Continuing Education Activity
Macrocytic anemia refers to macrocytosis (mean corpuscular volume (MCV) greater than 100 fL) in the setting of anemia (hemoglobin less than 12 g/dL or hematocrit (Hct) less than 36% in nonpregnant females, hemoglobin less than 11 g/dL in pregnant females, or hemoglobin less than 13 g/dL or Hct less than 41% in males). It is divided into two forms, megaloblastic (hypersegmented neutrophils) and non-megaloblastic. The megaloblastic form is due to impaired DNA synthesis from folate and/or vitamin B12 deficiencies, while the non-megaloblastic moiety occurs from multiple mechanisms.There are many etiologies for macrocytic anemia, decreased hemoglobin with elevated mean corpuscular volume (>100 fL), several of which are easily treatable and some that that are life-threatening. This activity describes the evaluation, diagnosis, and management of macrocytic anemia and highlights the role of team-based interprofessional care for affected patients.
Objectives:
- Identify the epidemiology of macrocytic anemia.
- Summarize the evaluation of a patient with macrocytic anemia.
- Outline the treatment and management options available for macrocytic anemia.
- Describe interprofessional team strategies for improving care coordination and communication to advance treatment of macrocytic anemia and improve patient outcomes.
Introduction
Macrocytic anemia refers to macrocytosis (mean corpuscular volume (MCV) greater than 100 fL) in the setting of anemia (hemoglobin less than 12 g/dL or hematocrit (Hct) less than 36% in nonpregnant females, hemoglobin less than 11 g/dL in pregnant females, or hemoglobin less than 13 g/dL or Hct less than 41% in males). It is divided into two forms, megaloblastic (hypersegmented neutrophils) and non-megaloblastic. The megaloblastic form is due to impaired DNA synthesis from folate and/or vitamin B12 deficiencies, while the non-megaloblastic moiety occurs from multiple mechanisms.[1][2]
Etiology
Megaloblastic anemia occurs from deficiencies in folic acid and vitamin B12. Folate deficiency is due to diminished intake (alcohol abuse or malnutrition), increased consumption (hemolysis or pregnancy), malabsorption (familial, gastric bypass, or medications like cholestyramine or metformin). Vitamin B12 deficiency appears in diminished intake (malnutrition), malabsorptive states (atrophic gastritis either autoimmune or non-autoimmune from Helicobacter pylori or Zollinger-Ellison syndrome, Diphyllobothrium tapeworm infection, gastric bypass, ileal resection), or the presence of antagonists (nitrous oxide). Drugs that impair DNA synthesis are folic acid analogs (ex. methotrexate, trimethoprim-sulfamethoxazole), nucleic acid analogs (5-fluorouracil, zidovudine), and others (hydroxyurea, pentamidine, phenytoin, pyrimethamine, sulfasalazine, triamterene).
Non-megaloblastic anemia, the absence of hypersegmented neutrophils, occurs in a variety of settings. Benign conditions are alcohol consumption (RBC toxicity), hereditary spherocytosis (impaired volume regulation increases red cell size), hypothyroidism and liver disease (due to lipid deposition in the cell membrane), and marked reticulocytosis from states of excess RBC consumption such as hemolysis or turnover in pregnancy or primary bone marrow disease (reticulocytes are larger than the average RBCs).
Some cases of macrocytosis are normal variants associated with a genetic predisposition or found in infants, patients with Down syndrome, and pregnant women. Others are spurious findings include hyperglycemia concentrates the blood, and when diluted, the RBCs swell with volume, leukocytosis and paraproteinemia increase sample turbidity for overestimates of RBC size, or operator error from occlusion of microscope aperture or sample left out at room temperature too long.[3][4]
Epidemiology
Macrocytosis affects 2% to 4% of the population, 60% of whom have anemia. Alcohol use accounts for the majority, followed by deficiencies in folate and vitamin B12 and medications. Autoimmune causes are more common in middle-aged women. Hypothyroidism and primary bone marrow disease account for more cases of macrocytic anemia in older patients. The prevalence of vitamin B12 deficiency increases in patients older than 60 years.
Mild macrocytic anemia (MCV 100 fL to 110 fL) is more likely to be caused by benign conditions compared to marked macrocytic anemia (MCV more than 110 fL), the latter of which is due to primary bone marrow disease or megaloblastic anemia from folate or vitamin B12 deficiencies.[5][6]
Pathophysiology
The equation for mean corpuscular volume [MCV (fL) = Hct (%) X 10 / RBC (106/microgram)] explains how macrocytic anemia represents large red blood cells (RBCs) in comparison to total amount. Folate and vitamin B12 are necessary for RBC nucleic acid synthesis. Without DNA or RNA, erythropoiesis is ineffective with nuclear/cytoplasmic asynchrony, resulting in larger erythrogenic precursors with abnormal nuclei (ex. hypersegmentation) but normal cytoplasms. Anemia occurring in the presence of macrocytosis and hypersegmented neutrophils is known as megaloblastic anemia. The absence of hypersegmented neutrophils characterizes non-megaloblastic anemia. This occurs from mechanisms discussed earlier: abnormalities involving the RBC membrane, excess erythrocytic precursors, increased cell volume, or RBC toxicity.
