A vast network of nerve tracts in the central nervous system (CNS) which spans the cerebral cortex, brainstem, cerebellum, and spinal cord control the initiation and modulation of movements. The nerves in the CNS which carry the impulses for movement are known as upper motor neurons (UMN). The primary tract which carries signals for voluntary movement is known as the pyramidal tract. The pyramidal tract divides further into the corticospinal tract and the corticobulbar tract. Injury or lesions to UMN’s are common because of the vast areas covered by the motor neuron pathways. UMN lesions are designated as any damage to the motor neurons that reside above nuclei of cranial nerves or the anterior horn cells of the spinal cord. Damage to UMN’s leads to a characteristic set of clinical symptoms known as the upper motor neuron syndrome. These symptoms can include weakness, spasticity, clonus, and hyperreflexia. UMN’s lesions have a wide differential diagnosis which ranges from cerebrovascular accidents, traumatic brain injury, malignancy, infections, inflammatory disorders, neurodegenerative disorders, and metabolic disorders.
Structure and Function
Upper motor neurons are first-order neurons which are responsible for carrying the electrical impulses that initiate and modulate movement. Various descending UMN tracts are responsible for the coordination of movement. The major UMN tract that initiates voluntary movement is the pyramidal tract. The pyramidal tract provides a direct pathway between the cerebral cortex and the spinal cord, in contrast with extra-pyramidal tracts which provide indirect pathways for the coordination of movement. The pyramidal tract divides into the corticospinal tract and the corticobulbar tract. Corticospinal tract fibers synapse with spinal nerves while corticobulbar fibers synapse with cranial nerves. The cell bodies of the pyramidal tract concentrate around the motor area of the cerebral cortex. In general, the motor areas of the left and right hemispheres will innervate the musculature on the contralateral side of the body. The motor areas are somatotopically organized. This means that control of facial musculature is situated on the most lateral area of the cerebral hemisphere while control of the legs takes a more medial position. The mapping of different parts of the motor area for specific body parts is called the cortical homunculus.[1][2]
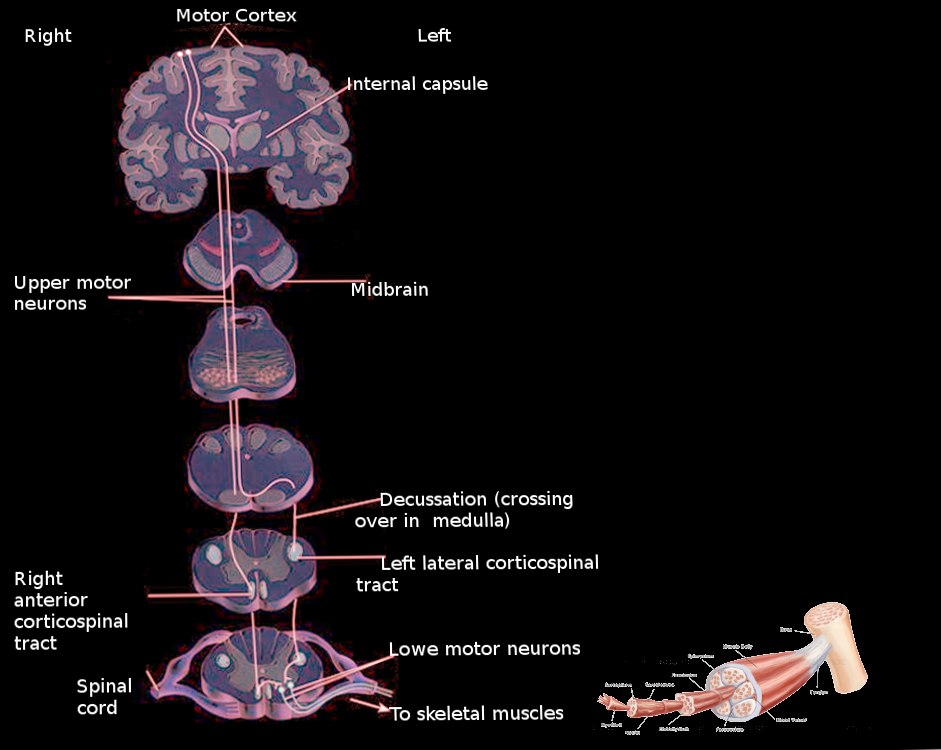
Upper motor neurons of the pyramidal tract have the majority of their cell bodies located in the precentral motor cortex (Brodmann area 4) and the premotor area (Brodmann area 6). Cell bodies are also present in the supplementary motor area, primary somatosensory cortex, and the superior parietal lobe. UMN axons radiate out into the corona radiata and converge at the posterior limb of the internal capsule. The pathway of the corticospinal tract descends through the cerebral peduncle in the midbrain, ventral pons, and the pyramids of the medulla. At the inferior aspect of the medulla, the majority of corticospinal tract axons decussate at the pyramidal decussation. The axons continue their descent contralateral from their cell bodies of origin and enter the spinal cord at the lateral funiculus. The tract is now the lateral corticospinal tract. The axons terminate throughout the spinal cord in the ventral gray column and the base of the dorsal column. The lateral corticospinal tract axons that control distal extremities synapse directly on lower motor neurons. These direct connections are presumed to be necessary for the fine control of the fingers and hands. The rest of the lateral corticospinal tract axons will synapse on premotor interneurons. At the pyramidal decussation, approximately 10% of the corticospinal tract axons do not decussate and continue their descent down the brain ipsilateral to their cell bodies of origin. These fibers enter the ventral aspect of the spinal cord and are known as the anterior corticospinal tract. As the fibers descend the spinal cord, most of them will decussate through the anterior white commissure before synapsing with interneurons. A small percentage of corticospinal axons will not decussate anywhere along their descent the brainstem or the spinal cord. These axons provide the impulses which control axial musculature necessary to maintain body posture.[3]
