Continuing Education Activity
Hypertensive encephalopathy is a hypertensive emergency highlighted by mental status changes due to severely elevated blood pressure. The condition requires prompt but meticulous treatment. An abrupt blood pressure increase can exceed the cerebral blood vessels' autoregulatory capacity, disrupt the blood-brain barrier, and produce brain edema. Patients may experience severe headaches, altered mental status, visual disturbances, and seizures. Coma and death may result if this condition is not managed promptly.
This activity for healthcare professionals enhances learners' proficiency in evaluating and managing hypertensive encephalopathy. Valuable insights will be gained that will enable learners to collaborate effectively with an interprofessional team caring for affected individuals.
Objectives:
Identify the signs and symptoms suggestive of hypertensive encephalopathy.
Create a clinically appropriate diagnostic plan for a patient suspected to have hypertensive encephalopathy.
Compare the various hypertensive encephalopathy management options and determine an individualized treatment plan for a patient diagnosed with this condition.
Collaborate and coordinate effectively with the interprofessional team in formulating short- and long-term care plans for patients with hypertensive encephalopathy.
Introduction
The internal carotid and vertebral arteries give rise to the brain's blood supply. The arterial branches lie in the subarachnoid space.
The internal carotid arteries originate in the neck from the common carotid arteries, ascend to the skull base, and enter the middle cranial fossa through the carotid canals. The carotid arteries pass anteromedially toward the cavernous sinus on the sphenoid body. The anterior and middle cerebral arteries are the internal carotid arteries' terminal branches, comprising the brain's anterior circulation. The anterior communicating artery bridges the right and left anterior cerebral arteries.
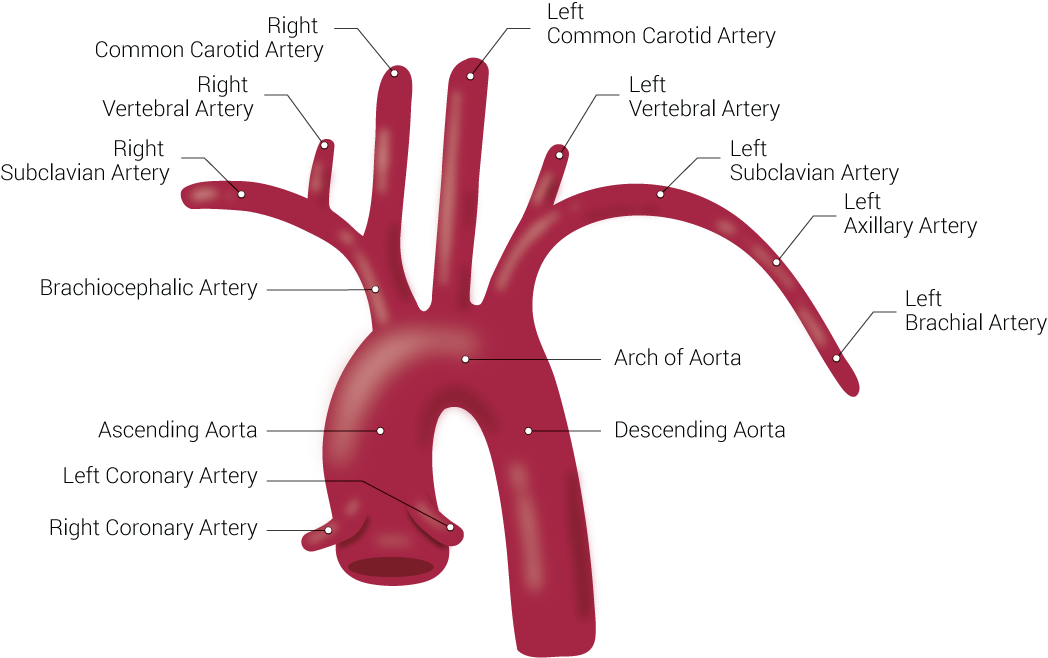
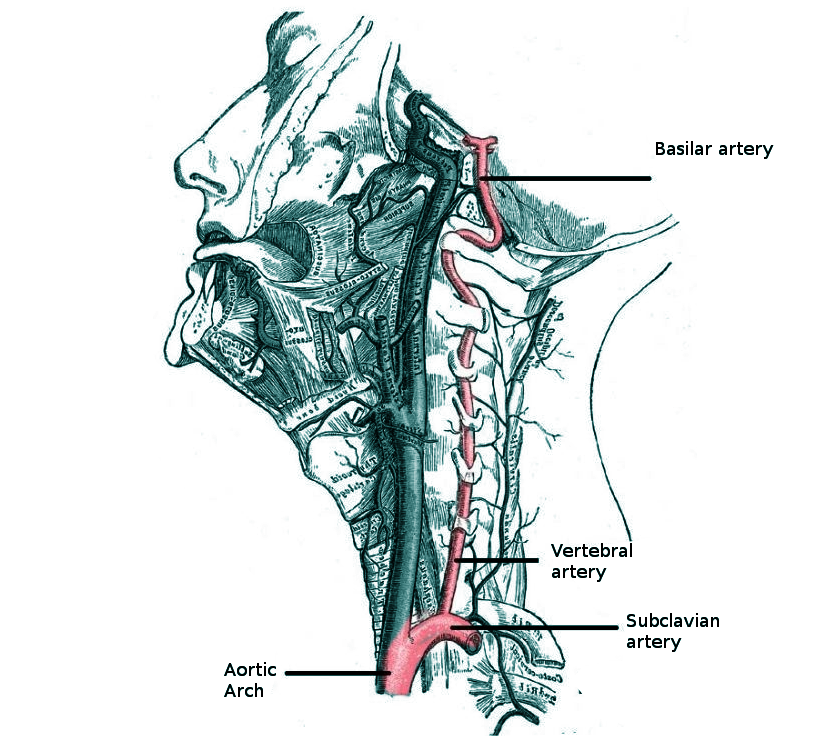
The vertebral arteries are the first branches of the first part of the subclavian arteries, arising from the root of the neck (see Image. Branches of the Aorta). The superior vertebral artery segments run through the C1 to C6 transverse foramina. Suboccipital branches enter the dura and arachnoid and traverse the foramen magnum (see Image. Vertebral Artery Anatomy in the Neck Region). The basilar artery arises from the fusion of the right and left vertebral arteries at the caudal pontine margin. This artery then ascends to the superior pontine border and bifurcates into 2 posterior cerebral arteries. The vertebrobasilar arterial system comprises the brain's posterior circulation.
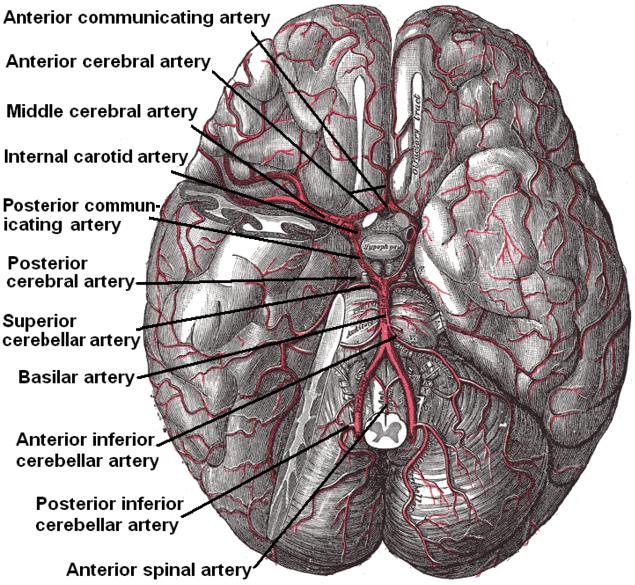
The posterior communicating arteries connect the internal carotid and posterior cerebral arteries. Connecting the anterior and posterior brain circulations completes the cerebral arterial circle of Willis (see Image. Arterial Circulation of the Brain).
