][15][16] Currently, non-contrast CT of the whole skull without further contrast-enhanced CT examination is recommended in cases where MRI is included in the imaging study. In the context of limiting exposure to ionizing radiation, contrast-enhanced CT examination is indicated only in the case of contraindications to MRI[15]. In the evaluation of skull lesions, certain CT findings guide the diagnosis and significantly shorten the differential diagnosis list. For example, while a regular cortical expansion and remodeling of the bone with smooth thinning suggest benign pathologies that exhibit a slow-growing pattern, permeative and destructive changes strongly support the presence of a rapidly progressing process such as aggressive inflammation or malignity.[16] And certain pathologies such as fibrous dysplasia, hemangiomas, and Paget disease offer highly specific CT findings. Fibrous dysplasia characteristically appears as an intradiploic expansile mass showing ground-glass matrix on CT, while in most cases, it appears misleadingly aggressive on MRI. Hemangiomas are seen on CT as well-circumscribed intradiploic osteolytic lesions showing sunburst pattern of coarse trabeculae with spicules and/or radiations. Thanks to this characteristic appearance, hemangiomas can be accurately diagnosed by CT without further MRI examination. Likewise, Paget disease also shows characteristic CT findings, including bone expansion, cortical thickening, and trabecular coarsening.[4][5]
Magnetic Resonance
In imaging of the skull, CT and MRI usually complement each other in terms of their strengths and disadvantages and are often used in combination. MRI is superior in imaging the diploic area and demonstrating bone marrow involvement. It can detect a lesion in the diploic area even before it changes bone architecture, and can shed light on the content of the lesion. Another strength of MRI is that it provides the opportunity to evaluate the associated soft tissue component accurately and precisely define scalp involvement and intracranial/extracranial extension.[3][4][5][6]
The skull MRI sequence profile shows some differences as compared with that of the head MRI. First, a skull MRI study should include more fat-saturated imaging sequences compared to brain imaging because of the considerably high adipose tissue content of the structures surrounding the skull, especially the skull base. Second, the study should always include non-contrast T1-weighted images without fat saturation since it is the best sequence in evaluating possible marrow replacement by a tumor or edema. While most physicians are usually persistent in requesting contrast-enhanced MRI for skull imaging, it should be taken into consideration that gadolinium may obscure lesions in case the appropriate technique is not performed. Therefore, the administration of contrast material should be justified according to the suspected pathology.[15]
