Continuing Education Activity
Acne conglobata (AC) is a rare but severe form of nodulocystic acne. It usually presents with tender, disfiguring, double or triple interconnecting comedones, cysts, inflammatory nodules, and deep burrowing abscesses on the face, shoulders, back, chest, upper arms, buttocks, and thighs. The comedones often occur in groups of three, and the cysts often contain purulent, foul-smelling material that is discharged on the skin surface. It is a chronic inflammatory disease that inevitably leads to scar formation and disfigurement. Acne conglobata may occur following the sudden worsening of pustular acne, or the disorder may occur gradually following the recrudescence of acne that has been quiet for many years.[2][3][4] This activity reviews the evaluation and management of acne conglobata and highlights the role of the interprofessional team in evaluating and improving care for patients with this condition.
Objectives:
- Describe how acne conglobata differs from acne fulminans.
- Explain the etiology of acne conglobata.
- Outline the treatment of choice for acne conglobata.
- Identify strategies that interprofessional team members can utilize to improve evaluation, management, and counseling for patients with acne conglobata.
Introduction
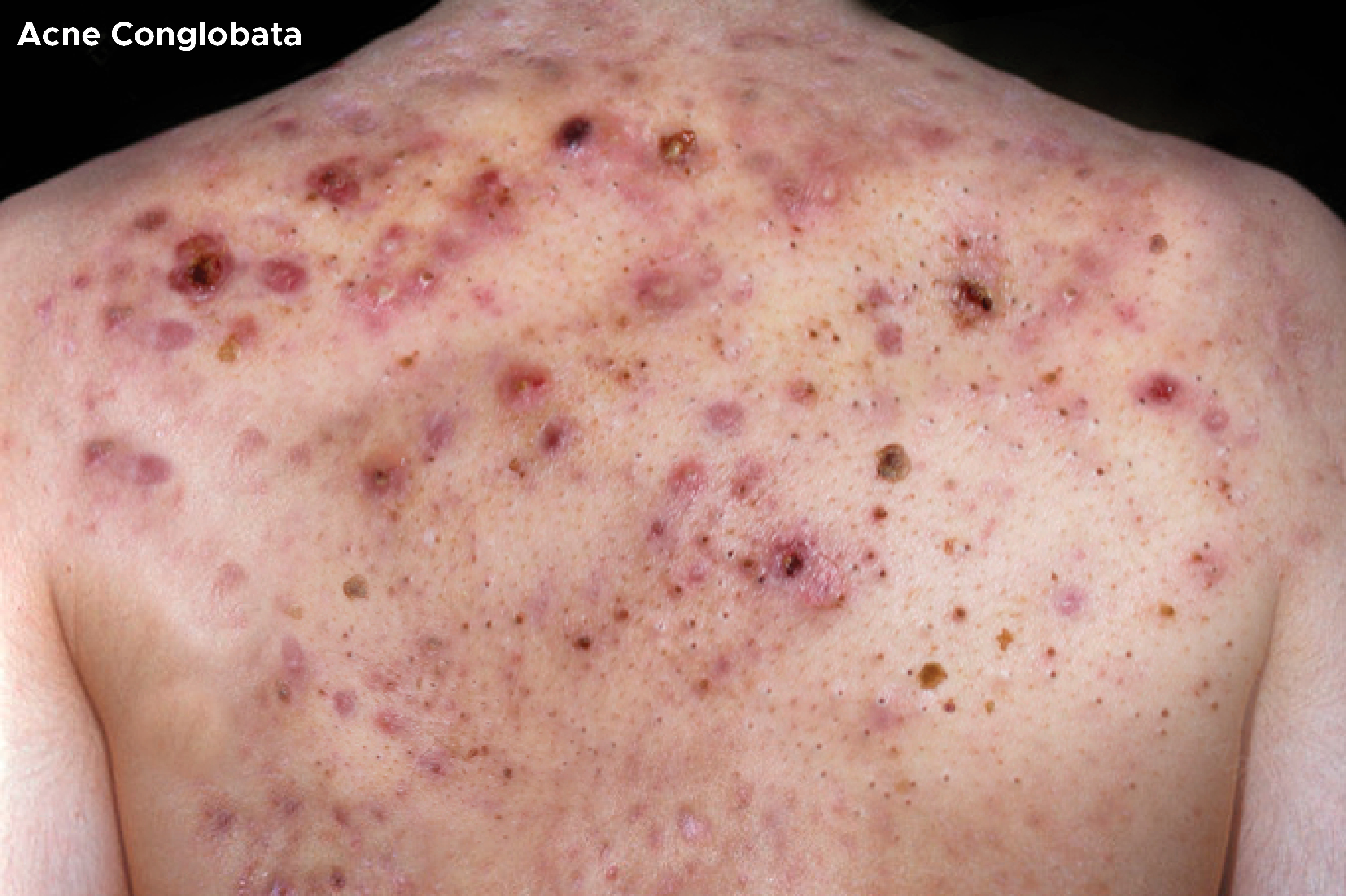
Acne conglobata (AC) is a rare but severe form of nodulocystic acne. It usually presents with tender, disfiguring, double or triple interconnecting comedones, cysts, inflammatory nodules, and deep burrowing abscesses on the face, shoulders, back, chest, upper arms, buttocks, and thighs. The comedones often occur in groups of three, and the cysts often contain purulent, foul-smelling material that is discharged on the skin surface. It is a chronic inflammatory disease that inevitably leads to scar formation and disfigurement.[1] Acne conglobata may occur following the sudden worsening of pustular acne, or the disorder may occur gradually following the recrudescence of acne that has been quiet for many years.[2][3][4]
Acne conglobata is part of the follicular occlusion tetrad, a group of related diseases involving dysfunction of the follicular unit, including dissecting cellulitis, pilonidal disease, and hidradenitis suppurativa (HS). The follicular occlusion tetrad can be exceptionally difficult to treat. Whereas ordinary acne vulgaris can typically be managed with topical agents, AC requires aggressive treatment due to the degree of inflammation and formation of deep nodules and cysts.[1]
Acne conglobata may occur in isolation or present with a systemic inflammatory condition, including SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis), PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum, acne), PASH syndrome (pyoderma gangrenosum, acne, suppurative hidradenitis), or PAPASH syndrome (pyogenic arthritis, pyoderma gangrenosum, acne, suppurative hidradenitis).[5] The sudden onset of severe acne with oozing and ulcerative lesions in relation to these syndromes or with respect to isotretinoin use is called acne fulminans, an immunologically induced systemic inflammatory response that may have accompanying fevers, malaise, and weight loss. Acne fulminans may arise from pre-existing AC lesions in a patient or may arise entirely de novo after initiation of isotretinoin therapy or concerning anabolic steroid use.[1]