The dural venous sinuses drain the superficial and deep veins of the brain. These venous sinuses empty into the internal jugular veins. The veins on the brain's superolateral aspect drain into the superior sagittal sinus. Their posteroinferior counterparts empty into the straight, superior petrosal, and transverse sinuses.
The blood-brain barrier (BBB) separates the peripheral and central nervous system (CNS) circulation. Endothelial cells connected by tight junctions are the main BBB components. The tight junctions hinder paracellular transport that can contaminate the cerebral vasculature. Other cells comprising the BBB include the astrocytes, pericytes, and microglia. Astrocyte endfeet (podocytes) form the glia limitans, a membrane that further hinders solute movement across the BBB. Without membrane transporters, only small or lipid-soluble particles can enter the CNS circulation.[38]
Angiotensin receptors make the BBB sensitive to the effects of the renin-aldosterone-angiotensin system. These receptors mediate endocrine regulation of water and electrolyte balance, vascular resistance, oxidative stress, neuroinflammation, and brain homeostasis.[39]
A hypertensive emergency is a life-threatening condition. Target-organ damage occurs due to markedly elevated blood pressure.[1] Hypertensive emergencies may arise in patients with or without a history of preexisting hypertension.[2] Pulmonary edema, cardiac ischemic events, acute renal failure, aortic dissection, eclampsia, retinopathy, encephalopathy, and intracranial hemorrhage may develop as a result of hypertension-related organ injury.[3]
Hypertensive encephalopathy is an uncommon hypertensive emergency manifestation. Signs and symptoms include severe headaches, nausea, vomiting, visual disturbances, seizures, and mental status changes.[4] The condition is diagnosed after ruling out other CNS dysfunction etiologies. Lowering the blood pressure dramatically improves symptoms. Early recognition of hypertensive encephalopathy can result in favorable clinical outcomes as prompt treatment can reverse the symptoms of this condition.[5]
Etiology
Inadequately controlled primary hypertension is the most common cause of hypertensive encephalopathy. Secondary causes of hypertension, such as kidney disorders and adrenal tumors, can also predispose to this condition. Autoregulatory mechanisms normally enable the brain to maintain adequate cerebral perfusion pressure (CPP), altering arterial and arteriolar resistance in response to physiological changes.[1] Steep blood pressure elevation can overwhelm these mechanisms, leading to vascular wall damage, BBB disruption, and plasma, red blood cell, and macromolecule exudation.[2]
Hypertensive encephalopathy shares many clinical features with other syndromes giving rise to cerebral edema, such as posterior reversible encephalopathy syndrome (PRES), hypertensive brainstem encephalopathy, and eclampsia. Evaluation for underlying causes like renal disease, sympathomimetic (eg, amphetamines and cocaine) consumption, adverse effects of drugs like immunosuppressive agents, and pregnancy-induced hypertensive states should be considered if a patient is not known to have primary hypertension.