On MRI, intact inner and outer tables appear as signal-free areas, and the diploic space displays variable signal intensity depending on patient age. While most of the skull lesions are hypointense on T1-weighted and hyperintense on T2-weighted images, the signal characteristics of the lesions show a wide range of variations according to their cellular content.[13] In general, due to their high water content, inflammatory lesions, as well as low-grade benign tumors, display a high T2 signal. On the other hand, as a result of their high cellular content, malignant neoplasms exhibit intermediate to low signal intensity on T2-weighted images. Besides, the apparent diffusion coefficient (ADC) values within malignant lesions are decreased as compared with healthy tissues.[16]
Ultrasonography
Ultrasonography (US) is not a useful imaging modality for evaluating bone pathologies. The use of the US in the skull region is not intended for bone lesions, but the evaluation of brain parenchyma and cerebral vascular structures through the acoustic windows obtained between sutures or through the relatively low mineralized skull in newborns.[17][18][19]
Nuclear Medicine
Bone scintigraphy is a diagnostic nuclear medicine imaging method that evaluates active bone formation related to malignant and benign diseases, as well as physiological processes.[7] Its excellent sensitivity makes it useful in screening for a wide variety of bone diseases, including primary and metastatic tumors, bone infection, and Paget disease. However, its considerably low specificity limits the use of the method alone.[20] Therefore, complementary tests, including MRI, CT, bone scintigraphy, and positron emission tomography (PET-CT), are often used together in varying combinations.[21]
Almost all bone scintigraphy examinations are performed in patients with a diagnosis of malignancy, especially breast, prostate, and lung cancer. And the method plays an indispensable role in the staging and treatment of malignant tumors. Bone metastases usually appear as scattered foci of increased uptake, which are different from each other in terms of size and shape on radionuclide bone imaging.[20] Whole-body fluorodeoxyglucose positron emission tomography (FDG-PET) is another imaging method used for the detection of primary and metastatic tumors. The method is based on depicting the increase in glucose consumption of the malignant tissue and shown to be superior in detecting osteolytic metastases compared to bone-affine radiotracers. FDG-PET has gained intense popularity in metastasis screening and has increasingly been used in recent years.[7] Finally, integrated PET-MRI systems developed in recent years are now available. However, the role of this young technology in oncological imaging is still at the research stage. Fortunately, good results have been reported in some studies evaluating PET-MRI in the context of head and neck malignancies.[22]
Angiography
The use of angiography in imaging studies of skull lesions is extremely limited. The most common application area of angiography in skull lesions is for preoperative embolization of the brain tumors affecting the skull, especially meningiomas. Preoperative embolization is applied to reduce intraoperative blood loss, facilitate tumor resection, and shorten the operation time. It is especially useful in skull base tumors and tumors with very high vascularity.[23] Angiography, although extremely rare, is also used in the evaluation of arteriovenous fistula and arteriovenous malformation cases associated with skull involvement.[24][25]
