Continuing Education Activity
The most important step in the initial evaluation of any pregnant patient is establishing an accurate delivery date (due date). Accurate knowledge of the gestational age is important for numerous reasons. A patient's gestational age determines the appropriate intervals for prenatal care visits, as well as the timing of certain interventions. This activity describes the different methods to date a pregnancy.
Objectives:
Identify the technique of performing a transvaginal ultrasound for pregnancy dating.
Describe the indications for dating a pregnancy.
Review the clinical significance of dating a pregnancy.
Outline interprofessional team strategies for improving pregnancy dating and improving patient outcomes.
Introduction
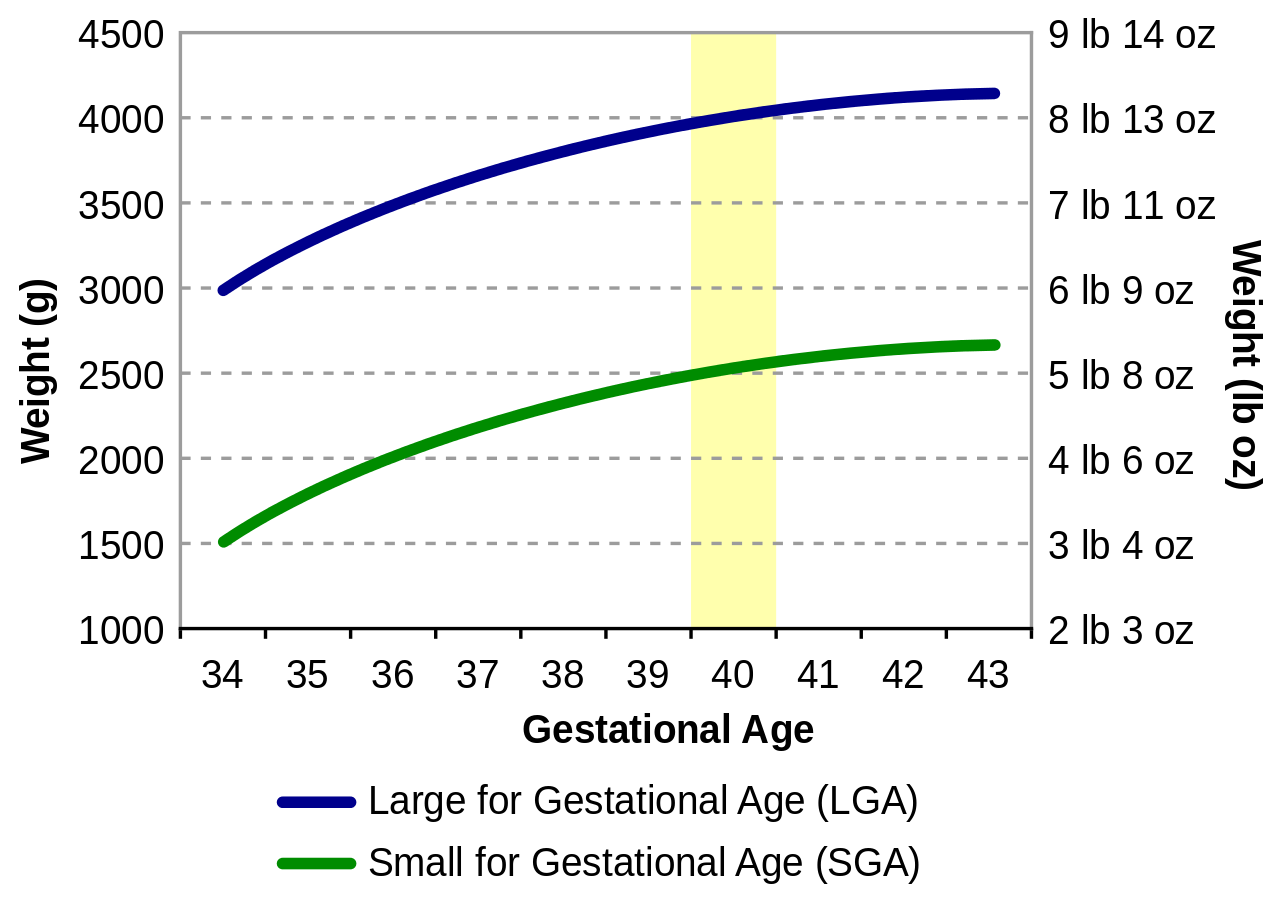
The most important step in the initial evaluation of any pregnant patient is establishing an accurate delivery date or due date (see Image. Pregnancy Timeline). Accurate knowledge of gestational age is important for numerous reasons. A patient's gestational age determines the appropriate intervals for prenatal care visits and the timing of certain interventions (see Image. Birth Weight for Gestational Age Chart). For example, certain antenatal screening tests like the quadruple marker screen (screening test for fetal aneuploidy and open neural tube defects) must be performed with accurate knowledge of the gestational age to accurately calculate lab values. In patients with a history of preterm labor and delivery, screening tests and interventions early in pregnancy can be used to prevent preterm labor in any subsequent pregnancy. As pregnancy progresses, accurate and optimal pregnancy dating is important when deciding on the timing of both medically indicated and elective deliveries.[1]
Anatomy and Physiology
Pregnancy ultrasound involves an anatomic survey of the uterus and adnexa. On the initial ultrasound, it is important to establish the location of the gestational sac, confirm the intrauterine location, and document the presence or absence of the yolk sac, fetal pole, and fetal number. If a fetal pole is seen, the presence of fetal heart tones should be documented. A full fetal anatomic survey is possible if ultrasound is performed beyond 18 weeks of gestation.[2]
Indications
For appropriate management of any pregnancy, practitioners must establish gestational age. All pregnancies should have either abdominal or transvaginal ultrasound to confirm or establish a gestational age before 22 0/7 weeks.[1] Any pregnancy that does not meet this criterion should be considered suboptimally dated.[3]
Contraindications
Ultrasound has been used in obstetrics for over 50 years and is safe when used appropriately.[2] Energy used to obtain ultrasound images does have an effect on tissue. For this reason, ultrasound should only be used when clinically indicated and for the shortest possible time.[4]
Equipment
When using the patient's last menstrual period to establish pregnancy dating, Naegele's rule requires the use of a calendar. Ultrasound is the most reliable method to establish pregnancy dating, particularly first-trimester ultrasound.[1] Transvaginal ultrasound utilizes a 6-MHz to 10-MHz ultrasound probe. This probe has a higher frequency than transabdominal ultrasound probes, which can show intrauterine structures approximately 1 week earlier in gestation. Beyond 8 weeks, transabdominal ultrasound is typically satisfactory for the evaluation of pregnancy. Transabdominal ultrasound utilizes a curvilinear ultrasound probe with a frequency of 3 MHz to 6 MHz, which provides good penetration into the uterus. Abdominal obesity or a retroverted uterus may cause difficulty during the transabdominal approach. Both transabdominal and transvaginal approaches require the use of an acoustic gel.[4]
Personnel
A physician typically selects the appropriate estimated delivery date for a pregnant patient. In certain circumstances, an ultrasound technician is the first person to evaluate a pregnancy using ultrasound. Ultrasound-reported estimated date of delivery, as well as other dating methods, should be compared by the treating clinician to choose the best clinical estimate of gestational age using the rules described below.[1]