Etiology
The etiology of acne involves the interplay of multiple factors, including follicular hyperkeratinization, hormonally-induced sebum production, and inflammation. The gram-positive microaerophilic/anaerobic rod called Cutibacterium acnes (formerly Propionibacterium acnes) is a commensal organism of the skin found deep within the sebaceous follicle and mediates a portion of the inflammatory component.[6]
The precursor of all acne lesions is the microcomedo. Increased follicular keratinocyte proliferation and cohesiveness lead to the accumulation of keratinocytes within the upper portion of the hair follicle rather than being shed and extruded as normal. This creates a follicular plug and bottleneck behind which additional keratinocytes and sebum build up within the follicle. Further accumulation of keratin and sebum leads to the formation of a comedo which develops into an inflammatory papule. Rupture of the follicular wall leads to intense inflammation and the formation of a nodule or cyst. Acne conglobata lies at the extreme end of the acne spectrum with many interconnecting comedones, cysts, inflammatory nodules, and draining sinus tracts. These can frequently become secondarily infected.[7]
Sebaceous glands are controlled principally by androgens such as testosterone, 5a-dihydrotestosterone (DHT), and dehydroepiandrosterone (DHEA). Receptors for these hormones are found in the cells of the sebaceous gland and outer root sheath of the hair follicle, and increased levels of circulating hormones seen with the onset of puberty lead to a rise in sebum production.[8] Persons with acne tend to have higher production of sebum overall as well as a different composition of the sebum they produce. They have higher levels of squalene, which form oxidative products, and lower levels of linoleic acid, the reduction of which predisposes to comedo formation and increased epidermal permeability by inflammatory substances.[9]
The role of Cutibacterium acnes in the pathogenesis of acne vulgaris has been under much study in recent years. Previously, it was believed that an overgrowth of C. acnes led to acne formation, but studies have found that the quantity of C. acnes on the skin is no difference between those with acne and those without.[6] Rather, research suggests that the specific strain or subtype of C. acnes prevalent in the follicles mediates the inflammatory response in acne formation. Subtypes II and III are believed to play a protective role in the normal microbiome of the skin, but Subtype I appears to be pathogenic when out of balance with the other two subtypes.[10][11] Individuals who develop acne conglobata likely have significant dysbiosis and an inflammatory reaction to Subtype I above and beyond that normally seen in acne-prone skin, although the specific reason for that is unknown.[12][13][14]
Ingestion of thyroid medication and exposure to halogenated aromatic hydrocarbons may trigger acne conglobata. Other factors that can provoke acne conglobata include androgens (e.g., androgen-producing tumors) and anabolic steroids.[1]
Acne conglobata has also been reported to occur in individuals who stop anabolic hormones or as a reaction to other hormonal agents.