Daily folate needs are 100 to 200 micrograms, and the body can absorb 400 micrograms/day. Healthy patients have stores for 4 months. Folate is largely absorbed in the small bowel. In comparison, daily vitamin B12 requirements are one microgram, and the body can absorb 2 to 3 micrograms/day. Most patients have several years of B12 stores. Vitamin B12 is absorbed in the ileum when bound by an intrinsic factor (IF), a protein produced by the gastric parietal cells. Abnormalities in these cascades cause deficiencies in folate or vitamin B12, respectively.[7]
Histopathology
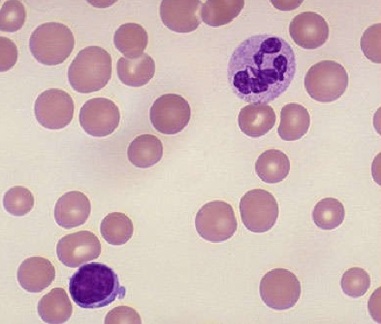
Macrocytic anemia that is megaloblastic contains hypersegmented neutrophils and macro-ovalocytes on peripheral blood smear (PBS) (figure "macrocytic anemia"). Anisocytosis and poikilocytosis are not uncommon due to ineffective erythropoiesis. Bone marrow evaluation will demonstrate hypercellularity with abnormal maturation and proliferation of myeloid cell lines, particularly the erythroid lineage.
Nonmegaloblastic macrocytic anemia will not have hypersegmented neutrophils; instead, its PBS will show round macrocytes or macro reticulocytes, in addition to other cells representative of the underlying etiology (acanthocytes from liver disease, myeloid dysplasia or immaturity in primary bone marrow disease, polychromatophilic RBCs with reticulocytosis, schistocytes from hemolysis, or spherocytes in inherited hemolytic anemias such as hereditary spherocytosis).
History and Physical
The presentations of macrocytic anemia are dependent on the underlying cause. Patients with vitamin B12 deficiency complain of mood disturbances and neurologic symptoms like loss of balance, memory loss, paresthesias, peripheral neuropathy. The remainder of symptoms is specific to the underlying cause (constitutional symptoms from primary bone marrow disease, gastrointestinal upset from enteral malabsorption, or hypoactive metabolism from hypothyroidism). Folate deficiency has common features except neuropsychiatric complaints. Prior surgeries include a gastric bypass for weight loss or ileal resection for colonic pathologies. Family or personal medical histories reveal autoimmune diseases or hemolytic anemias. Certain medical conditions require at-risk medications. Review of dietary intake reveals excessive alcohol consumption or limited food choices (“tea and toast”).
Physical exam may reveal nonspecific anemia findings (conjunctival pallor), neurologic deficits if vitamin B12 deficient (impaired proprioception or vibration, positive Romberg sign), and stigmata of underlying diseases (glossitis from autoimmune atrophic gastritis, hepatosplenomegaly from familial hemolytic anemias, hypopigmentation from vitiligo, or jaundice and spider angiomata from alcohol abuse).
Evaluation
Initial evaluation of macrocytic anemia includes a thorough history and physical followed by limited labs (PBS, reticulocyte count, and serum B12). Pure RBC indices will underestimate the presence of macrocytosis by 30% because MCV represents the mean distribution curve of all RBCs and fails to identify smaller macrocytes. If the PBS is normal, no megaloblastic RBCs, order additional testing for liver and thyroid diseases (aminotransferases and thyroid stimulating hormone), the most common causes of non-megaloblastic anemia. If there are megaloblastic RBCs on PBS, check the reticulocyte count: less than 1% indicates underproduction, while greater than 2% is associated with hyperproliferation due to hemolysis or hemorrhage (commence hemolytic anemia work-up). If hyperproliferative, look at the B12 level. Values less than 100 pg/mL indicate deficiency. Order RBC folate level (not serum folate due to lack of sensitivity) for B12 above 400 pg/mL; low levels indicate folate deficiency and normal ones may need further investigation with bone marrow evaluation. Measure homocysteine and methylmalonic acid (MMA) in patients with B12 100 pg/mL to 400 pg/mL; these are biochemical compounds important in pathways involving cell metabolism and use folate and vitamin B12 as cofactors. Both or MMA only are elevated in vitamin B12 deficiency; homocysteine is elevated in folate deficiency. Normal values may warrant hematology consultation for bone marrow studies. Specialist consults are recommended in patients with abnormal myeloid morphology on PBS (disordered immaturity, hypo-granulated or hypo-segmented neutrophils, or additional cytopenias).