Preparation
Patient preparation before ultrasound varies depending on which approach is used. For transabdominal ultrasound, a full bladder is helpful but not required. For a transvaginal ultrasound, a full bladder can displace the uterus posteriorly and out of the field of view of the transvaginal ultrasound probe. For this reason, it is recommended to perform a transvaginal ultrasound with an empty bladder.[4]
An abdominal ultrasound approach may be performed in the supine position. The transvaginal approach should be performed with the patient in the lithotomy position, with the patient's buttocks at the end of the table, allowing for a complete range of motion with the transvaginal ultrasound probe.[4]
Technique or Treatment
One method of estimating the delivery date is by using the patient's last menstrual cycle. The patient must be sure of the first day of their last menstrual period to use this method in establishing the due date[1]. Adding 7 days and then 9 months to the patient's last menstrual period (or 280 days) gives an estimated delivery date. This technique assumes that the patient has a normal 28-day menstrual cycle and ovulates on day 14 of that cycle.[1]
Fundal height measurement is a physical exam parameter that can be used to estimate gestational age. The distance from the uterine fundus to the pubic symphysis defines fundal height measurement. Measurement should be performed using a nonelastic tape measure, and the patient should have an empty bladder. The most common use for fundal height measurement is recording the trend of this measurement to screen for appropriate fetal growth throughout gestation. The usefulness of fundal height measurement in any circumstance has varied widely throughout the literature but can be helpful in resource-poor areas for an estimation of gestational age. The assumption with fundal height measurement is that the measurement in centimeters from the uterine fundus to pubic symphysis is equal to the patient's gestational age. Uterine fibroids, amniotic fluid abnormalities, increased maternal body mass index, and fetal growth abnormalities are some examples of circumstances that can alter the accuracy of fundal height measurement.[5]
First-trimester ultrasound (ultrasound before 13 weeks and 6/7 days) is the most accurate method to establish or confirm gestation age in pregnancy. First-trimester ultrasound can be performed either trans-vaginally or trans-abdominally. Crown-rump length is used for pregnancy dating the first trimester. The average of 3 crown-rump length measurements is used to improve accuracy. When the crown-rump length exceeds 84 mm (approximately 14 weeks and 0/7 days), the accuracy decreases, and full fetal biometry should be used to approximate the gestational age. First-trimester ultrasound has an accuracy of +/- 5 to 7 days. The last menstrual cycle, if known, should be used to estimate the gestational age before an ultrasound. If the ultrasound is performed at less than 9 0/7 weeks, and the ultrasound dating differs by less than or equal to 5 days, the last menstrual period should be used for gestational age determination. If the estimated delivery date in this circumstance differs by more than 5 days, the ultrasound-determined estimated delivery date should be used. An ultrasound performed between 9 0/7 weeks and 13 6/7 weeks can differ by 7 days. If the ultrasound-determined estimated delivery date differs by more than 7 days, the ultrasound-estimated delivery date should be used. If the ultrasound-estimated delivery date varies by less than 7 days, the last menstrual period should be used.[1]
The performance of a first-trimester ultrasound is not always possible. Patients occasionally initiate prenatal care in the second trimester or may not present to a facility with ultrasound capability. An initial ultrasound should be performed between 18 to 20 weeks in resource-poor areas. Ultrasound between 18 to 20 weeks allows both optimal dating criteria and a detailed anatomical survey of the fetus.[2] Second-trimester ultrasound estimates the delivery date with fetal measurements of biparietal diameter, head circumference, abdominal circumference, and femur length.[1]