Epidemiology
In the United States, approximately 50% of the adult population has some degree of hypertension.[3] Hypertensive emergencies account for a small percentage (less than 2%) of hypertensive presentations in emergency departments.[4] Hypertensive encephalopathy specifically accounts for 15% of the hypertensive emergencies seen.[5][6] Hypertensive encephalopathy has been implicated in the rise in hospitalizations in the US from 2000 to 2011. The dramatic increase in hypertensive encephalopathy incidence does not only reflect a true epidemiologic change but also evolving coding and billing practices.[7]
Pathophysiology
Normally, the brain sustains blood flow within a narrow perfusion pressure range without being affected by systemic arterial pressure fluctuations. The CPP ranges from 50 to 150 mm Hg in healthy individuals, while the mean arterial pressure (MAP) lies normally between 60 and 160 mm Hg. CPP cannot be directly measured but may be calculated by subtracting intracranial pressure (ICP) from MAP (CPP = MAP - ICP).[8] Autoregulation-induced cerebral blood flow alterations involve diverse mechanisms, encompassing neurogenic, myogenic, endothelial, and metabolic responses.
Cerebral arteriolar vasoconstriction occurs with MAP elevation. Conversely, MAP reduction is accompanied by arteriolar dilation to keep the CPP constant. This adaptive process maintains adequate brain perfusion despite systemic blood pressure changes. However, steep, sudden arterial pressure increases can overwhelm this autoregulatory mechanism due to the arterioles' limited constricting ability. Elevated intracerebral blood pressure causes a BBB breach, consequently leaking capillary fluid into the brain parenchyma. Cerebral edema develops, thus increasing the ICP, damaging the neurons, and producing neurologic deficits. Altered mentation, visual deficits, and seizures are some of the known manifestations of hypertensive encephalopathy.
Chronic hypertension induces the cerebral vasculature to undergo adaptations, such as arteriolar hypertrophy, to allow for a higher autoregulatory range. Lowering the blood pressure too quickly in these patients can produce cerebral ischemia at a higher MAP compared to normotensive patients.
In previously normotensive patients, acute hypertensive episodes may induce hypertensive encephalopathy at diastolic blood pressures as low as 100 mm Hg. This scenario may be seen in patients with eclampsia or receiving cytotoxic and immunosuppressive therapies.[9][10] These conditions have been hypothesized to directly elicit a toxic effect on the vascular endothelium that leads to BBB dysfunction.
History and Physical
Hypertensive emergencies can arise in the preclinical and clinical settings and rapidly progress without prompt intervention. A quick primary survey must be performed to assess and address the patient's airway, breathing, circulation, disability, and exposure. The blood pressure and cardiac and neurologic functions must be continuously monitored after administering initial treatment. The secondary survey and diagnostic studies may be initiated after stabilizing the patient and other emergencies have been ruled out.
On history, patients may initially complain of headaches, visual blurring, nausea, vomiting, lethargy, and neck pain for hours or days. Patients are commonly aged 40 or older with preexisting primary hypertension. These individuals may also have a history of antihypertensive treatment nonadherence.[11] An inciting factor like trauma, emotional or physical stress, and emergence from anesthesia may also be reported. Patients may be taken or referred for consultation for symptom persistence or the development of new ones, such as altered mental status and seizures.
Acute hypertension in patients younger than 40 usually has a secondary cause, such as illicit drug use, pregnancy, or chronic kidney disease. The diagnostic workup must include tests for underlying disorders that possibly precipitated the event.[12]
Acute hypertensive episodes are systemic conditions and thus may damage other organs like the heart and kidneys. In many cases, encephalopathy may be accompanied by cardiorespiratory manifestations, such as angina and dyspnea, regardless of age.