Some people with acne conglobata have the XYY karyotype.
Epidemiology
Acne conglobata is not very common. Overall, it is more common in men than women. Over the past 30 years, many reports have been published on athletes with this type of acne, which is felt to be primarily due to the use of anabolic steroids. Outside the US, not much is known about acne conglobata. The condition is usually seen in young adults and very rarely seen in children or older adults. The onset is usually in the second and third decades of life. Whether it occurs more frequently in any specific race is not known.[15]
Pathophysiology
Acne conglobata presents with deep burrowing abscesses that interconnect with each other via sinus tracts. Initially, the nodular lesion may mimic a pimple, but underneath there is a vigorous inflammatory reaction and pus formation. Over time, the pus pushes into the adjacent tissues and extrudes on the skin's surface. Scar formation and disfigurement of the body are common with this type of acne. The comedones often occur in groups of three, and the cysts often contain purulent, foul-smelling material discharged on the skin surface.
History and Physical
Acne conglobata is a rare but severe form of nodulocystic acne. It usually presents with tender, disfiguring, double or triple interconnecting comedones, cysts, inflammatory nodules, and deep burrowing abscesses on the face, shoulders, back, chest, upper arms, buttocks, and thighs. The comedones often occur in groups of three, and the cysts often contain purulent, foul-smelling material that is discharged on the skin surface. It is a chronic inflammatory disease that inevitably leads to scar formation and disfigurement. Acne conglobata may occur following the sudden worsening of pustular acne, or the disorder may occur gradually following the recrudescence of acne that has been quiet for many years.
A physical exam will usually reveal a severe form of acne. The nodular lesions are tender and dome-shaped. When the nodules have broken down, there will be the presence of discharge that is foul-smelling pus. After the pus has drained, crusting of the lesion is common, followed by the formation of large irregular scars.
A classic feature of the disorder is the presence of paired or aggregates of blackheads on the trunk, neck, upper arms, and buttocks.
Acne conglobata may follow the use of androgenic anabolic steroids and is quite common in bodybuilders. Many young adult males will present to the dermatology clinic complaining of severe acne and facial scars. It is important to seek a thorough history of the use of anabolic steroids because discontinuation of these agents is vital for treatment.
Acne conglobata may also occur in patients with hidradenitis suppurativa and pyoderma gangrenosum. When the condition develops following puberty, the nodules will gradually coalesce and increase in severity over the ensuing years. Active nodule formation usually persists for the first three decades of life and then becomes quiescent.
Evaluation
The diagnosis is made clinically, and the discharge should be cultured. Appropriate antibiotics should be started in the presence of putrid discharge, as discussed below (e.g., minocycline or doxycycline). One should not wait for culture results before starting antibiotic therapy.