Work-up for specific causes of megaloblastic anemia should be based on presentation. Antibodies for intrinsic factor or parietal cells are indicative of pernicious anemia. The Schilling test, once used to measure vitamin B12 uptake before and after administration of intrinsic factor, has fallen out of favor. [3][8]
Treatment / Management
Treat macrocytic anemia by replacing folate or vitamin B12 and targeting the underlying cause. Give folic acid orally, 1 mg to 5 mg daily, and encourage diets with foods rich in folate (fortified cereals, leafy vegetables). Patients who are taking folate antimetabolites or pregnant women (especially those with a history of neural tube defects or taking antiepileptics) should take daily supplements to prevent deficiencies. It is important to not overlook vitamin B12 deficiency as a cause for macrocytic anemia, treatment of folate deficiency but not vitamin B12 deficiency will resolve the anemia but not the neurologic effects. Prescribe 1000 micrograms oral vitamin B12 daily for 1 month followed by 125 to 250 micrograms daily or administer 1000 micrograms intramuscular B12 every week for 4 weeks then monthly to replace vitamin B12 stores, the latter of which is preferred for patients with pernicious anemia or altered gastrointestinal anatomy. Clinicians may prescribe empiric folate supplementation (400 micrograms to 1 g/day) in patients receiving vitamin B12 replacement. Reticulocytosis will improve within 1 to 2 weeks, and anemia should resolve after 4 to 8 weeks. There is no need to monitor RBC indices or recheck folate or vitamin B12 levels and their metabolites during active treatment, though some physicians check yearly complete blood counts in patients taking long-term vitamin B12 therapy. Neurologic symptoms from vitamin B12 deficiency take longer. Macrocytosis related to alcohol use resolves with abstinence. Other non-megaloblastic anemias improve when the underlying conditions are treated.
In other instances, macrocytosis is indicative of medical compliance (ex. methotrexate or zidovudine) and does not need additional management beyond supplements to prevent anemia.[9][10]
Differential Diagnosis
- Folate deficiency anemia
- Anemia due to liver disease
- Hypothyroidism
- Myelodysplastic syndrome
- Alcoholism
Prognosis
With early identification and treatment of underlying cause, the prognosis for macrocytic anemia is excellent. Specialist referral is rarely needed unless anemia is resistant to therapy or there is evidence of underlying myelodysplasia or leukemia.
Complications
Patients with chronic megaloblastic anemia from vitamin B12 deficiency can develop permanent neurologic damage referred to as subacute combined neurodegeneration. Patients will have gait ataxia, memory loss, peripheral neuropathy, and psychiatric disturbances. Patients with macrocytic anemia from underlying conditions will experience complications of their respective diseases.
Deterrence and Patient Education
Macrocytic anemia is a special blood disorder in which the body is not able to form enough blood cells because it lacks necessary nutrients. Some patients do not eat enough foods with these nutrients (folate or vitamin B12), while others cannot absorb it or have an underlying condition that makes it difficult for the body to keep up with its needs. Patients may feel tired, have memory or mood disturbances, or notice tingling in the arms and legs. Physicians can diagnose the anemia during an office visit and lab work. Treatment involves addressing the underlying cause and nutrient supplementation.
Pearls and Other Issues
With early identification and treatment of underlying cause, the prognosis for macrocytic anemia is excellent. Specialist referral is rarely needed unless anemia is resistant to therapy or there is evidence of underlying myelodysplasia or leukemia. This anemia is the most underestimated of all forms and physicians should not hesitate to treat due to its unique side effects.
Enhancing Healthcare Team Outcomes
Today, healthcare workers encounter many cases of macrocytic anemia than in the past. Further, as the population ages, many more cases of macrocytic anemia are likely to be seen in the future. The other thing of note is that there are many causes of macrocytic anemia including medications; thus the management of these patients is an interprofessional. It is important to educate the patient that some of the more common causes of macrocytic anemia include deficiency of folate and cobalamin. In addition, several reverse transcriptase inhibitors used to treat HIV can also cause macrocytic anemia and hence the pharmacist should encourage the patient to regular blood tests. Another common cause of macrocytic anemia is alcohol abuse; however, with abstinence, this anemia is rapidly corrected. Finally, patients should be educated about foods that are rich in folate and cobalamin.[11][12]
Outcomes
When the cause of the macrocytic anemia is dietary, the condition can be reversed with dietary changes. For those who fail to comply with diet, they are at risk for anemia related cardiac complications, neurological damage, and defects in fetal development. When the cause is a malignancy, the prognosis is guarded. [13][14]