The blood pressure cutoffs set by the American College of Cardiology and American Heart Association (ACC/AHA) 2017 guidelines for hypertension stage 1 are 130 mm Hg systolic and 80 mm Hg diastolic. Meanwhile, the 8th Joint National Committee (JNC 8) defined hypertension as having 2 or more blood pressure measurements of 130 mm Hg systolic or higher or 90 mm Hg diastolic or higher within 2 years.[40] Clinically, patients with a systolic blood pressure greater than 180 mm Hg or diastolic blood pressure greater than 120 mm Hg without any symptoms are diagnosed with hypertensive urgency. However, the development of acute organ damage, as in hypertensive encephalopathy, makes the condition a hypertensive emergency.
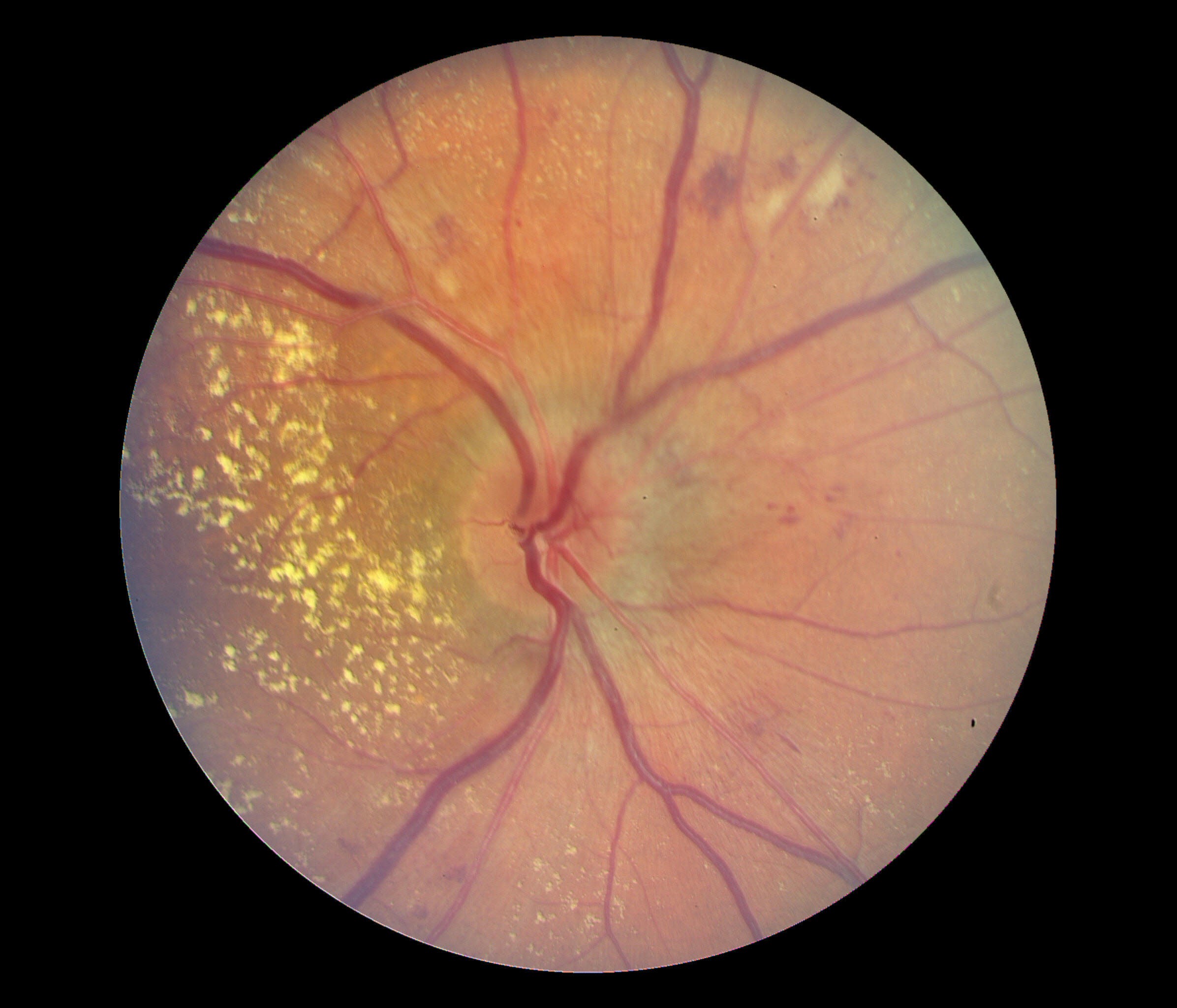
Regardless of the presentation, a thorough physical examination with detailed cardiovascular and neurologic assessments should be performed on patients with elevated systolic or diastolic pressure per the ACC/AHA or JNC 8 guidelines. Cardiac involvement may manifest with extra heart sounds, elevated jugular venous pressure, bipedal edema, or rales.[18] Eye involvement may be examined by funduscopy, which may show retinal hemorrhages, macular edema, fibrinous exudates, and cotton wool spots (see Image. Macular Edema Associated with Hypertensive Retinopathy).[19]
The neurological examination may reveal altered sensorium and focal deficits, especially after a seizure episode. Transient and mild sensorimotor weakness may accompany acute hypertension. Sudden loss of consciousness and persistence of lateralizing signs may indicate a hemorrhagic stroke, which can develop if acute hypertension is not promptly addressed. Suspect a subarachnoid hemorrhage if patients report intense headaches with or without auras.