The corticobulbar tract fibers originate from the parts of the motor cortex that represent the face. The axons share a similar trajectory to the corticospinal tract descending through the corona radiata and the internal capsule. At the level of the brainstem, the axons will synapse with each cranial nerve nuclei at their respective levels. The upper motor neuron innervation of most cranial nerves is bilateral which means that each cranial nerve receives impulses from the left and right hemisphere. This bilateral innervation pertains to the muscles of the eyes, jaw, pharynx, upper face, larynx, and neck. Two exceptions to this rule are CN VII and XII. The control of tongue protrusion by CN XII and the control of the muscles of the lower face by CN VII only receive contralateral innervation from the pyramidal tract.[4]
Knowledge about the pathways of the pyramidal tracts is paramount to understanding the clinical presentation of UMN lesions. Lesions above or below the pyramidal decussation will have symptoms on different parts of the body. UMN lesions rostral to the pyramidal decussation will result in symptoms contralateral to the site of the lesion. For example, a unilateral lesion on the right corticospinal tract before the pyramidal decussation would cause weakness and spasticity of musculature on the left side of the body. UMN lesions caudal to the decussation will cause symptoms ipsilateral to the site of the lesion. This presentation would generally be with lesions to the spinal cord. For example, left-sided lesions of the corticospinal tract in the spinal cord will cause left-sided weakness and spasticity. Unilateral UMN lesions innervating cranial nerves do not manifest with clinically significant symptoms due to their bilateral innervation from the left and right motor areas. Hence, only bilateral lesions to the UMN of cranial nerves would create deficits. Lesions of UMN’s to CN VII and XII are the exceptions because of their unilateral innervation from contralateral motor areas. For example, a right-sided UMN lesion to the motor area that controls CN VII would manifest as a weakness on the left lower face.[5]
Surgical Considerations
The management of UMN lesions should focus on ascertaining the cause of the lesion. Indications for surgical treatment are in very few specific diagnoses such as intracranial aneurysms, hematomas, malignancies, or abscesses. The remainder of surgical management does not focus on the UMN lesions but instead on the sequelae of the damage such as spasticity and contractures. Prompt evaluation and a detailed history and physical exam are necessary to provide patients with optimal treatment of their lesions and symptoms. Upper motor neuron syndrome has a variety of long-lasting symptoms that can drastically affect a patient’s quality of life. The long-term management of patients with UMN syndrome includes extensive rehabilitation. Muscle spasticity can lead to abnormal postures and joint contractures in the long term. This would result in decreased angles of passive motion and thus reduced quality of life. Prevention of contractures is an essential goal in the management of patients recovering from UMN lesions. If conservative medical management and rehabilitation fail to decrease the spasticity and contractures, surgical intervention may be the proper course of management. Surgical management includes the lengthening of spastic muscles to enhance levels of function. The patients who are candidates for surgery can be stratified based on their volitional control of extremities. The goals of surgery are dependent on the functional potential of patients. Surgical management centers around the muscular pathology identified in surgical candidates. The muscular abnormalities that are surgical candidates include:
Shoulder adduction and internal rotation
Elbow flexion
Forearm pronation
Wrist and finger flexion
Hand intrinsics spasticity
Clenched fist deformity
Thumb-in-palm deformity
Inferior subluxation of the glenohumeral joint
After identification of the muscle pathology, the basis of surgical intervention is on whether a patient has volitional control. Patients with volitional control may undergo tendon fractional lengthening, muscle origin release, or a joint osteocapsular release. Patients that are found to have no volitional control may undergo muscle origin release, myotomy, tenotomy, neurectomy, arthrodesis, and joint osteocapsular release. The specific procedure used is based on the surgically targeted muscle and the goals of the procedure.[6]
Clinical Significance
UMN lesions can arise from a variety of injuries to the brain or spinal cord. These include cerebrovascular accidents, traumatic brain injury, anoxic brain injury, malignancy, infections, inflammatory disorders, neurodegenerative disorders, and metabolic disorders. The clinical manifestation of a UMN lesion is known as upper motor neuron syndrome. The symptoms of UMN damage require differentiation from damage to lower motor neurons which would manifest with weakness, muscle atrophy, hypotonia, hyporeflexia, fasciculations, and fibrillation.[7]
Upper Motor Neuron Syndrome
The symptoms of UMN syndrome can separate into negative and positive symptoms. Negative symptoms include weakness, decreased motor control, and easy fatigability. A unique characteristic of UMN syndrome is its tendency to affect specific muscle groups. The weakness caused by UMN syndrome will predominantly affect the extensors of the arm and flexors of the leg. Positive symptoms are those involving increased muscle activity. The symptoms can include:
Spasticity
The definition of spasticity is a velocity-dependent increase in a muscle’s resistance to a passive stretch. Slow passive movements of the arms or legs will not elicit the increased resistance. Brisk stretches of muscles will cause an abrupt increase in tone followed by a decrease in muscular resistance with continued stretch. This phenomenon is called clasp-knife rigidity. The antigravity muscles of the arms and legs are most affected. These include the flexors of the arms and the extensors of the leg. Because of the decreased modulation of spinal reflexes in UMN syndrome, patients will often exhibit flexor and extensor spasms.
Clonus
Clonus is a sequence of rhythmic, involuntary muscle contractions. These contractions occur at a frequency of 5 to 7 Hz and are a response to abruptly applied stretch stimuli. Clonus is most easily elicited at the ankle with brisk dorsiflexion and plantar-flexion movements. Clonus can also be observed during voluntary movement or through cutaneous stimulation.
Hyperreflexia of deep tendon reflexes
Patients can be seen to have abnormally brisk reflexes which are due to decreased modulation by descending inhibitory pathways. Radiation of reflexes is a regular observation with the hyperreflexia of UMN lesions. For example, tapping of the supra-patellar tendon would elicit a knee-jerk reflex.
Hyporeflexia of superficial reflexes
The superficial abdominal reflex and the cremasteric reflex are seen to be decreased or abolished following UMN lesions. The superficial abdominal reflex is the tensing of abdominal by stroking the overlying skin while the cremasteric reflex is the elevation of the scrotum in response to stroking the medial thigh.
Synkinesias
Synkinesias are involuntary movements in a limb that have associations with the voluntary movements in other limbs. For example, flexion of the arm may result in flexion of the leg. These involuntary movements can also occur with yawning or sneezing. Volitional movements of one arm or leg may also result in mirror movements of the opposite limb.