Clinical Significance
The skull is at the target of many pathological processes, including congenital, inflammatory, neoplastic, and traumatic pathologies. Most skull lesions are asymptomatic and are incidentally discovered during CT or MRI performed for other reasons. Benign tumors such as hemangioma and osteoma are the most commonly encountered lesions in this region.[3] For practical purposes, skull lesions can be handled under two main headings: calvarial and skull base lesions.
Calvarial Lesions
Osteoma, hemangioma, fibrous dysplasia, eosinophilic granuloma, epidermoid and dermoid cysts, and Paget disease are the most commonly encountered benign lesions in the calvarium. Among these, hemangiomas, eosinophilic granulomas, and epidermoid and dermoid cysts are seen as lucent lesions while the remaining are sclerotic on radiography and CT. The most common two malign calvarial lesions are metastases and multiple myeloma. While the lung, breast, prostate, kidney, and thyroid are the most common origins of skull metastases in adults, a metastatic lesion in the skull of a child primarily suggest neuroblastoma or sarcoma as the origin. Skull metastases may be either lytic, sclerotic, or mixed; however, they mostly present as multiple lytic foci with accompanying soft-tissue components. Single and expansive lytic lesions are highly suggestive of thyroid or renal neoplasm metastasis. Metastases of prostate carcinoma are typically osteosclerotic. Multiple myelomas, the most common primary bone tumor of adulthood, characteristically show punched-out lytic lesions with sharp non-sclerotic margins that may coalesce to form larger lytic areas in the skull.[3][4][5][6]
Skull Base Lesions
The skull base has an extremely complex anatomy and is not favorable for clinical examination. Therefore, radiologic imaging is an indispensable part of skull base evaluation. Inflammatory and neoplastic lesions of this region are the two main groups of pathology that must be primarily addressed. The main inflammatory lesions of the skull base are mucoceles and cranial complications of sinusitis and mastoiditis. Mucocele refers to the expansion of an air cell by mucus accumulation caused by the obstruction of the sinus ostium. In cases of mucocele, it is necessary to determine the cause of obstruction and to evaluate intraorbital/intracranial expansion, on CT and/or MRI. Sinusitis and mastoiditis may cause several intracranial infectious complications such as meningitis, cerebritis, ventriculitis, epidural abscess, subdural empyema, or skull base osteomyelitis. An initial non-contrast CT of the skull base and paranasal sinuses/temporal bone, followed by MRI with and without contrast administration, should be performed in case any of the mentioned complications are suspected. The neoplastic involvement profile of the skull base is no different from that of the calvarium, except for chordoma and chondrosarcoma, both of which have a well-known tendency for the skull base.[14][15][16]
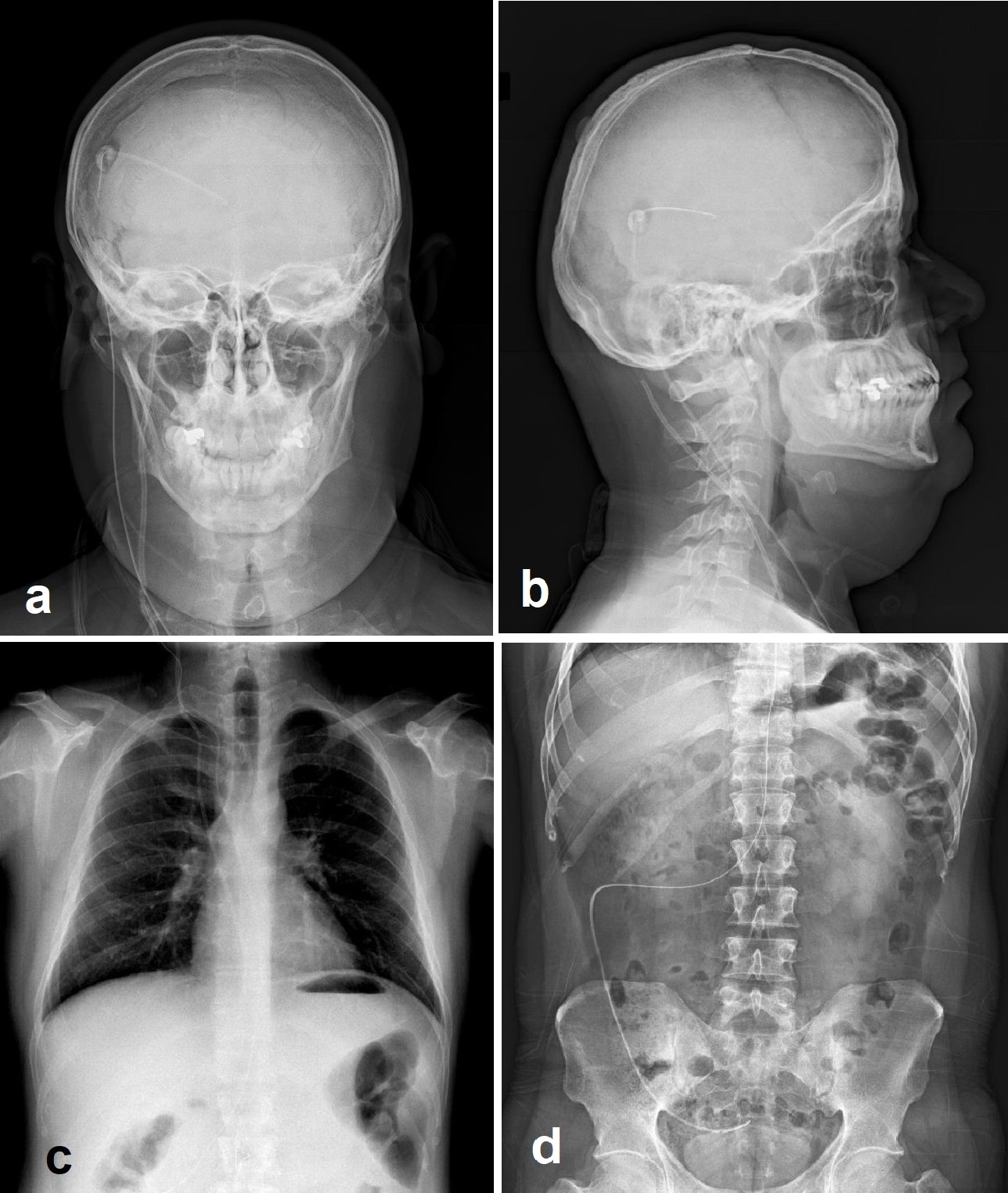
(Click Image to Enlarge)
Shunt series including biplanar head (a and b), anteroposterior chest (c) and anteroposterior abdominal (d) radiographs demonstrating the ventriculoperitoneal shunt catheter throughout its course.