Acute renal damage, if present, may manifest with decreasing urine output, sudden behavioral changes, breathing difficulty, and seizures due to uremia. Uremia may compound neurologic damage arising from abrupt blood pressure elevation.
Evaluation
Acute hypertension that remains untreated can lead to seizures, cerebral hemorrhage, coma, and death.[13] A diagnosis is made in individuals with severely elevated blood pressure and neurologic symptoms after ruling out other conditions that present similarly. Ischemic stroke and intracerebral hemorrhage must be excluded in these patients because these conditions are treated differently and not managed primarily or exclusively by lowering blood pressure.
Vital Signs and Cardiac Monitoring
Patients should be hooked to a cardiac and vital signs monitor. An electrocardiogram (ECG) is a good initial cardiac function test. Patients with longstanding hypertension may have signs of cardiac hypertrophy, such as tall or wide QRS waves and ST deviations. Without previous ECG tracings for comparison, myocardial infarction must be ruled out by obtaining cardiac enzyme levels.
A peaked T wave, prolonged PR interval, ST depression, wide QRS, and flattened P wave may indicate hyperkalemia if acute kidney damage is present. The ECG may also show ischemic changes in young patients or individuals without preexisting hypertension in the presence of an inciting factor, such as substance abuse, preeclampsia, or toxic kidney injury.
The blood pressure must be monitored closely, especially after initiating antihypertensive treatment. Abrupt changes in the heart and respiratory rates may be signs of beginning cardiorespiratory distress secondary to cardiac damage. The oxygen saturation must be continuously monitored in patients with dyspnea.
Pregnant patients may need to be monitored by tocometry. This modality can detect fetal compromise in a laboring patient.
Laboratory Studies
Initial blood tests may include a complete blood count, coagulation profile, and complete metabolic panel. The test results are usually within normal limits or only slightly deranged if acute hypertension is managed promptly and the patient has no preexisting condition. Abnormal test results may be due to an underlying condition or hypertensive end-organ damage. Hypertensive encephalopathy is less likely if these initial blood tests yield abnormal results.
Normochromic, normocytic anemia often occurs in chronic kidney disease but not acute kidney injury. Uremia arising from either condition may cause platelet dysfunction, prolonging bleeding time. The metabolic panel may reveal hyponatremia and elevation of creatinine, blood urea nitrogen, and potassium levels. The arterial blood gases in patients with uremia typically show acidosis.
Pregnancy-related hypovolemia may also lower the hematocrit and hemoglobin levels. Severe cases of pregnancy-induced hypertension may progress to the syndrome of hemolysis, elevated liver enzymes, and low platelets or "HELLP syndrome." The condition may lead to disseminated intravascular coagulation.
Cardiac enzymes must be obtained for individuals suspected to have cardiac involvement. Elevated creatine kinase-myocardial band, troponin I, and new-onset abnormal ECG patterns signify acute cardiac damage.
Low urine output (<20 mL/h), red blood cell cast formation, and dysmorphia may signify acute glomerulonephritis. Pregnancy-induced hypertension often produces proteinuria. A urine toxicology test may be useful in evaluating acute hypertension in a previously healthy young individual.
Imaging Studies
Brain computed tomography (CT) without contrast is a good initial imaging test for individuals presenting with a sudden behavioral change, altered sensorium, or focal neurological deficits. Hypertensive encephalopathy may not always exhibit radiological abnormalities, though CT may not be as sensitive as magnetic resonance imaging (MRI) in identifying brain edema regions. Still, CT imaging is usually more readily available, takes less time to perform, and can rule out many intracranial lesions. This modality can identify ischemic stroke or intracerebral hemorrhage.