Co-Contraction
Co-contraction is defined as the simultaneous contraction of agonist and antagonist muscles around a joint. This increases the stiffness and stabilization around the joint which prepares it for activity in healthy individuals. The pathological co-contraction in UMN lesions causes a decreased rate of rapid alternating movements and creates greater fatigability for voluntary movements in weakened muscles.
Babinski Sign and other reflexes
The Babinski sign can be elicited by stroking the sole of the foot with a firm stimulus. The normal adult response is plantar-flexion. The sign is positive when the application of the stimulus elicits extension of the large toe and fanning of the other toes. The Babinski sign is known to be a normal response in infants before full maturation of the corticospinal tract. However, in adults, a positive sign is indicative of underlying UMN damage. Other reflexes exist which represent lesions of the corticospinal tract. The Brissaud reflex is linked with the extensor response of the Babinski sign and is positive when stroking the sole of the foot elicits contraction of the tensor fascia latae of the ipsilateral leg. The Hoffman sign is an analog of the Babinski reflex for the upper limbs. The test is performed by loosely holding the patient’s middle finger and quickly flicking the fingernail downward. A positive sign is the flexion and adduction of the thumb.[8]
Pseudo-Bulbar Palsy
As previously stated, most cranial nerves have bilateral innervation from the brain with the exception of CN VII and CN XII. The muscles of cranial nerves with bilateral innervation include the eyes, jaw, pharynx, upper face, larynx, and neck. These muscles would only show deficits with bilateral UMN lesions. Bilateral damage of UMN’s to cranial nerves is known as a pseudobulbar palsy. Slurred speech is often the first presenting symptom. Other characteristic deficits include dysphagia, dysarthria, brisk jaw jerk, spastic tongue, and pseudobulbar affect.[9]
CN VII and CN XII UMN lesions
CN VII and CN XII innervate muscles of the lower face and the tongue, respectively. These cranial nerves receive unilateral innervation from the pyramidal tract. Unilateral lesions of UMN’s to CN VII or CN XII would manifest as a lower facial droop or tongue deviation away from the side of the lesion, respectively.
Spinal Shock
Spinal shock refers to the period of acute flaccid paralysis following spinal cord injury. Hypotonia and hyporeflexia are the most characteristic symptoms. The paralysis is most evident in the arms and legs with the preservation of truncal musculature. The duration can range from a few days to weeks after which spasticity and hyperreflexia replace the prior symptoms. The symptoms of spinal shock are most pronounced with lesions of the spinal cord versus cerebral lesions.[10]
Other Issues
Detailed patient history and a complete physical exam are essential for differentiating the cause of UMN lesions. Some diseases that can damage upper motor neurons include cerebrovascular accidents, amyotrophic lateral sclerosis, primary lateral sclerosis, multiple sclerosis, Brown-Sequard Syndrome, vitamin B12 deficiency.