Treatment / Management
The treatment of choice for acne conglobata is using retinoids like isotretinoin for 20 to 28 weeks or, in some cases, even longer. Consider adding oral prednisone (1 mg/kg/d) for 14 to 28 days upon starting isotretinoin. Steroids have been shown to be effective if acne flares during the initiation of isotretinoin or when there are systemic constitutional symptoms. The sudden onset of severe acne with oozing and ulceration in relation to isotretinoin use is called acne fulminans, an immunologically induced systemic response that may have accompanying fevers, malaise, anorexia, and weight loss. In such cases, isotretinoin should be temporarily stopped while prednisone is used for 2 to 4 weeks, then isotretinoin can be restarted slowly (0.1 mg/kg/day) while continuing prednisone an additional four weeks, after which isotretinoin is tapered up while prednisone is tapered down.[16][17]
Topical retinoids are not as effective as oral retinoids but can be used adjunctively. It is important not to administer retinoids to women of childbearing age in the absence of effective contraception, as these drugs are known to be teratogenic.[18][19]
- Other options include the use of minocycline or doxycycline at 100 mg twice daily. These tetracyclines should not be combined with oral isotretinoin because there is a potential to induce pseudotumor cerebri.[1]
- Dapsone dosed at 50 to 150 mg daily is an option if unresponsive, although care must be taken with lab monitoring for methemoglobinemia, G6PD deficiency, and agranulocytosis.[20]
- Therapy with TNF-alpha inhibitors infliximab, adalimumab, and etanercept is supported in some case reports. These may be particularly helpful when acne conglobata arises as part of the follicular occlusion tetrad.[18]
- Laser therapy with fractional and ablative carbon dioxide laser, Nd:YAG, and vascular laser has shown efficacy in a few case reports.[21]
- In severe cases of acne conglobata that do not respond to the above treatments, another option is external beam radiation.[22]
Surgery
- When nodules are large and fluctuant, they can be aspirated. Sometimes providers may use cryotherapy or intralesional triamcinolone. The large nodules can also be excised surgically.
- Once the lesions have healed, dermal fillers can be used to improve the scars. In 2015 the FDA approved using the bovine collagen filler to treat acne scarring. Other dermal fillers and biostimulators can be used as well.
Differential Diagnosis
The differential diagnoses of acne conglobata include but are not limited to the following:
- SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis)
- PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum, acne)
- PASH syndrome (pyoderma gangrenosum, acne, suppurative hidradenitis)
- PAPASH syndrome (pyogenic arthritis, pyoderma gangrenosum, acne, suppurative hidradenitis)
- Acne fulminans
- Acne vulgaris
- Acneiform papulonodules
- Bromoderma
- Iododerma
- Rosacea fulminans
Prognosis
Acne conglobata can produce marked disfigurement. Severe scarring causes psychological impairment; individuals with acne conglobata often feel excluded. Acne conglobata has also been responsible for anxiety and depression in many patients.
Complications
Most patients with acne conglobata are shy and embarrassed about their skin condition. Many give a history of being withdrawn and isolated. Suicidal ideations are also common in this population. Thus, it is vital to offer them mental health counseling and referral to their primary care physician or psychiatrist to manage depression.
Deterrence and Patient Education
Once the diagnosis of acne conglobata is made, these individuals should receive psychological counseling because of depression and anxiety resulting from body disfigurement. The tendency is for these patients to hide the body disfigurement and skin lesions with garments, often leading to excess warmth and humidity, which worsens the skin condition. Hence, patient education on skin hygiene and counseling is recommended.
Enhancing Healthcare Team Outcomes
Patients with acne usually present to their primary care provider. But these clinicians should be aware that there are types of acne that are very serious and need an appropriate consult with a dermatologist. Acne conglobata is best managed by a dermatologist leading an interprofessional team that also includes nurses and pharmacists, as it requires more aggressive therapy with close follow-up.
In patients with acne conglobata, significant disfigurement is common, and the scarring often results in psychological impairment and social isolation. Many people with acne conglobata develop depression and anxiety. Once the diagnosis is made, these individuals should receive psychological counseling. The tendency is for these patients to hide the body disfigurement and skin lesions with garments, often leading to excess warmth and humidity, which worsens the skin condition. Hence, clinicians and nurses should educate the patient on skin hygiene and recommend counseling. In more severe cases, starting these patients on antidepressants and anti-anxiety medications can also be helpful.[23] [Level 5]