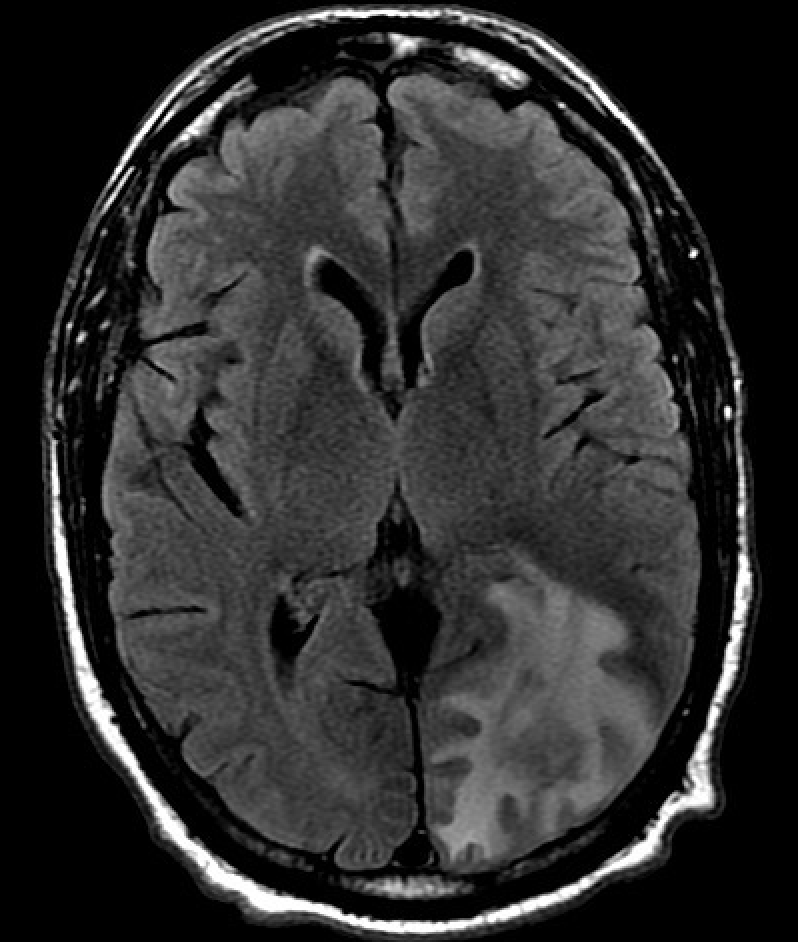
T2-weighted MRI can localize cerebral edema regions that may arise from hypertensive encephalopathy. PRES appears as bilateral white matter edema in the posterior cerebral hemispheres (see Image. Posterior Reversible Encephalopathy Syndrome on Magnetic Resonance Imaging). Hypertensive brainstem encephalopathy may feature punctuate or confluent areas of increased signal.[14] The distribution of cerebral edema is localized, occurring in the parietooccipital regions in PRES and pontine region in cases of hypertensive brainstem encephalopathy.
PRES may also involve the frontal lobe and atypical regions such as the basal ganglia, periventricular white matter, thalami, brainstem, and spinal cord.[15] Hemorrhage is a recognized complication of PRES and occurs in approximately 15% of patients.[16] PRES is usually associated with hypertensive encephalopathy. However, the condition may also be found in normotensive individuals predisposed to vascular injuries, such as people with autoimmune disease or preeclampsia or on immunosuppressive drugs.[17]
Lumbar puncture is not required to diagnose hypertensive encephalopathy. However, this procedure may be performed when a patient is evaluated for other causes of encephalopathy, such as a CNS infection. PRES may manifest with modestly elevated protein levels without pleocytosis, ie, an albuminocytologic dissociation.[18]
A chest x-ray may be indicated in patients with dyspnea or suspected cardiac involvement. Findings may include an enlarged cardiac shadow and bilateral pulmonary infiltrates.
A pelvic ultrasound is warranted in patients with preeclampsia to assess if the fetus may be safely delivered. Pregnancy termination is the best treatment for pregnancy-induced hypertension.
Treatment / Management
While the initial diagnosis and treatment of a hypertensive emergency may occur in the emergency department, definitive treatment is usually performed in an intensive care unit. Management involves administering antihypertensive drug therapy to reduce systolic blood pressure by no more than 25% within the initial hour, followed by a gradual blood pressure reduction to 160/100 mm Hg over the next 2 to 6 hours if stable.[19] The blood pressure should be cautiously brought to normal within 24 to 48 hours.[20]
Overaggressive hypertensive therapy can cause the MAP to fall below the brain's hypertensive-adapted autoregulatory range, increasing the risk of stroke. In contrast, careful blood pressure reduction minimizes the risk of ischemic neurologic events and allows for the healing of brain vasculature. Ischemic complications in other organs may also be prevented by gradual blood pressure lowering.[21][22] Exceptions to conservative blood pressure reduction include ischemic stroke, intracerebral hemorrhage, and aortic dissection.
Parenteral antihypertensive agents should be used initially. Oral antihypertensive agents must be avoided in the initial treatment phase because these agents cannot be titrated and have a slower onset of action. Parenteral antihypertensive drugs commonly used for this condition include nicardipine, labetalol, esmolol, fenoldopam, sodium nitroprusside, and clevidipine. These medications allow a more controlled reduction in blood pressure. Fenoldopam, a dopamine receptor agonist, may be recommended in patients with renal impairment as it has demonstrated a renoprotective effect.[23] Clonidine should be avoided as it can cause CNS depression.
The initial intravenous therapy is tapered and discontinued after reaching the target blood pressure. Oral antihypertensives may be started 8 to 24 hours after discontinuing intravenous antihypertensives.