Cerebrovascular Accidents
Cerebrovascular accidents or strokes are the sudden cessations of blood flow to areas of the brain leading to cell death. Strokes fall into two etiologic categories, being either ischemic or hemorrhagic. Ischemic strokes are the sudden interruption of blood flow to the brain which can be due to thrombi, emboli, or compression. Hemorrhagic strokes are characterized by bleeding into the brain due to the rupture of a blood vessel. The cerebral blood supply has many branches which supply different areas of the brain. Occlusion of the middle cerebral artery or anterior cerebral artery can damage the motor areas of the cerebral cortex. Given the extensive areas of the brain supplied by the middle cerebral and anterior cerebral artery, strokes in those regions are likely to present with sensory, language, perceptual, and visual deficits in addition to UMN signs. Occlusion of the lenticulostriate arteries can damage the internal capsule. A stroke that targets the posterior limb of the internal capsule presents with pure motor deficits of the contralateral face, arm, and leg. Occlusion of the various branches of the vertebral artery or basilar artery can lead to strokes in different areas of the brainstem. Notable brainstem strokes that damage the corticospinal tract are medial medullary syndrome, medial pontine syndrome, and Weber Syndrome.[11]
Amyotrophic Lateral Sclerosis
Amyotrophic lateral sclerosis (ALS) is the most prevalent neurodegenerative disease that is characterized by its involvement of both upper and lower motor neurons. Hence, the clinical presentation is a combination of upper motor signs and lower motor neuron signs. Nerve conduction studies and electromyography are utilized to confirm the diagnosis. Labs are generally used to rule out other disease processes that can manifest with weakness in patients. ALS is currently incurable however various treatments have been developed to extend life in patients. Riluzole is a glutamate pathway antagonist that is the only current drug shown to extend life in patients with ALS.[12]
Primary Lateral Sclerosis
Primary lateral sclerosis (PLS) is a neurodegenerative disorder that targets upper motor neurons. PLS is generally seen in adults and is sporadic in nature, though hereditary variants have been observed. Compared to ALS, PLS has a slower progression and lacks lower motor neuron signs. However, some individuals with PLS do develop lower motor neuron signs as their disease progresses. The condition would then be considered upper motor neuron onset ALS. There are no cures for PLS and treatment is aimed at alleviating symptoms of spasticity and weakness through medications and physical therapy.[13]
Brown-Sequard Syndrome
Brown-Sequard Syndrome is a spinal cord lesion caused by a hemisection injury to the spinal cord. The most common etiology is from penetrating trauma to the spine. However, other etiologies include blunt trauma, hematoma, tumors, or disc herniation. As a result of the hemisection of the spinal cord, the symptoms are manifestations of damage to the lateral corticospinal tract, dorsal column, and the lateral spinothalamic tract. Patients present with upper motor neuron signs ipsilateral and below the level of the lesion. Patients will also present with ipsilateral loss of fine touch, vibration, and proprioception in addition to the contralateral loss of pain and temperature sensation.[14]
Multiple Sclerosis
Multiple Sclerosis (MS) is an immune-mediated, inflammatory demyelinating disease. The symptomatology of MS is characterized by episodes that occur in different anatomic locations in the central nervous system and occur months or years apart. The presenting symptoms of patients are highly variable. Symptoms can include cognitive disturbance, visual changes, hemiparesis, ataxia, and sensory deficits. The UMN signs of MS are due to the demyelination of upper motor neurons. MRI is the imaging test of choice used to diagnose MS. CSF studies may also be used to aid in diagnosis. Oligoclonal bands and intrathecal immunoglobulin G are classically seen in the CSF of MS patients.[15]
Vitamin B12 Deficiency
The most prevalent etiologies of vitamin B12 deficiency are pernicious anemia, bariatric surgery, small intestine surgery, and gastritis. Other etiologies include pancreatic insufficiency, inadequate dietary intake, and drug side effects. Vitamin B12 deficiency causes degeneration of the dorsal column and lateral white matter of the spinal cord. This can lead to degeneration of the lateral corticospinal tract with subsequent UMN signs. Degeneration of the dorsal column manifests as sensory ataxia. Deficiency also leads to macrocytic anemia. Supplementation with vitamin B12 generally corrects the anemia and stops the progression of the degeneration of the spinal cord.[16]
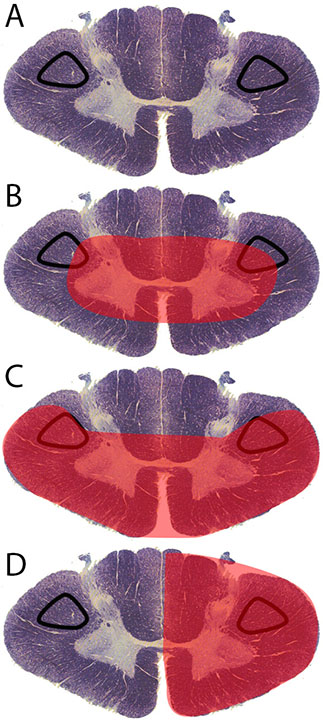
<p>Contributed by RS Menon, MD </p>
(Click Image to Enlarge)
Corticospinal Tract Lesion Locations. Corticospinal tract lesion locations: (A) normal spinal cord cross-section, (B) area affected by central cord syndrome, (C) area affected by anterior cord syndrome, (D) area affected by Brown-Sequard syndrome.