Contributed by Meltem Özdemir, MD
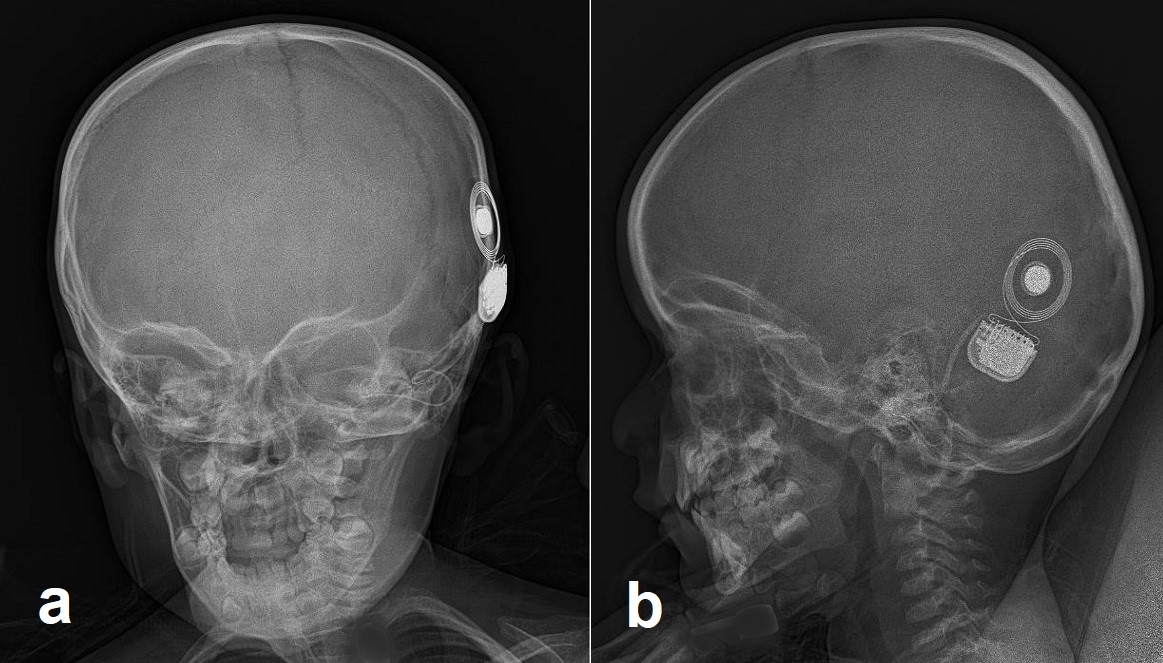
(Click Image to Enlarge)
Anteroposterior (a) and lateral (b) skull radiographs showing cochlear implant components within the left inner ear and on the left temporal bone.
Contributed by Meltem Özdemir, MD
Jin SW,Sim KB,Kim SD, Development and Growth of the Normal Cranial Vault : An Embryologic Review. Journal of Korean Neurosurgical Society. 2016 May;
[PubMed PMID: 27226848]
Van den Wyngaert T,Strobel K,Kampen WU,Kuwert T,van der Bruggen W,Mohan HK,Gnanasegaran G,Delgado-Bolton R,Weber WA,Beheshti M,Langsteger W,Giammarile F,Mottaghy FM,Paycha F, The EANM practice guidelines for bone scintigraphy. European journal of nuclear medicine and molecular imaging. 2016 Aug;
[PubMed PMID: 27262701]
Vogl TJ,Harth M,Siebenhandl P, Different imaging techniques in the head and neck: Assets and drawbacks. World journal of radiology. 2010 Jun 28;
[PubMed PMID: 21160634]
Caricato A,Pitoni S,Montini L,Bocci MG,Annetta P,Antonelli M, Echography in brain imaging in intensive care unit: State of the art. World journal of radiology. 2014 Sep 28;
[PubMed PMID: 25276307]
Love C,Din AS,Tomas MB,Kalapparambath TP,Palestro CJ, Radionuclide bone imaging: an illustrative review. Radiographics : a review publication of the Radiological Society of North America, Inc. 2003 Mar-Apr;
[PubMed PMID: 12640151]
Hines JP,Howard BE,Hoxworth JM,Lal D, Positive and Negative Predictive Value of PET-CT in Skull Base Lesions: Case Series and Systematic Literature Review. Journal of neurological surgery reports. 2016 Mar;
[PubMed PMID: 26937333]
Queiroz MA,Hüllner M,Kuhn F,Huber G,Meerwein C,Kollias S,von Schulthess G,Veit-Haibach P, PET/MRI and PET/CT in follow-up of head and neck cancer patients. European journal of nuclear medicine and molecular imaging. 2014 Jun;
[PubMed PMID: 24577950]
Manaka H,Sakata K,Tatezuki J,Shinohara T,Shimohigoshi W,Yamamoto T, Safety and Efficacy of Preoperative Embolization in Patients with Meningioma. Journal of neurological surgery. Part B, Skull base. 2018 Oct;
[PubMed PMID: 30210986]
Kim MS,Oh CW,Han DH,Kwon OK,Jung HW,Han MH, Intraosseous dural arteriovenous fistula of the skull base associated with hearing loss. Case report. Journal of neurosurgery. 2002 May;
[PubMed PMID: 12005406]