In patients with pregnancy-induced hypertension, antihypertensive therapies are chosen based on safety evidence on fetal and placental health. The blood pressure must be controlled for as long as possible to allow the fetus to develop closer to term. However, the presence of hypertensive emergency manifestations like seizures warrants immediate delivery regardless of gestational age.
Antiseizure medication may be prescribed and continued until symptoms and neuroimaging findings improve. The antiseizure medication may be tapered after 1 to 2 weeks, as seizure recurrence after encephalopathy resolution is rare.[24] Drug selection for seizure treatment may depend on the presence of other conditions, such as pregnancy or renal function impairment.
Patients with PRES and hypertension are treated with antihypertensive drugs similarly to those with hypertensive encephalopathy. The main goal of treating PRES is to address the underlying cause. Management may involve reducing blood pressure, administering antiepileptics, discontinuing or changing medications, and correcting electrolyte imbalances. Timely delivery must be ensured in pregnant women. Immunosuppressive drug dosages may be reduced or discontinued in patients who develop PRES symptoms.
Patients on a new immunosuppressive drug must be evaluated by neuroimaging if PRES symptoms recur. Prior medications associated with an encephalopathic episode must be avoided in these individuals. Fluid therapy overload, MAP greater than 25% of baseline, and creatinine values greater than 1.8 mg/dL have been found to increase the risk of PRES in patients receiving cytotoxic and immunosuppressive drugs.[25]
Differential Diagnosis
The differential diagnosis of hypertensive encephalopathy includes the following conditions:
- Ischemic or hemorrhagic stroke
- Intracerebral hemorrhage
- Intracranial tumor
- Occult brain trauma
- Acute toxic metabolic encephalopathy
- Hepatic encephalopathy
- Central venous thrombosis
A thorough clinical and diagnostic investigation can distinguish these conditions from hypertensive encephalopathy.
Treatment Planning
Parenteral Antihypertensives
- Nicardipine is a dihydropyridine calcium channel blocker with a selective arterial vasodilator effect. The initial dose is 5 mg/hour, and the maximum is 15 mg/hour. The onset of action is fast with IV infusion. Nicardipine achieves a rapid, dose-dependent increase in plasma concentrations within the initial 2 hours following the start of infusion. Plasma concentration decreases rapidly upon infusion discontinuation. The drug's effect decreases by nearly 50% in the first 1 to 2 hours, then wanes gradually over approximately 50 hours.
- Labetalol is an α- and β-adrenergic receptor blocker. This drug may be administered as an intravenous bolus or infusion. A 10 to 20-mg bolus is given initially over 1 to 2 minutes, followed by subsequent boluses of 10 to 80 mg intravenously every 10 minutes to a maximum total dose of 300 mg daily. Labetalol may also be given as a continuous infusion of 0.5 to 2 mg/min and titrated up to 10 mg/min or until the desired hemodynamics are achieved. Intravenous labetalol's onset of action is less than 5 minutes, with peak effects occurring after 5 to 10 minutes. The medication's half-life is approximately 6 hours. Labetalol should not be used without prior adequate α-blockade in patients with hyperadrenergic states, eg, cocaine-induced hypertension.
- Fenoldopam is a selective dopamine-1 agonist. This drug decreases peripheral vascular resistance and increases renal blood flow. The initial infusion dose is 0.1 mcg/kg per minute, with the dose titrated at 15-minute intervals, depending on patient response. A maximum infusion rate of 1.6 mcg/kg per minute has been reported in clinical trials. Fenoldopam is especially beneficial in patients with kidney disease. However, the medication increases intraocular pressure and should be used cautiously in patients with glaucoma.[23]
- Clevidipine is a dihydropyridine calcium channel blocker with an elimination half-life of 5 to 15 minutes. The initial dose is 1 mg/hour, and the maximum is 21 mg/hour. This agent is ultra-short-acting, has a rapid onset of action, and is usually associated with mild or no reflex tachycardia.[26]
- Sodium nitroprusside is a nitrovasodilator that releases nitrous oxide to induce peripheral vasodilation through direct action on arteriolar and venous smooth muscles. Peripheral resistance subsequently abates. The initial dose is 0.25 to 0.5 mcg/kg/min, and the usual maximum dose is 8 to 10 mcg/kg/min. Sodium nitroprusside is not a first-line drug, as it may cause cyanide toxicity.[27] The risk of cyanide toxicity is higher if the medication is used at a high infusion rate for a prolonged period (greater than 24 to 48 hours) or if the patient has renal impairment. This agent may also cause reflex tachycardia, increased ICP, and decreased renal blood flow.
Prognosis
Hypertensive encephalopathy is often reversed by prompt but gradual blood pressure reduction. PRES was initially described as a condition with good outcomes. However, mortality has been reported in 19% of patients diagnosed with PRES, while functional impairments of varying degrees have been reported in 44%.[28][29] The prognosis for PRES varies depending on whether other comorbidities are present. Factors associated with poor outcomes include neoplastic etiology, severe encephalopathy, delayed treatment of the underlying cause, coagulopathy, and hyperglycemia.