Jang SH. The corticospinal tract from the viewpoint of brain rehabilitation. Journal of rehabilitation medicine. 2014 Mar:46(3):193-9. doi: 10.2340/16501977-1782. Epub
[PubMed PMID: 24531325]
Dall'Orso S, Steinweg J, Allievi AG, Edwards AD, Burdet E, Arichi T. Somatotopic Mapping of the Developing Sensorimotor Cortex in the Preterm Human Brain. Cerebral cortex (New York, N.Y. : 1991). 2018 Jul 1:28(7):2507-2515. doi: 10.1093/cercor/bhy050. Epub
[PubMed PMID: 29901788]
Canedo A. [Functional heterogeneity of the piramidal system: corticobulbar and corticospinal tracts]. Revista de neurologia. 2003 Mar 1-15:36(5):438-52
[PubMed PMID: 12640598]
Rhee PC. Surgical Management of Upper Extremity Deformities in Patients With Upper Motor Neuron Syndrome. The Journal of hand surgery. 2019 Mar:44(3):223-235. doi: 10.1016/j.jhsa.2018.07.019. Epub 2018 Sep 25
[PubMed PMID: 30266480]
Mayer NH, Esquenazi A. Muscle overactivity and movement dysfunction in the upper motoneuron syndrome. Physical medicine and rehabilitation clinics of North America. 2003 Nov:14(4):855-83, vii-viii
[PubMed PMID: 14580042]
Damodaran O, Rizk E, Rodriguez J, Lee G. Cranial nerve assessment: a concise guide to clinical examination. Clinical anatomy (New York, N.Y.). 2014 Jan:27(1):25-30. doi: 10.1002/ca.22336. Epub 2013 Dec 5
[PubMed PMID: 24307604]
Chu J, Liu X, Chen F, Hong F, Bao Y. [Effects of GAO's neck acupuncture on swallowing function and quality of life in patients with post-stroke pseudobulbar palsy:a randomized controlled trial]. Zhongguo zhen jiu = Chinese acupuncture & moxibustion. 2017 Jul 12:37(7):691-695. doi: 10.13703/j.0255-2930.2017.07.003. Epub
[PubMed PMID: 29231539]
Hiersemenzel LP, Curt A, Dietz V. From spinal shock to spasticity: neuronal adaptations to a spinal cord injury. Neurology. 2000 Apr 25:54(8):1574-82
[PubMed PMID: 10762496]
Lee SJ, Lee DG, Moon HJ, Lee TK. Lesion Pattern, Mechanisms, and Long-Term Prognosis in Patients with Monoparetic Stroke: A Comparison with Nonmonoparetic Stroke. BioMed research international. 2017:2017():9373817. doi: 10.1155/2017/9373817. Epub 2017 Sep 12
[PubMed PMID: 29138753]
de Carvalho M, Poliakov A, Tavares C, Swash M. Interplay of upper and lower motor neuron degeneration in amyotrophic lateral sclerosis. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2017 Nov:128(11):2200-2204. doi: 10.1016/j.clinph.2017.08.024. Epub 2017 Sep 19
[PubMed PMID: 28957737]
Le Forestier N, Meininger V. [Primary lateral sclerosis: the era of international diagnosis criteria]. Revue neurologique. 2009 May:165(5):415-29. doi: 10.1016/j.neurol.2008.07.022. Epub 2008 Oct 7
[PubMed PMID: 18842276]
Zeng Y, Ren H, Wan J, Lu J, Zhong F, Deng S. Cervical disc herniation causing Brown-Sequard syndrome: Case report and review of literature (CARE-compliant). Medicine. 2018 Sep:97(37):e12377. doi: 10.1097/MD.0000000000012377. Epub
[PubMed PMID: 30213001]
Langan RC, Goodbred AJ. Vitamin B12 Deficiency: Recognition and Management. American family physician. 2017 Sep 15:96(6):384-389
[PubMed PMID: 28925645]
Use the mouse wheel to zoom in and out, click and drag to pan the image