The accuracy of second-trimester ultrasound (between 14 0/7 weeks and 27 6/7 weeks) is widely variable. The earlier in the second trimester an ultrasound is performed, the more accurate the gestational age measurement is.[2] Suppose a first-trimester ultrasound has been used to confirm or establish an estimated date of delivery. In that case, a second-trimester ultrasound should not be used to adjust the estimated date of delivery. If an ultrasound is performed between 14 0/7 and 15 6/7 weeks and the date of delivery as estimated by the last menstrual period differs by more than 7 days, the ultrasound-estimated delivery date should be used for pregnancy management. If an ultrasound is performed between 16 0/7 and 21 6/7 weeks and the estimated date of delivery by the last menstrual period differs by more than 10 days, the ultrasound-estimated date of delivery should be used.[1] Pregnancies without confirmation or revision of gestational age by ultrasound before 22 0/7 weeks are considered suboptimally dated.[3] Beyond 22 0/7 weeks until 27 6/7 weeks, if the last menstrual period-determined estimated delivery date differs by more than 14 days, the ultrasound estimated delivery date should be used.[1]
Third-trimester ultrasound (beyond 28 0/7 weeks) is the most inaccurate method for pregnancy dating, with an accuracy of +/- 21 to 30 days.[1] One primary concern with third-trimester dating ultrasound is underestimating the gestational age of a growth-restricted fetus.[1] Management decisions based on third-trimester ultrasound alone can be difficult for this reason[1].
Complications
Once the estimated delivery date is established and confirmed with first or second-trimester ultrasound, it should be carefully documented in the medical record for use by other health care providers if needed. Changes to the estimated delivery date can have significant implications for pregnancy management, so before making a change to the patient's epatient'sdelivery date, the patient should be counseled on possible implications.[1]
Clinical Significance
Establishing an accurate gestational age and estimated delivery date is the most important step in managing any pregnancy.[1] Accurate knowledge of gestational age allows laboratory and screening tests to be performed at the appropriate time in the pregnancy.[1] Optimal dating before 22 0/7 weeks enables an accurate assessment of fetal growth as the pregnancy progresses. Suboptimally dated pregnancies, due to the error of ultrasound at advanced gestational age, can be difficult to manage because of the uncertainty of pregnancy dating. Elective delivery should not be performed in suboptimally dated pregnancies. In pregnancies with clear medical indications for delivery (pre-eclampsia, gestational diabetes, etc), delivery planning should be based on the best clinical estimation of gestational age. Amniocentesis for fetal lung maturity should not be used routinely before planning delivery for sub-optimally dated pregnancy. Even with proven fetal lung maturity, late preterm and early-term infants have an increased risk of respiratory morbidity. Elective delivery should be performed at 41 completed weeks due to concerns that the fetus could be further along than estimated by third-trimester ultrasound. Antepartum fetal testing can be performed after 39 weeks in patients with sub-optimal dating due to concerns for post-term pregnancy.[3] In a sub-optimally dated pregnancy, a repeat low transverse cesarean delivery, if desired by the patient, should be performed at 39 weeks based on the best estimate of gestational age.[1][6][7][8][9]
Enhancing Healthcare Team Outcomes
Pregnancy is dated by the clinician. Establishing an accurate gestational age and estimated delivery date is the most important step in managing any pregnancy. Accurate knowledge of gestational age allows laboratory and screening tests to be performed at the appropriate time in the pregnancy.[1] Optimal dating allows one to follow the pregnancy, anticipate any difficulties, and predict the day of delivery. The more prepared the pregnancy team is, the better the outcomes.[10]