A recent study demonstrated favorable outcomes in individuals with PRES associated with preeclampsia and eclampsia.[30] Imaging characteristics linked to unfavorable outcomes include corpus callosum involvement, extensive cerebral edema, worsening imaging severity, hemorrhage, subarachnoid hemorrhage, and restricted diffusion on imaging.[31] Continued vigilance regarding home hypertension management is necessary once patients are released from the hospital. Antihypertensive treatment noncompliance increases the risk of another hypertensive crisis.
Complications
Failure or delayed treatment of a hypertensive emergency may result in renal failure, retinopathy, myocardial infarction, and stroke. Brain edema can progress and lead to status epilepticus, coma, or death if the blood pressure continues to be elevated in patients with encephalopathy. On the other hand, aggressive blood pressure reduction can lead to ischemic end-organ damage, especially in patients with an adapted autoregulatory mechanism due to chronic hypertension. Patients with risk factors such as autoimmune diseases, renal failure, sickle cell crisis, and hypertensive crisis are at risk for recurrent PRES.
Consultations
The management of hypertensive encephalopathy may involve several specialists, depending on the severity of the condition and the patient's specific needs. These specialists may include the following:
- Intensivist
- Cardiologist
- Neurologist
- Radiologist
These specialists' expertise is particularly valuable if the presentation is complex.
Deterrence and Patient Education
Patients should be educated about treatment compliance and advised home monitoring of blood pressure to reduce the risk of hypertensive crises. Moreover, dietary sodium and cholesterol should be reduced. Weight management, a balanced diet, and regular exercise should be encouraged, as healthy lifestyle habits can help control blood pressure.
Pearls and Other Issues
The most important points to remember in diagnosing and managing hypertensive encephalopathy are the following:
- The symptoms of hypertensive encephalopathy are insidious. Headache, nausea, and vomiting gradually worsen with time and may be followed by nonlocalizing neurologic symptoms. In contrast, ischemic stroke and intracerebral hemorrhage may present with abrupt and focal neurologic symptoms.
- Prompt and controlled blood pressure reduction is essential to prevent further brain damage. However, aggressive blood pressure lowering should be balanced with the risk of hypoperfusion.
- Neuroimaging, such as brain CT or MRI, is crucial for confirming the diagnosis of hypertensive encephalopathy and ruling out other potential causes of neurological symptoms. CT is not sensitive enough to detect brain edema but is essential in ruling out other causes of altered mental status.
- Hypertensive encephalopathy symptoms can mimic other neurological emergencies such as cardiovascular accidents and seizures. Clinical assessment and neuroimaging are vital for accurate diagnosis and appropriate management.
- The most commonly used first-choice antihypertensive drug for this condition is nicardipine.
- Hypertensive encephalopathy is often a consequence of uncontrolled hypertension, but clinicians should also consider and investigate underlying causes such as renal disease or endocrine disorders. Addressing the hypertensive crisis' underlying issues may help prevent recurrences.
- Continuous monitoring for complications like seizures, cerebral edema, and multiorgan dysfunction is essential in the acute management of hypertensive encephalopathy.
- Blood pressure targets may vary based on symptom severity and the presence of end-organ damage. Individualized treatment plans are necessary, and careful monitoring is crucial.
- After the acute phase, patients with hypertensive encephalopathy should have regular follow-up appointments to monitor blood pressure, assess for recurrence, and adjust medications as needed.
- Patient education is critical in preventing hypertensive encephalopathy recurrence. The importance of medication adherence, lifestyle modifications, and regular blood pressure monitoring must be emphasized.
Notably, individual patient management may vary based on specific clinical circumstances.
Enhancing Healthcare Team Outcomes
As this condition is treated in an intensive care unit, the patient's medical treatment will be managed primarily by an intensivist with consultations from other specialists, such as a cardiologist, neurologist, and radiologist, as dictated by organ involvement.
Encouraging patients to develop a medical home with their primary care provider is important as this practice contributes to better patient outcomes. Once discharged from the hospital, follow-up with a primary care provider is essential to encourage continued blood pressure monitoring and hypertension management. A pharmacy consultation to determine the appropriate agents and dosing is beneficial. The pharmacist, nursing staff, and primary care provider should educate the patient and their family about the importance of medication compliance and instructions on using antihypertensive medications. When counseling patients, the primary care team should emphasize the importance of lifestyle changes such as exercise, smoking cessation, and healthy eating habits.
Consultation with a social worker may be needed for individuals without primary care options. Unfortunately, a high percentage of this patient population does not remain compliant with antihypertensive medications and frequently seeks management in the emergency room. Healthcare outcomes are improved when hypertension is managed as an outpatient with their primary care provider rather than in an emergency department. Patient outcomes will improve when the interprofessional healthcare team functions collaboratively and not in "silos."